Anatomy
Distal femur physis
- fuses 14 in girls / 16 in boys
- 70% of growth of femur
- 40% of growth of lower limb
- 1 cm per year
Physis has three main undulatations
Epidemiology
Average age 10 - 11 years
Falls / MVA
NAI - distal femur fractures prior to walking
Associated injuries
Growth arrest
Basener et al J Orthop Trauma 2009
- systematic review of 564 distal femur growth plate fractures
- growth disturbance: 65% displaced fractures / 31% non displaced fractures
- growth disturbance: 36% SHI, 58% in SHII, 49% SHIII, and 64% SHIV
Vascular injury
Common peroneal nerve injury
ACL injury
Types
Distal femur fractures not involving physis
Growth plate fractures - Salter Harris Type II most common 60%


Salter Harris Type I
Salter Harris Type II



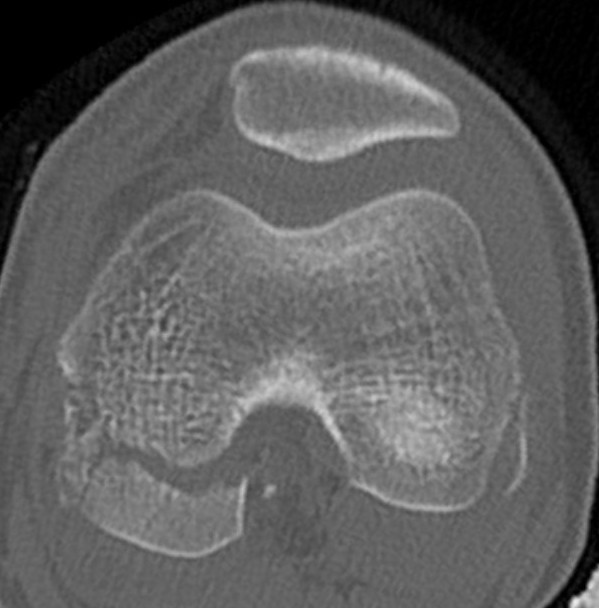
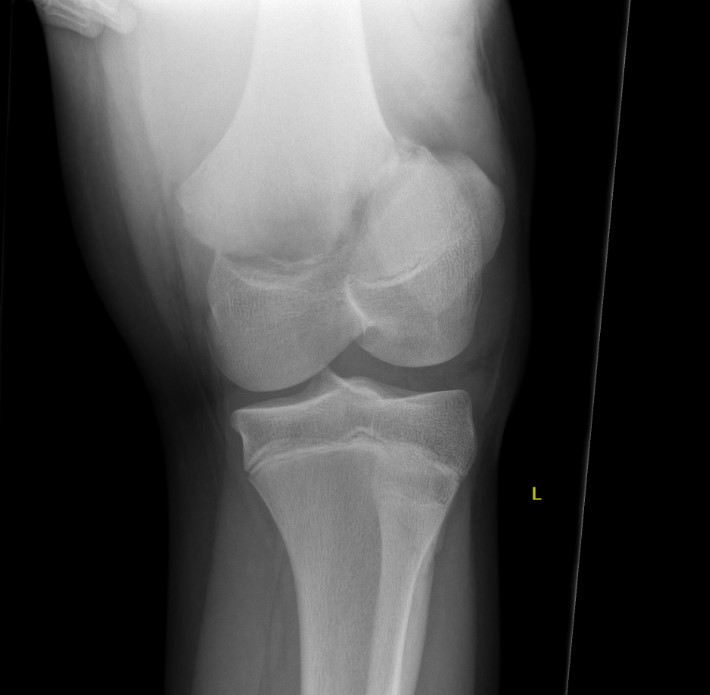
Salter Harris Type III
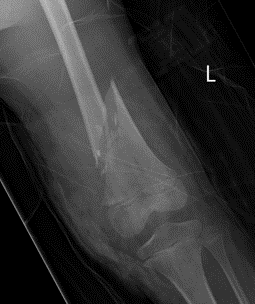

Supracondylar distal femur fracture


Supracondylar distal femur fracture through cyst

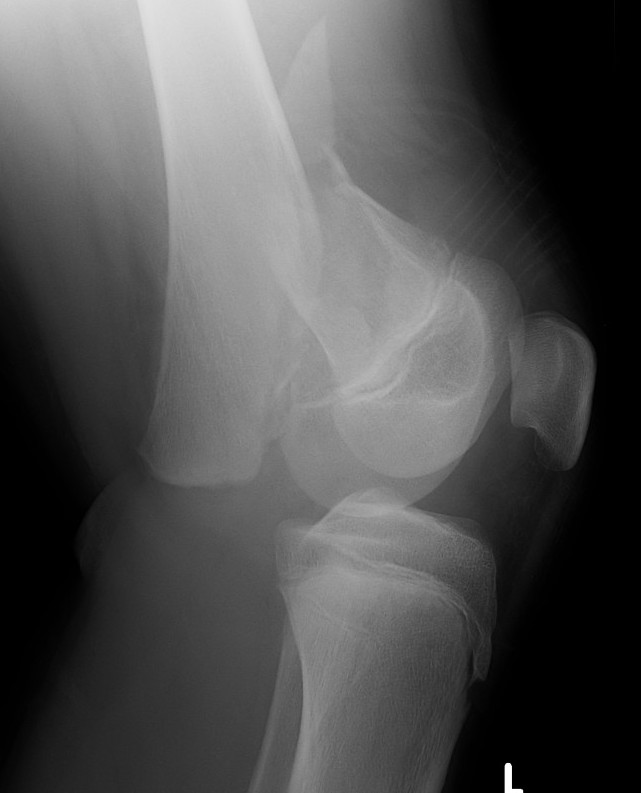
Pediatric Hoffa fracture
Management
Undisplaced
Extension plaster 6 weeks
Salter Harris Type I / Type II with minimal metaphyseal bone


Technique
AO foundation K wire fixation distal femur Salter-Harris Type I
AO foundation medial approach to pediatric knee
AO foundation lateral approach to pediatric knee
Closed reduction
- periosteum can cause block to reduction
- may require medial or lateral approach
Cross K wires
- can be unstable and lose position
- in children 4 and less the femoral artery can be in danger with medial K wire

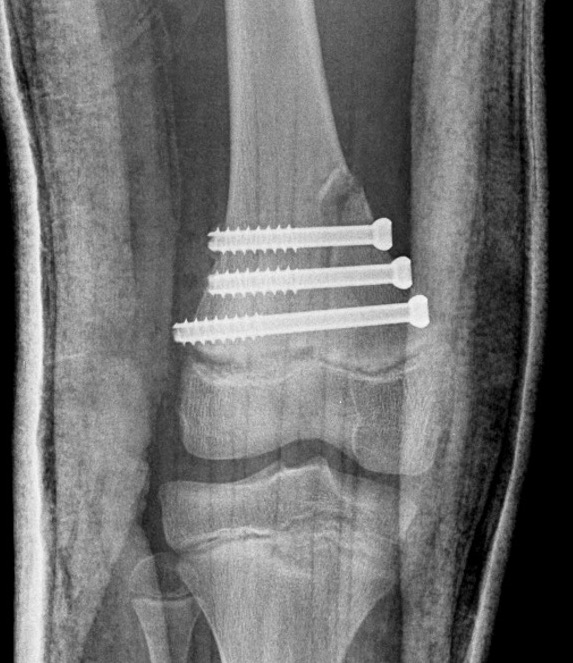
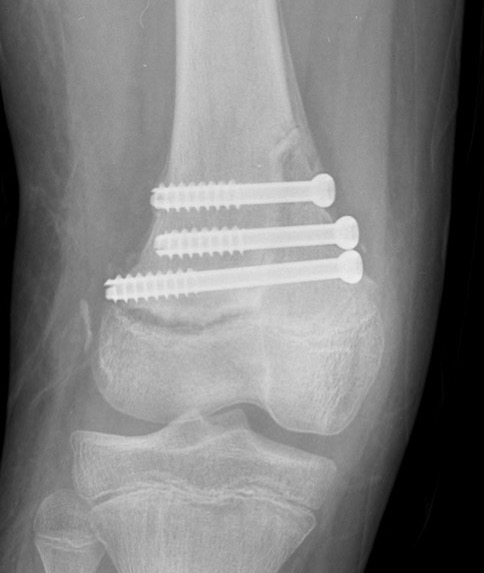
Salter Harris Type II with large Thurston Holland fragement

Technique
AO foundation screw fixation Salter Harris Type II
AO foundation medial approach to pediatric knee
AO foundation lateral approach to pediatric knee
Reduction
- attempt closed
- may be periosteum blocked on tension / medial side
Medial subvastus approach to knee
- identify Thurston-Holland fragment
- physeal sparing metaphyseal screws



Salter Harris Type III


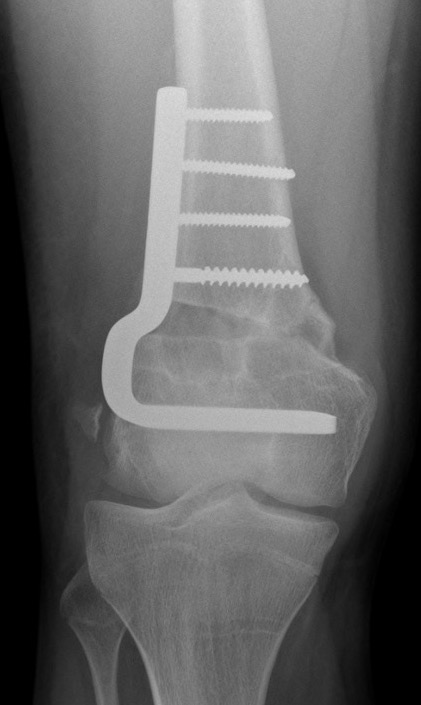
Supracondylar without physeal involvement

Plate fixation and currettage / bone grafting of cyst
Options
Plate
Antegrade flexible nails


Complications
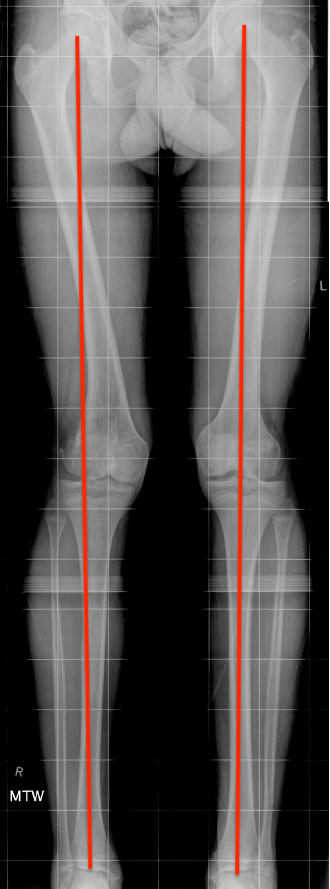
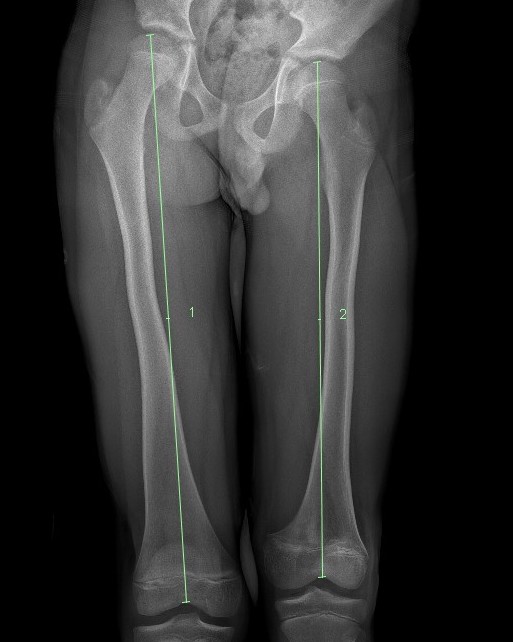
Complete growth arrest / Leg length discrepancy

Monitor 6 monthly
- plot short and long leg lengths on Mosely chart
- distal femur contributes 9 mm / year

Manage LLD as per predicted difference
- contralateral femoral epiphysiodesis +/- femoral lengthening
www.boneschool.com/pediatrics/leg-length-discrepancy
Partial growth arrest / angular deformity

Management
CT / MRI - assess percentage of bony bridge
Bony bridge < 50%
- excision and fat graft
- manage angular deformity with 8 plates / osteotomy
Bony bridge > 50%
- hemi-epiphysiodesis
- may need later correction of LLD and angular deformity