xrays
Metacarpal Fractures
Fractures
1. Neck of 5th Metacarpal
2. Metacarpal Shaft
3. Metacarpal Head
4. Base of Metacarpal Fracture Dislocations
5. Base of Thumb Fractures / Bennett's / Rolanda
1. Neck of 5th Metacarpal Fracture
Non operative Management
Accept 45o angulation
- will have finger extensor lag, but will recover
Ulna collateral ligament injury
Aetiology
Throwing injury
- seen in the throwing athlete
- repetitive microtrauma / valgus stress
- develop laxity
History
Initially
- lose velocity / accuracy
Develop medial pain
40% ulna nerve symptoms
Background
Aetiology
Intrinsic
- inflammatory
- degenerative
Extrinsic
- traumatic
- spur
Epidemiology
F > 40
Associations 60% of cases
- hypertension
- diabetes
- obese
- trauma
- prior surgery
- steroids
Ankle Arthroplasty

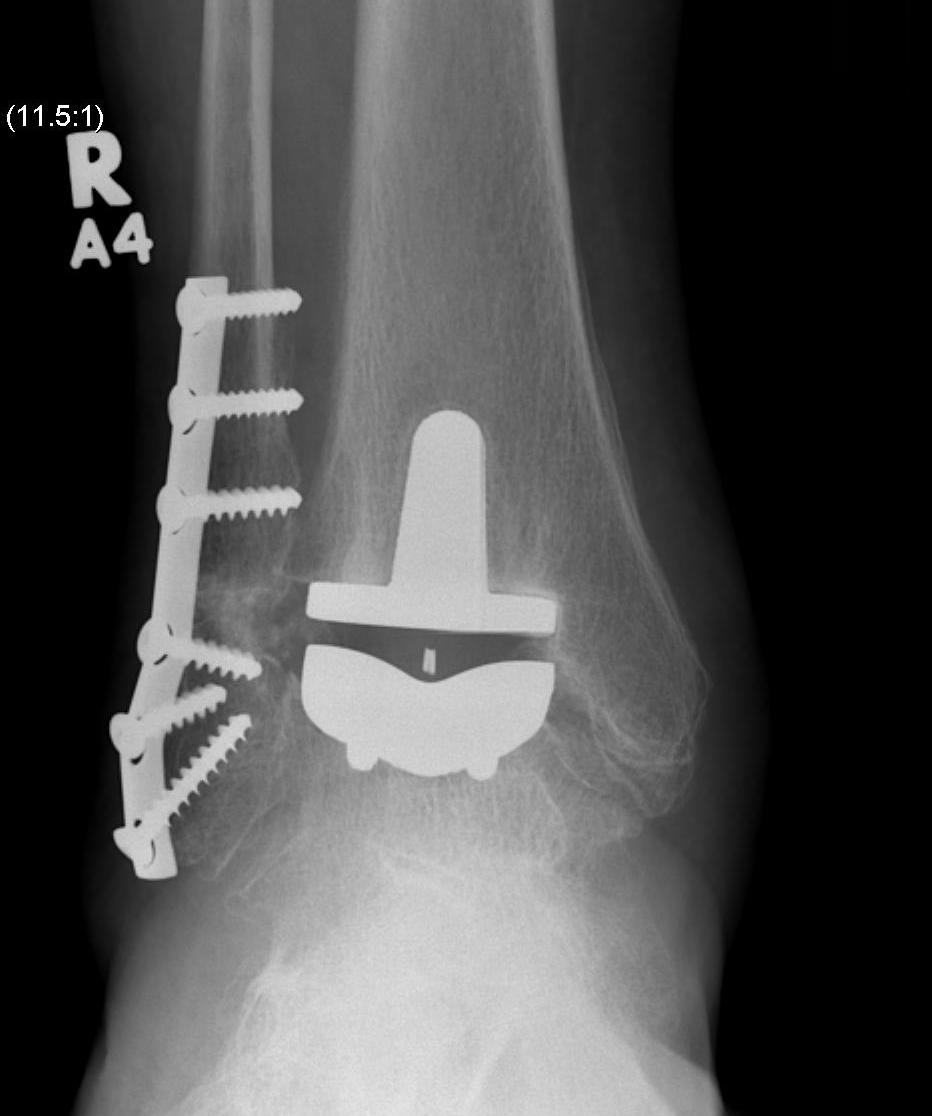

History
First generation (late 70s early 80s)
Results
Management
Observation
Curves < 20o observation only at 3-6 month intervals depending on growth rate
Non Operative Management / Bracing
Never brace curves if patient Risser 4 or 5
Indications
1. Risser 0-2 (growth potential)
2. Curve >30o adolescent
3. Curve >25o with progression (5o in six months)
Describing Bone Tumour X-rays
1. Pattern of bone destruction
Geographic
Least aggressive
- usually indicative of slow growing lesion
- usually seen in benign tumours
- may be myeloma / mets / OM
Narrow transition from normal to abnormal bone
- Margin of the lesion is well defined
- margin is easily separated from surrounding bone
- margin may be smooth / irregular, sclerotic / non sclerotic
Distal femur fractures
Problem
1. Undulating growth plate / higher rate of growth plate injury
- growth arrest / LLD
- angular deformity
- need to be warned
- require close and careful follow up especially in first 2 years
2. Can be unstable / malunion and shortening very problematic in this area
Xray
Salter Harris I
Radial neck fracture
Mechanism
FOOSH
- valgus injury
- don't get radial head fracture as is mostly cartilaginous
Types
SH 1 or 2
Associated Injuries
MCL injury
Olecranon / Medial epicondyle fracture