
Definition
Fracture through distal humeral physis in young children
Entire distal humerus physis is displaced
Epidemiology
Rare
Children < 3 with trauma
Non accidental injury / NAI
Neonates / birth trauma - difficult delivery / instrumented delivery / breech presentation
Clinical
Can be delayed presentation
- swelling / deformity
- pseudoparalysis
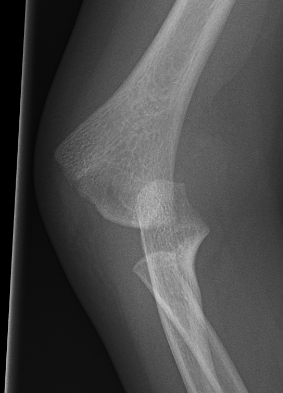
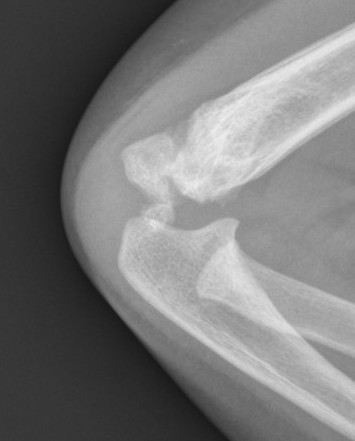
Xray
Distal physis not ossified < 1 year
- radius and ulna lose normal association with distal humerus
- posteromedial displacement of the ulnohumeral joint
- appears like an elbow dislocation
- disruption of radio-capitellar line




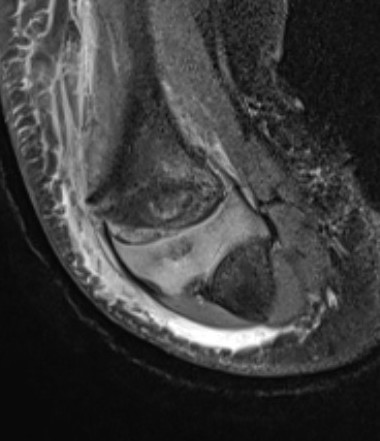
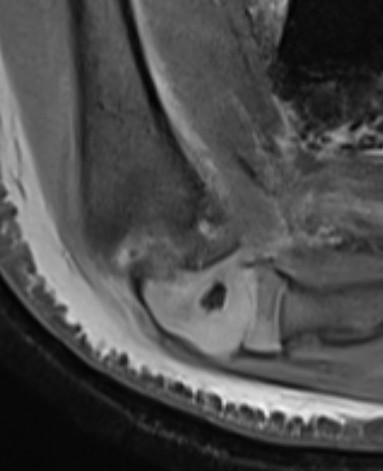
Diagnosis
Ultrasound
MRI
Arthrogram

Management
Options
Nonoperative care
Closed reduction - ? risk of AVN with late presentation
Closed reduction + percutaneous K wires
Results
Nonoperative
Brichni et al Orthop Traumatol Surg Res 2026
- 12 cases of distal humeral separation with 8 year follow up
- treated nonoperatively with cast
- complete and symmetrical ROM
- one resolving cubitus varus
Operative v nonoperative
Chalidis et al J Clin Med 2025
- systematic review of distal humerus physeal separation
- 12 studies and 260 patients
- NAI 17%
- 85% good or excellent results
- best results with K wiring / worst with closed reduction and cast
- cubitus varus 19%
- AVN 4%
Closed reduction +/- percutaneous K wires
- 10 cases of transphyseal humeral separation in neonates
- birth trauma
- 4 closed reduction, 6 percutaneous K wire
- all healed, no deformity or functional loss
Cha et al Injury 2020
- 12 patients treated with arthrogram + K wire fixation
- normal outcomes, no AVN
Closed reduction


Closed reduction + percutaneous K wires
May need arthrogram to visualize distal humerus epiphysis


Complications


AVN post reduction and K wire in a 2 year old