
Definition
Walking age child with unilateral / bilateral hip subluxation or dislocation
Hip has been out for some time and child has acetabular dysplasia
- need open reduction + osteotomies
Clinical signs
| Unilateral hip dislocation / subluxation | Bilateral hip dislocation / subluxation |
|---|---|
|
Limp / abductor lurch / Trendelenberg gait
Leg length discrepancy
Decreased abduction |
Waddling gait / bilateral Trendelenberg gait
Increased lumbar lordosis
Bilateral decreased abduction
|
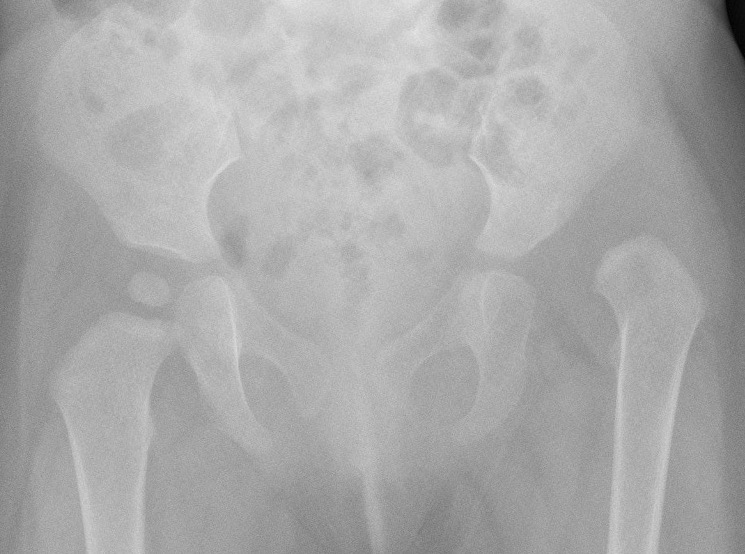
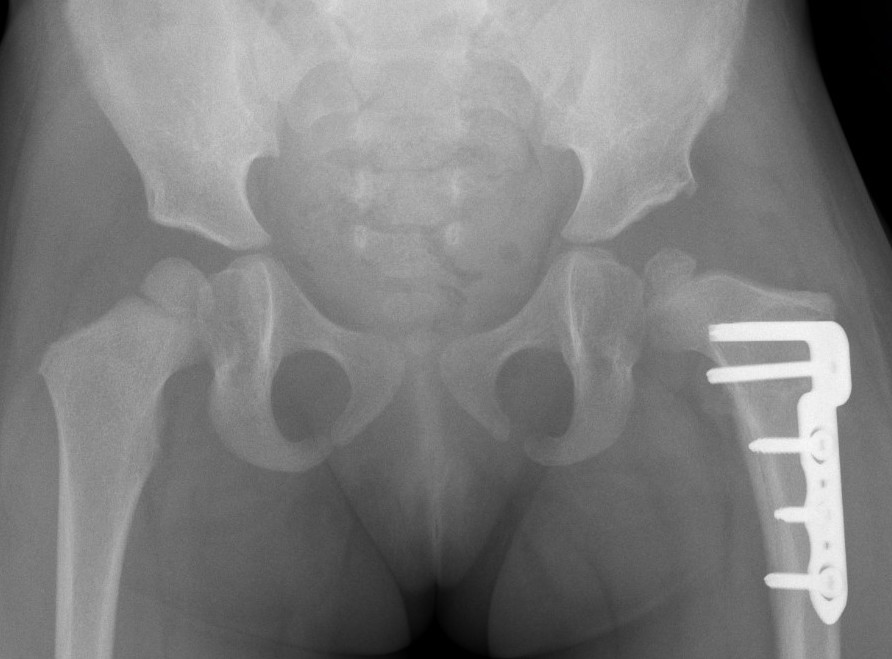
Xray


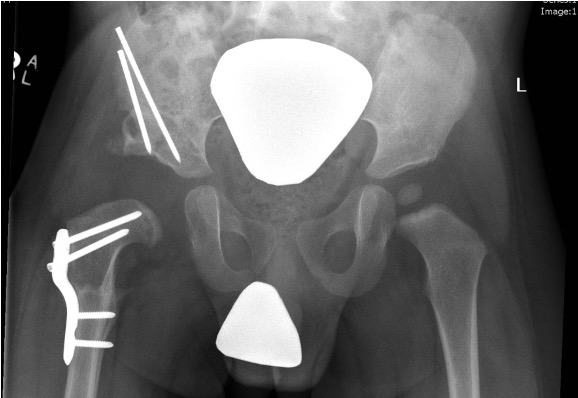
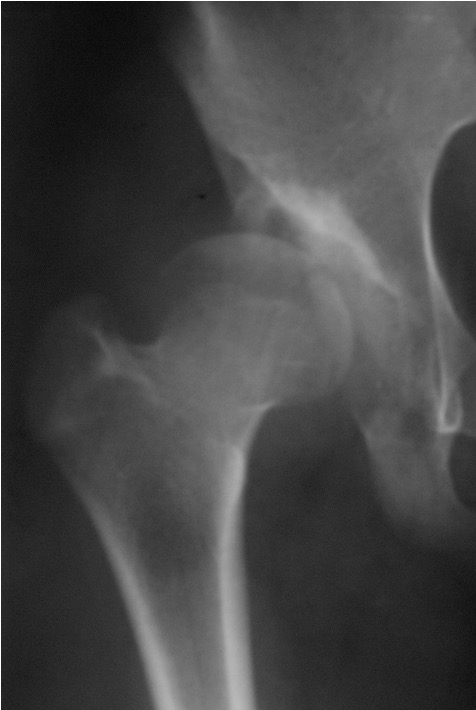
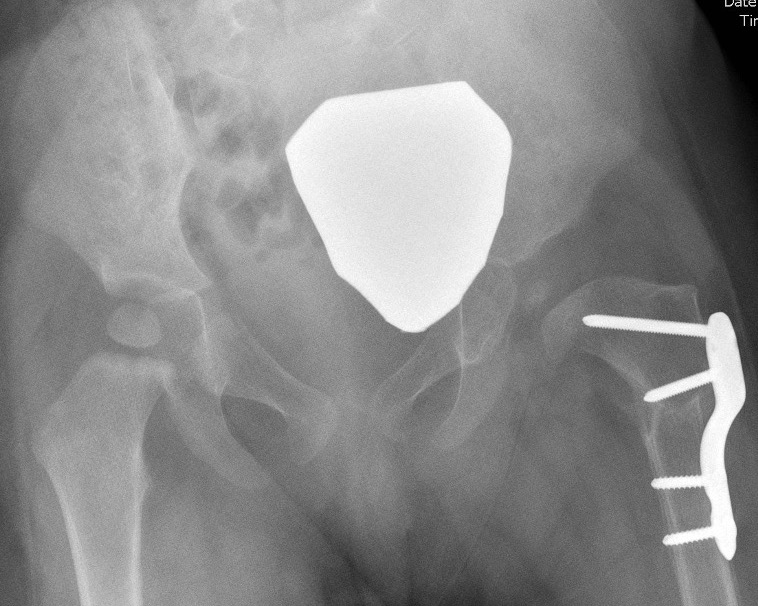
Dislocated hips in the setting of DDH with ncreased acetabular index
Management
Open reduction +
1. Pelvic osteotomy
- acetabular dsyplasia
- usually indicated in child of walking age
2. Femoral Varising Derotation Osteotomy (VDRO)
- shortening indicated if difficulty reducing the hip
- derotation if femoral anteversion > 50 degrees
Results
Outcome
Ning et al BMC Musculoskeletal Disorder 2014
- 864 hips treated with open reduction / pelvic osteotomy / femoral osteotomy
- 80% good or excellent results
- 27% AVN
- poorest outcomes age > 8
AVN
- 278 hips with Tonnis Grade IV DDH
- mean age 3
- treated with open reduction / pelvic osteotomy / femoral osteotomy
- 32% AVN
Bilateral
- 56 walking age bilateral DDH versus 156 bilateral DDH
- mean age 2 - 3 years
- worse outcomes and higher AVN with bilateral
Open reduction
Technique
Vumedi open reduction DDH Smith Peterson video
Medial approach
- release adductor tendon +/- psoas tendon
Smith Peterson approach
- split iliac apophysis
- identify and protect lateral femoral cutaneous nerve
- interval between sartorius and TFL
- interval between rectus femoris and gluteus medius
- retract sartorius and direct rectus medially or tag and release
- T shaped capsulotomy
Release
- release psoas tendon medially
- sublux femoral head from acetabulum
- ligamentum teres from femoral head and completely excise it
- resect pulvinar / medial fatty tissue
- divide transverse ligament
- identify and protect labrum
Trial reduction of femoral head
- if excessive tension / perform femoral shortening varus osteotomy
- capsulorraphy
Add pelvic osteotomy
Repair split in iliac apophysis
Hip spica for 6 weeks
Pelvic osteotomy
Indications
Acetabular dysplasia
Nearly always performed in hip reduction in walking age children

Options
Redirectional - Salter
Reshaping - Dega / Pemberton
Salvage / Augmentation - Chiari / Shelf
| Redirectional osteotomy | Reshaping osteotomy | Salvage / Augmentation osteotomy | |
|---|---|---|---|
| Mechanism |
Shift position of acetabulum No change to shape or volume |
Change slope, shape of acetabulum Reduce volume of acetabulum |
Increase femoral head coverage |
| Indication |
Normal acetabular shape Anterolateral deficiency |
Abnormal acetabular shape |
Concentric reduction not possible
|
| Types |
Salter: <8 years with flexible pubic symphysis
Tonnis triple osteotomy |
Dega
Pemberton |
Chiari
Shelf |
| Technique | Complete osteotomy |
Incomplete osteotomies Bend through triradiate cartilage |
Medial displacement osteotomy |
|
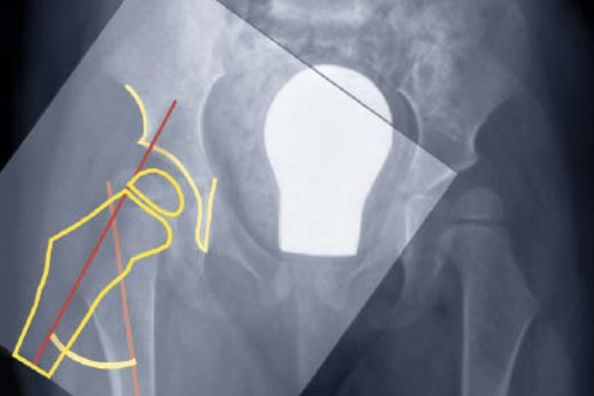
Salter osteotomy |
Dega osteotomy |
Chiari osteotomy |
Results
- systematic review of Salter's v Pemberton v Dega in 2000 cases
- better Severin outcome score with Pemberton / Dega v Salter
- best outcomes for Pemberton
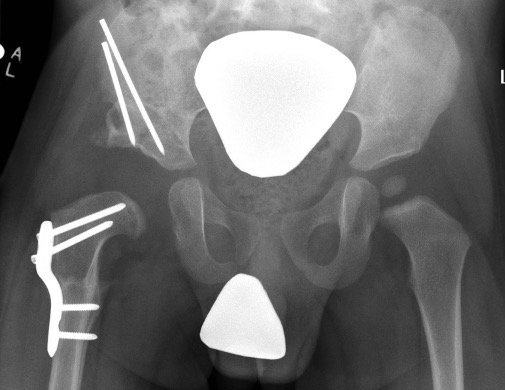
Salter Redirectional Osteotomy
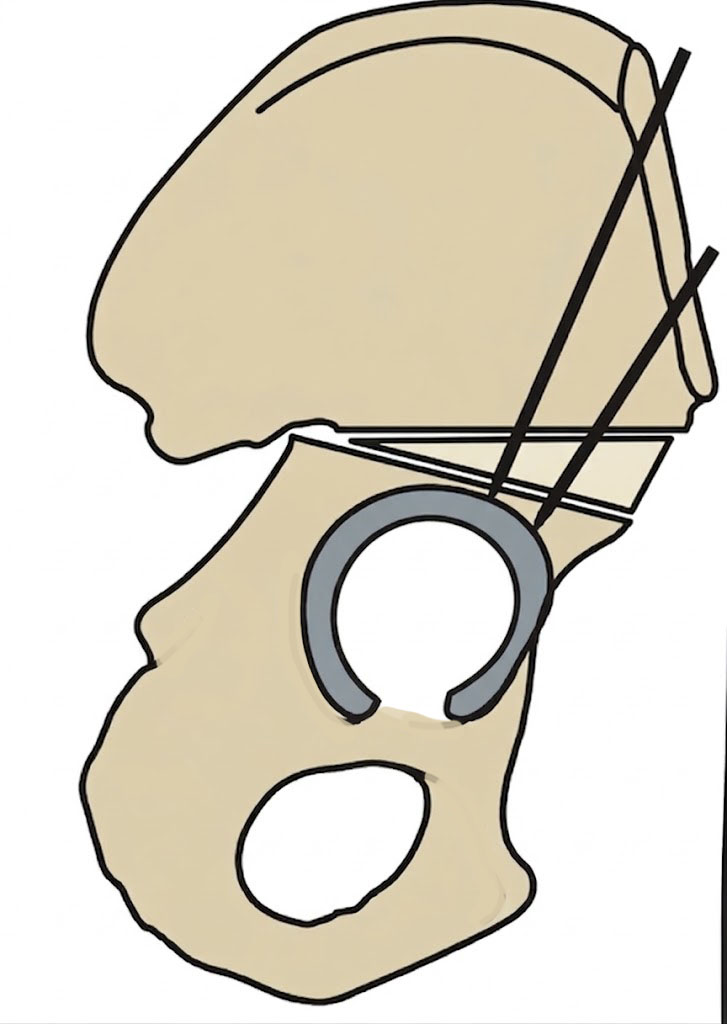
Indication
Anterolateral acetabular deficiency with concentric acetabular shape
Younger patient < 8 years - osteotomy rotates through flexible pubic symphysis
Technique
Vumedi open reduction and Salter osteotomy video
Vumedi open reduction and Salter osteotomy video 2
Smith Peterson approach
- iliac apophysis split
- release direct head of rectus and psoas tendon
- subperiosteal dissection to sciatic notch reflecting gluteals
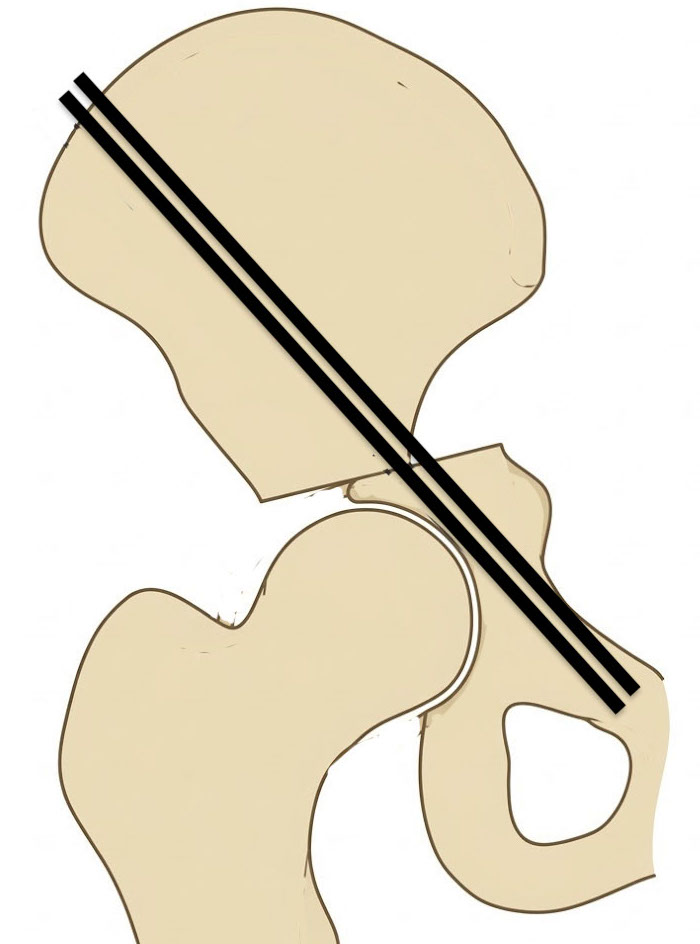
Osteotomy
- through greater sciatic notch to between ASIS and AIIS
- Gigli saw passed around greater sciatic notch
- osteotomy posterior to anterior
- acetabulum rotated anteriorly and laterally
- 15 mm triangular graft from iliac crest apophysis
- secure with K wire fixation
Repair split in iliac apophysis

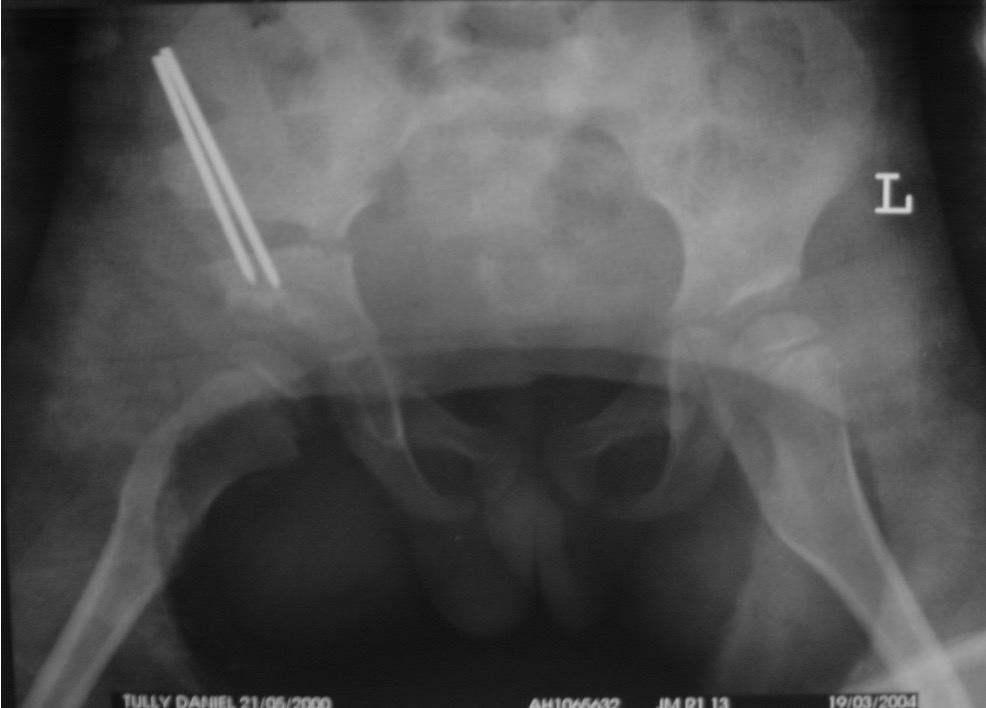
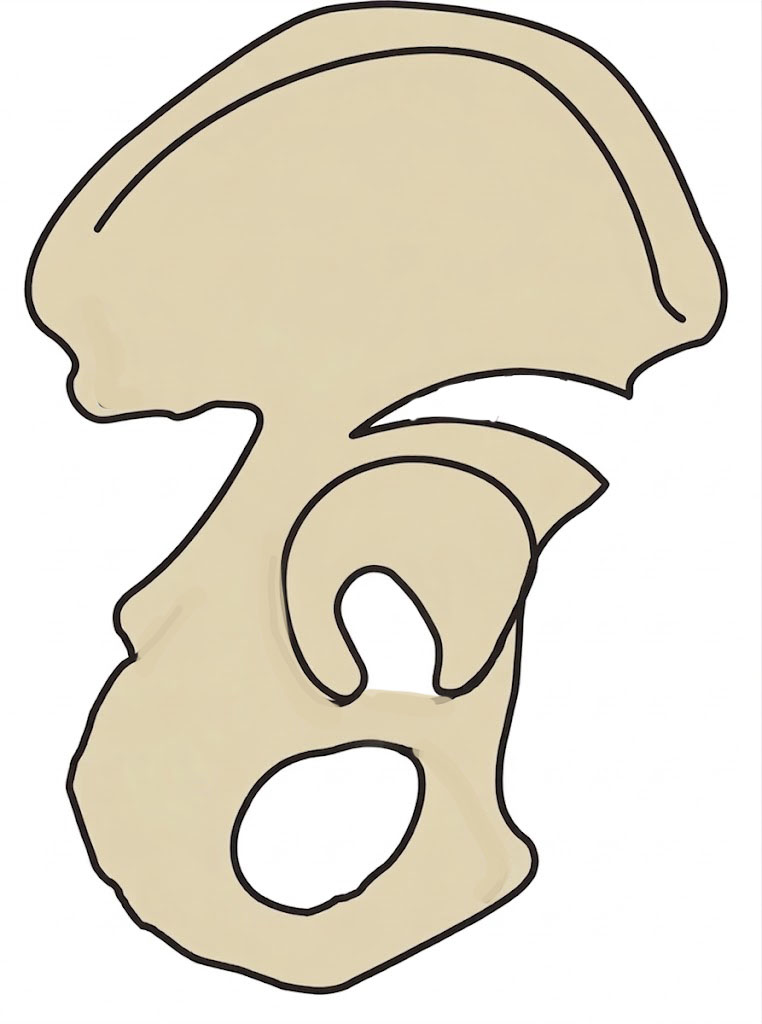
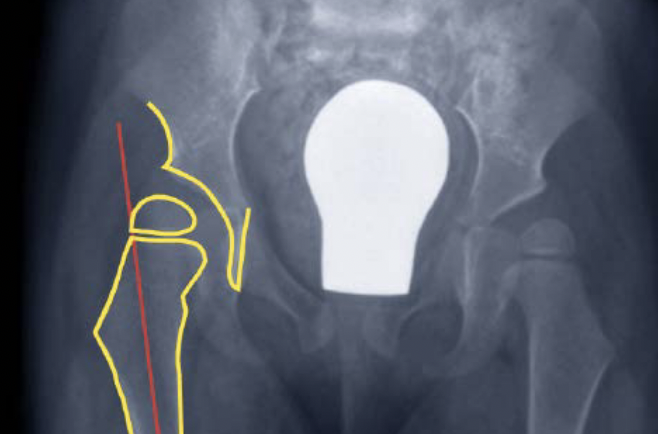
Salter complete osteotomy


Salter complete osteotomy
Reshaping osteotomy
Indication
Lateral deficiency
Abnormal acetabular shape
Concept
Dega / Pemberton
- incomplete iliac supra-acetabular osteotomies
- anterior and middle thirds of ilium, stop short of sciatic notch
- bend through tri-radiate cartilage
Technique

JBJS Essential techniques Pemberton Osteotomy PDF
AAOS Pemberton Osteotomy technique video
Smith - Petersen approach
- split apophysis
- release direct head of rectus and psoas tendon
- curved osteotomes
- 15 mm above and parallel to superior dome of acetabulum
- leave posterior column intact
- bone graft +/- K wires
Results
Wozniak et al J Pediatr Orthop B 2023
- systematic review of 636 hips treated with trans-iliac Dega pelvic osteotomy
- mean correction acetabular index 23 degrees
- 82% Severin Class I/II
- 85% clinical outcome good or very good
- 19% AVN
- reoperation 6%
Chiari / Salvage Osteotomy

Concept
Medial displacement osteotomy
Creates a shelf or bony roof above the femoral head
Indication
Painful unstable DDH
Incongruent hip joint / early OA

Chiari osteotomy
Femoral Varus Derotation Osteotomy (VDRO)

Indication
Tight reduction risking AVN
Unstable reduction with increased femoral anteversion
Increased femoral neck angle
Technique


Synthes Pediatric Proximal Femur Offset Plate Technique PDF
Youtube open reduction and VDRO video
Measure planned correction
- preoperative: 150 degrees
- postoperative: 120 degrees
Separate lateral approach
- elevate vas lateralis +/- release proximally with L shaped release
- open and protect periosteum with Homan retractors
- mark distal and proximal femur with drill holes to check rotation
- place wires up femoral neck short of physis
- use plate to mark osteotomy site
Osteotomy with microsagittal saw 1 cm below lesser tuberosity
- may need to shorten
- +/- adjust version
- apply plate and fix with screws
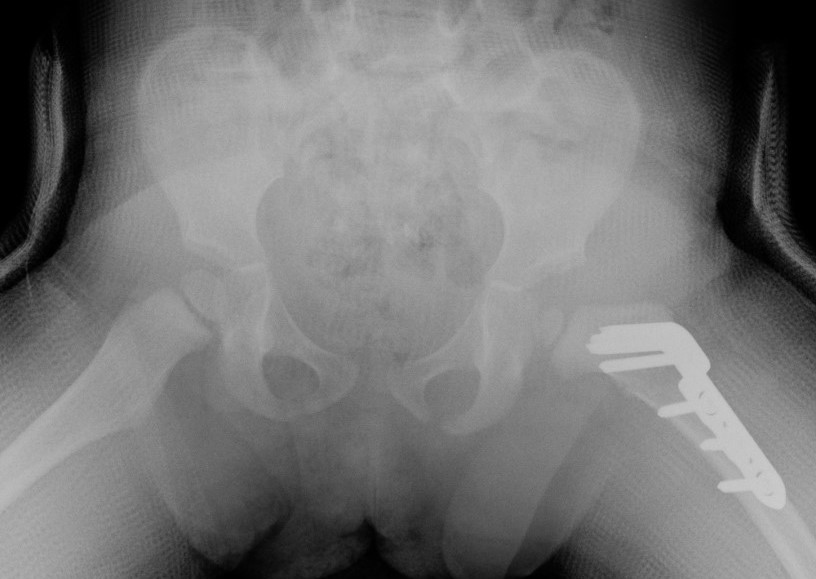
Results
Shi et al J Orthop Surg Res 2020
- 29 corrective femoral osteotomy for DDH
- half conventional technique, half computer navigation
- computer navigation increased accuracy, and reduced radiation exposure and surgical time