Complications
Complications
Types
Chondrolysis
AVN


Chondrolysis
AVN


Spontaneous osteonecrosis of the navicular
Osteoarthritis
- abnormal morphology
- loss of head neck offset
- bony impingement on acetabulum
AVN

Osteonecrosis of the navicular
Present at age 4-6 years
- same as Perthes disease
M:F 5:1
Bilateral in 20%
Repetitive trauma to maturing ossific nucleus
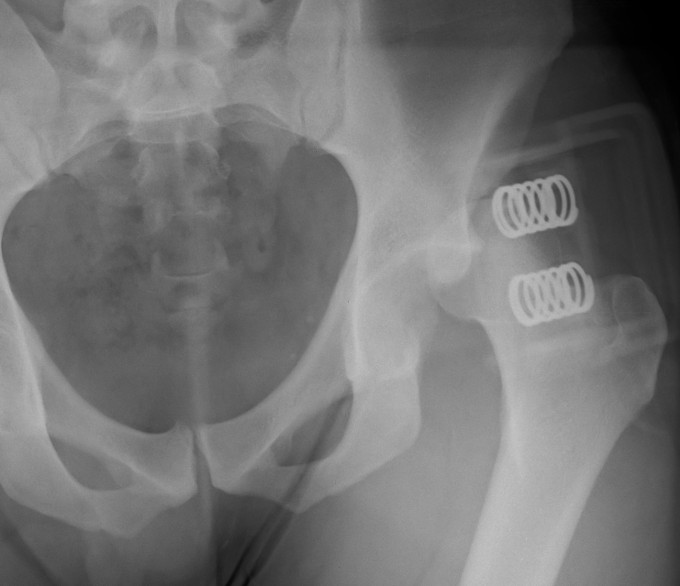
< 60 with good bone stock and preserved joint space
Union rates increased with anatomical reduction
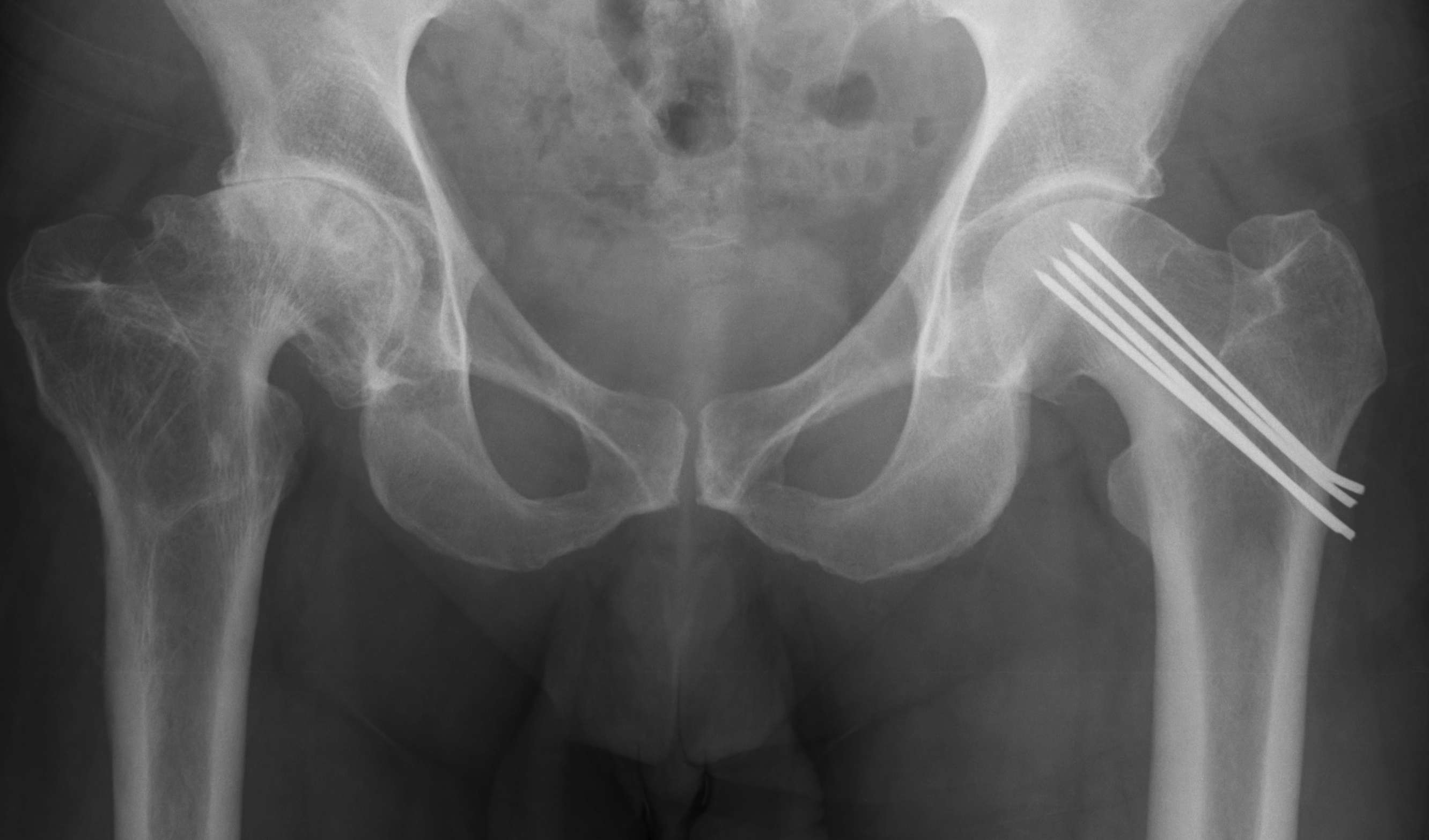
Options
- closed reduction
- open reduction / if closed reduction fails
Accept
- no varus
- < 15o valgus
- < 10o AP plane
Education regarding shoe wear
- extra wide / large toe box
Insoles
- longitudinal arch support
- pre MT dome for metatarsalgia
- podiatry to attend to callosities
Toe spacers
Analgesia
1. Continued pain and discomfort
2. Difficulties with shoe wear
Young men
Posterior / Anterior 9:1
High velocity injury
- head direction at impact decides direction of dislocation
Anterior Dislocation
Externally rotated & abducted leg
- flexion = inferior dislocation
1. Late presenters
2. Failures of splint in those < age 6/12
1. Adductor tenotomy + closed reduction
- most surgeons will attempt this initially
- risk of AVN wilth forceful reduction / excessive abduction
2. Open Reduction
- for failure of closed reduction
To obtain and maintain a concentric reduction without complication
0 - 6 /12
- best time for treatment
- maintain reduction of head & allow normal acetabular development
Obtain ultrasound
Graaf 2A and 2B
- Alpha angle 50 - 59o range
- many will resolve without treatment
Stage 0
Natural history mixed
- depends on size of lesion and diagnosis
- treat if becomes asymptomatic
- may benefit from bisphosphonates
Stage 1 / Normal X-ray, abnormal MRI
Forage: 80% G/E
Bisphosphonates
Stage 2 / Abnormal X-ray with cysts and sclerosis
A: As for Stage I