Aim
Prevent head deformity by containing femoral head within acetabulum
- if the femoral head remains in the acetabulum it usually remains spherical
- lateral extrusion results in deformity which results in osteoarthritis
| Age at onset | Hip | Management |
|---|---|---|
|
< 8
|
Contained hip | Non operative management |
|
< 8 |
Uncontained hip Hinge abduction
|
Femoral varus osteotomy +/- pelvic osteotomy |
|
> 8 |
Uncontained hip Hinge abduction
|
Femoral varus osteotomy +/- pelvic osteotomy |
Operative versus nonoperative managment
Outcomes
- systematic review of operative versus non operative management
- improved head sphericity in patients > 6 treated with surgery
- no effect < 6 years
- 345 Perthes hips
- no effect of treatment in children < 8 at age of onset
- Herring B and B/C: better outcomes with operative versus nonoperative treatment
- Herring group C: no difference operative versus nonoperative treatment
- systematic review of 650 surgically treated hips
- Herring type B hips: 70% good outcome
- Herring type B/C hips: 57% good outcome
- Herring type C: 38% good outcome
- 358 patients with 5 year follow up
- no effect surgery age onset < 6
- > 6 and > 50% head involvement - improved outcomes with femoral osteotomy
Nonoperative management
Indication
Age < 8 at onset
Herring A / Lateral pillar maintained
Good abduction
Options
Brace
Physio
Results
- 345 Perthe's hips
- no difference between no treatment / brace / physiotherapy
- 167 Perthes hips followed for 47 years
- non operative treatment
- 13% THA
Operative management
Goal
Containment of femoral head within acetabulum
Allows physiological remodelling of the epiphysis
Indications
> 8 at onset
Herring B or B/C
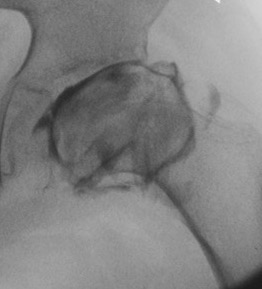
Uncontained hip / lateral extrusion
Hinge abduction
Reduced ROM
Herring B / BC



Uncontained hip / lateral extrusion


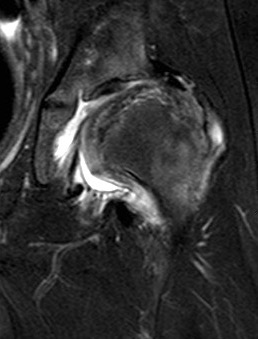
Hinge abduction

Containment Options
Femoral varus osteotomy
Pelvic osteotomy
- Salter osteotomy - < 8 when pubic symphysis elastic
- Triple pelvic osteotomy (Bernese / Tonnis) - older child
Combined femoral and pelvic osteotomy
Salvage Options

Valgus femoral osteotomy
Femoral head reduction osteotomy
Shelf osteotomy
| Femoral osteotomy | Pelvic osteotomy | |
|---|---|---|
| Advantage |
Treatment on affected side No increase intra-articular pressure Varus tends to restore over time
|
No trendelenberg gait |
| Disadvantage |
Shortens limb Greater trochanter more proximal Possible trendelenberg gait
|
Treatment on non affected side Increases intra-articular pressure May cause retroversion / FAI |
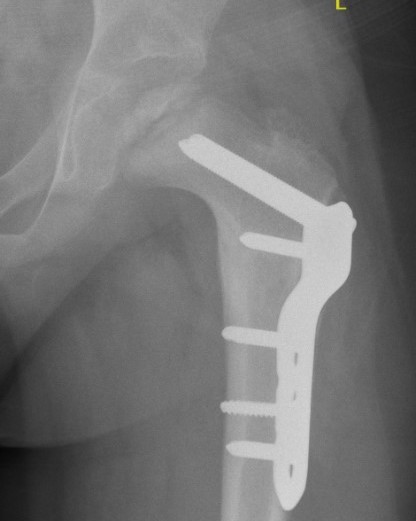
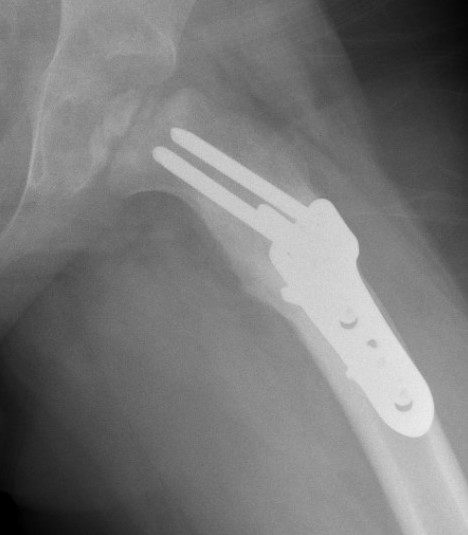
Femoral Varus Osteotomy (FVO)
Indications
Herring grade B or B/C
> 8 years at age on onset
Full containment of cartilaginous head
No hinge abduction
Issues
Persisting cova vara
Leg length discrepancy
Over-riding greater trochanter
Outcomes
- 52 Perthes patients treated with FVO
- optimal correction 15 degrees
- 30% had over riding greater trochanter
- 37% no correction of varus over time
Beer et al J Pediatr Orthop 2008
- 43 hips treated with FVO with 33 year follow up
- 55% Stuhlberg I / II
- 42% Stuhlberg III / IV
- 2% Stuhlberg V
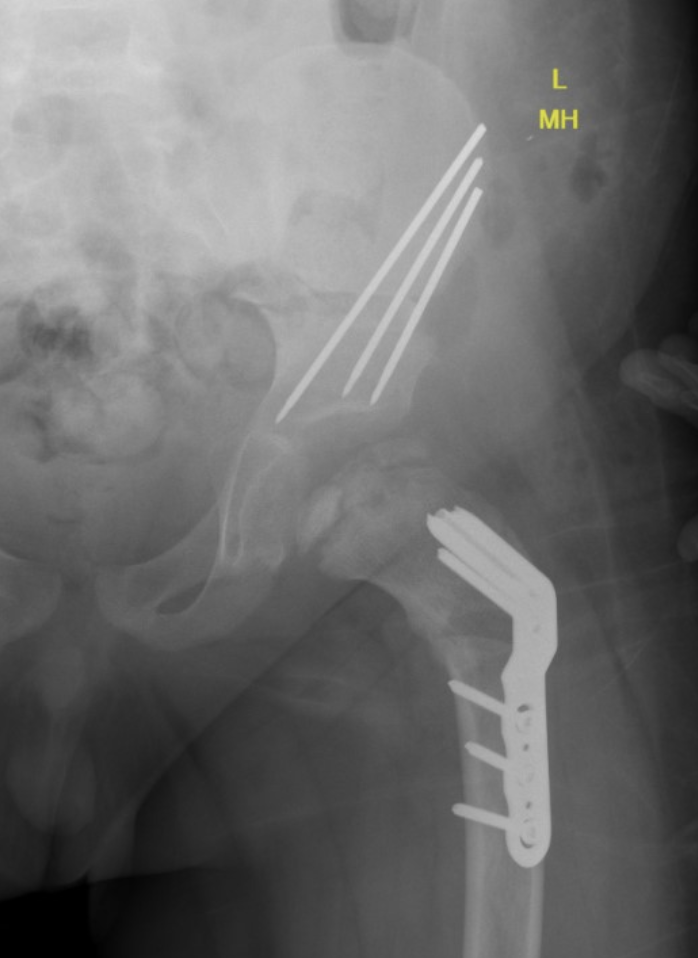
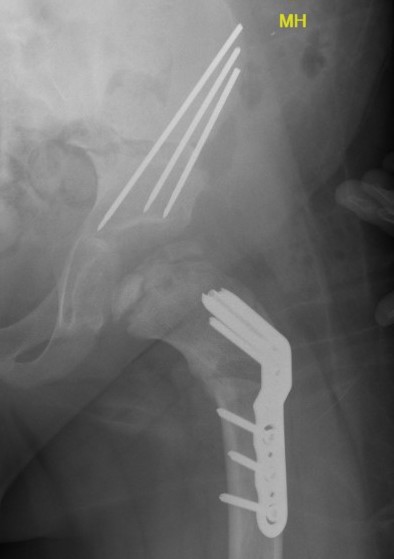
Technique

Synthes Pediatric Proximal Femur Offset Plate Technique PDF
Youtube femoral varus osteotomy for Perthes video
Patient supine on radiolucent table
- preop antibiotics
- frog leg laterals when needed
Lateral approach
- elevate vas lateralis +/- release proximally with L shaped release
- mark distal and proximal femur with drill holes to check rotation
- place wires up femoral neck short of physis
- use plate to mark osteotomy site
Osteotomy with microsagittal saw 1 cm below lesser tuberosity
- aim for 115o of varus
- avoid excessive varus < 100o to keep greater trochanter distal to femoral neck
- +/- adjust version
- apply plate and fix with screws
Salter pelvis osteotomy
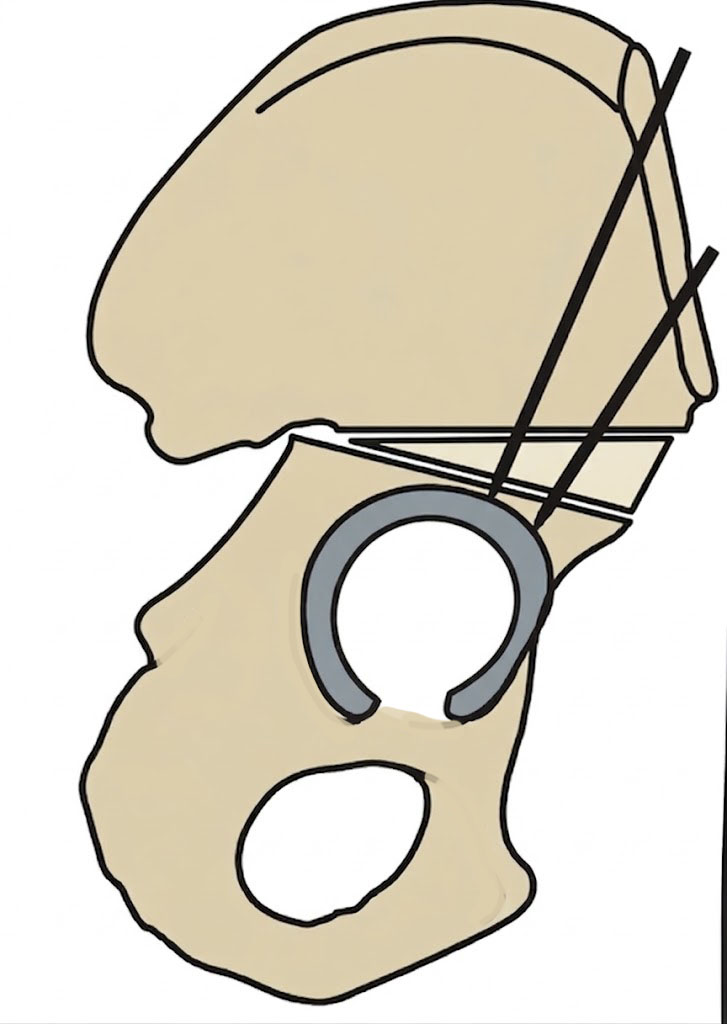
Concept
Redirects acetabulum to provide coverage for anterolateral head
Smith Peterson approach
- iliac apophysis split
- release direct head of rectus and psoas tendon
- subperiosteal dissection to sciatic notch reflecting gluteals
Osteotomy
- through greater sciatic notch to between ASIS and AIIS
- Gigli saw passed around greater sciatic notch
- osteotomy posterior to anterior
- acetabulum rotated anteriorly and laterally
- 15 mm triangular graft from iliac crest apophysis
- secure with K wire fixation
Repair split in iliac apophysis
Combined Femoral and Pelvic Osteotomy



Salvage
Indications
Failure of containment techniques / hinge abduction
Significant femoral head deformity
Options
Valgus femoral osteotomy
Femoral head reduction osteotomy
Shelf Arthroplasty
Valgus femoral osteotomy
Concept
Hinge abduction
- move medial, better-preserved part of the femoral head into the loading zone
- reduce adduction contracture and distalize the greater trochanter
Femoral head reduction osteotomy (FHRO)
Concept
Misshapen femoral head
Open surgical dislocation
- remove central necrotic area femoral head
- rreposition lateral femoral head to medial femoral head
Results
Eltayeby et al J Pediatr Orthop B 2024
- 22 severe Perthes treated with FHRO
- 23% poor outcomes
Shelf Arthroplasty

