

Ponseti casting
Three phases
1. Serial manipulation and casting
2. Percutaneous tenotomy
3. Bracing
Serial manipulation and casting
Begins first week
Options
- Conventional Ponseti technique: 5 - 8 above knee casts applied changed weekly for 6 weeks
- Accelerated Ponseti technique: casts changed every few days for 3 weeks
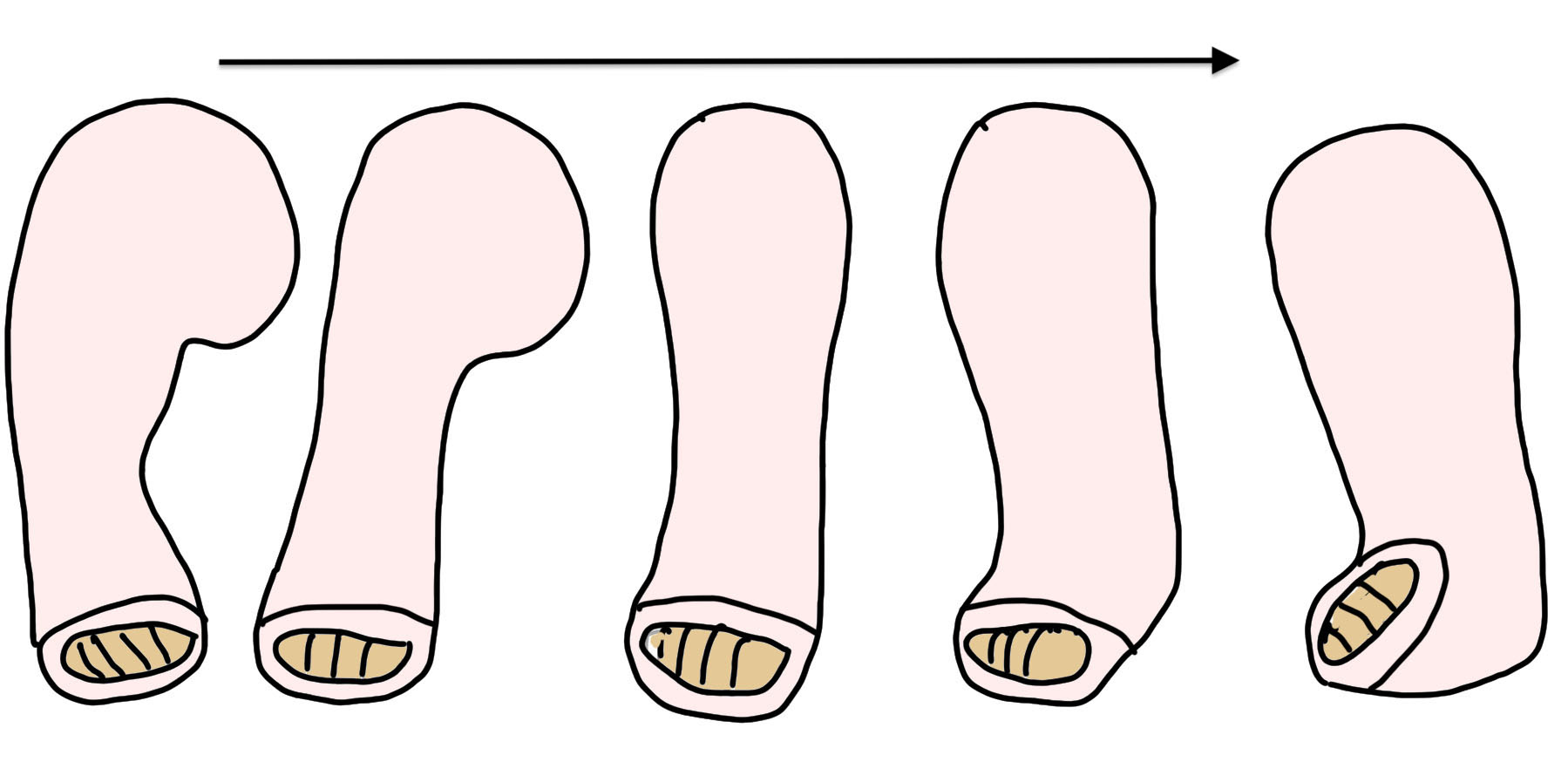
Sequence of correction
Youtube JBJS video Ponseti casting video
Physiopedia Ponseti casting PDF
Begin with short leg cast then convert to long leg cast
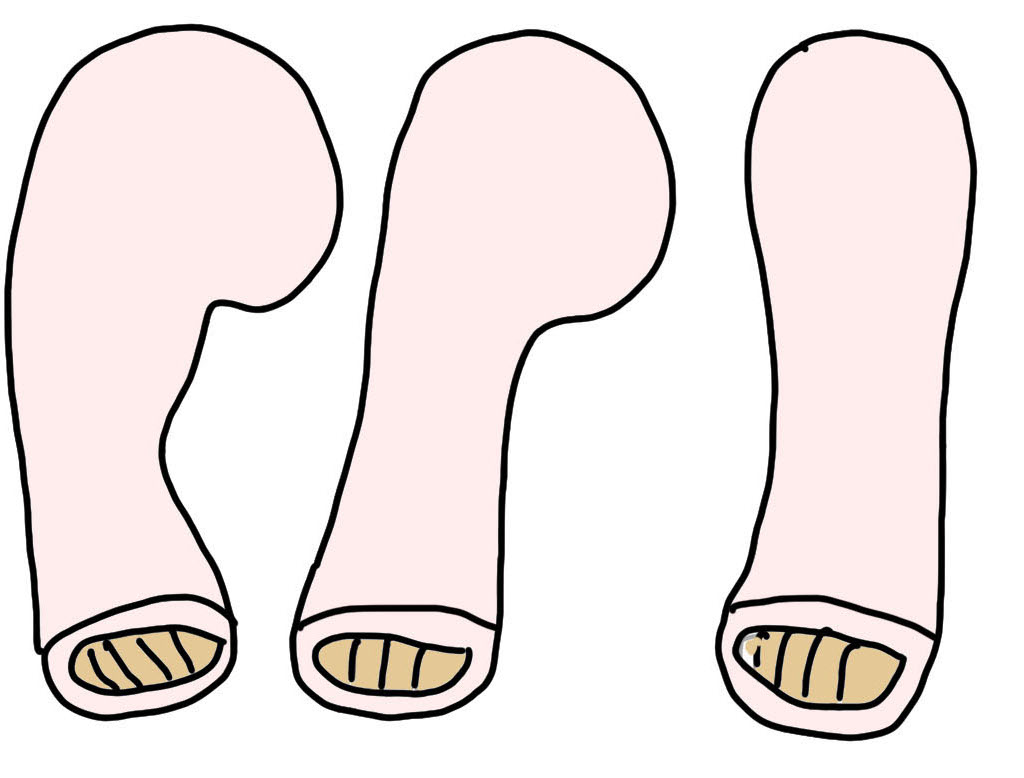
1. Correct cavus
- increase supination / elevate first ray
- matching forefoot to midfoot / hindfoot
- pronating foot worsens cavus
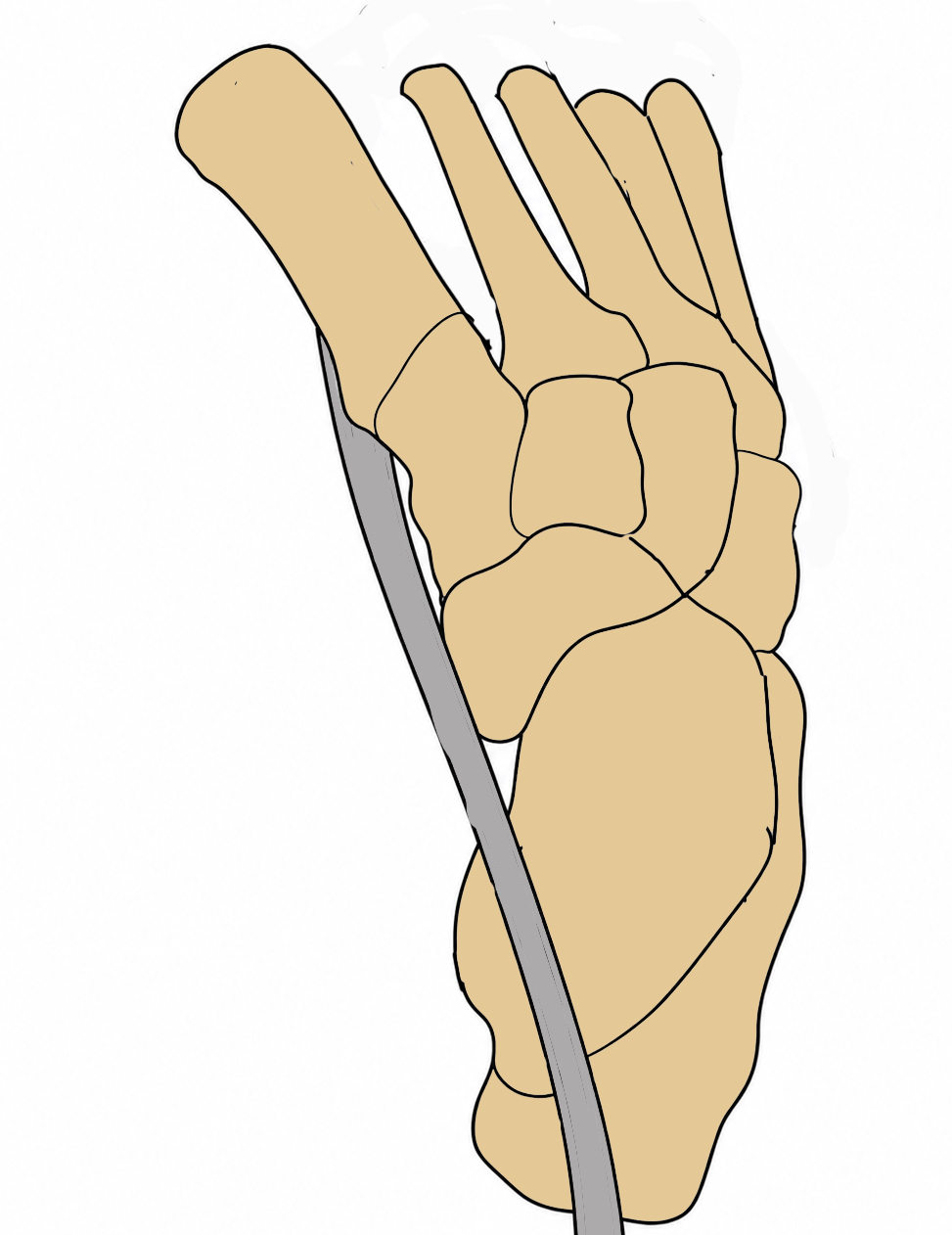
2. Correct varus / abduct the foot
- abduction and external rotation corrects varus
- rotates calcaneus under the talus / correct the subtalar joint
3. Correct equinus last
- once cavus and varus corrected
- forceful manipulation to correct equinus prior to correction of hindfoot varus
- will result in either a rockerbottom deformity or a flat top talus
Percutaneous tenotomy

Indication
- abduction / external 60o and but dorsiflexion < 10 - 20o
- required in 90% of children
Technique
- week 5 / 6
- performed in outpatient setting
- local anesthesia
- insert beaver blade medially
- continue Ponseti casting for 3 further weeks
Results
- systematic review of outpatient tenotomy v in operating room
- repeat tenotomy OPD: 3%
- repeat tenotomy OR: 1%
- complication rate 2% - bleeding most common
Long term splinting
Most important phase / required for 4 years
1. First 3 months
- AFO / Dennis Brown boots
- 23 hours a day for 3 months
2. 3 months to 4 years
- AFO / Dennis Brown boots worn at night
- shoulder width apart
- clubfoot external rotated 60 - 70o
- normal foot externally rotated 30 - 40o
Results
Ponseti technique
Zhao et al J Orthop Surg Res 2025
- systematic review of Ponseti technique
- idiopathic: initial correction success 96 - 98%, relapse 20 - 30%
- syndromic / neurological: initial correction success 91%, relapse 32%
Conventional versus accelerated Ponseti technique
- systematic review of conventional versus accelerated Ponseti
- faster treatment with Ponseti
- no difference other outcome measures
- number of casts (5 vs. 5)
- rate of tenotomy (66% vs. 63%)
- relapse rate (10% vs. 9%)
- complication rate (14% vs. 13%)
Idiopathic CTEV versus Arthrogryposis
Church et al J Paediatr Orthop 2025
- 10 year outcome of Ponseti technique
- idiopathic CTEV: 33% required additional surgery
- Arthrogryposis: 44% required additional surgery
Complications
Casting complications

Flat top talus
Associated with increased length of Ponsetti casting / forced dorsiflexion
- varies in severity
- may reduce dorsiflexion range / affect gait
- 50 consecutive CTEV treated with Ponseti casting
- 26% developed flat top talus
- associated with casting > 3 months
Relapse / recurrence (one-third of patients)
Mild recurrence
- repeat Ponseti casting
- Tibialis anterior transfer
Severe recurrence
- posteromedial release
- external fixation
Operative Management
Indications
Dynamic supination - Tibialis anterior tendon transfer
Severe residual / recurrent deformity
- posteromedial release
- external fixation
- triple arthrodesis
Dynamic supination during swing phase of gait
Concept
Tibialis anterior is a deforming force / Transfer tibialis anterior to lateral foot
SPLATT
- split tibialis anterior tendon transfer (SPLATT)
- < 3 years old
- Pulvetaft through peroneus brevis
TATT
- full tibialis anterior tendon transfer (TATT)
- > 3 years old
- attach to ossified lateral cuneiform via drill hole and tie over button
Techique
Three incision - medial / lateral / proximal incision above extensor retinaculum
Two incision - medial / lateral incision only
JBJS Essential techniques TATT pdf
Results
Masrouha et al J Pediatr Orthop 2012
- 102 relapsed clubfeet treated with tibialis anterior transfer
- 15% recurrence
Posteromedial release
Issues
Indicated for severe / relapsing / neurological feet
Not great results at long term follow up



Incisions
| Cincinatti | Turco | Norris-Carroll |
|---|---|---|
|
Incomplete circumferential incision - perform prone - good exposure lateral |
Posteromedial incision - base of 1st MT to tendoachilles |
Two incisions - medial from os calcis to TNJ - lateral halfway between tendoachilles and lateral malleolus |
| Can cause heel pad necrosis | May need separate lateral incision |
Medial releases
POSN Academy posteromedial release video
Posteromedial approach
- identify and protect NV bundle
- identify Knot of Henry above Abductor Hallucis
- reflect Abductor Hallucis downwards to identify FDL / FHL
- Z lengthen FDL / FHL
- Z lengthen tendoachilles and tibialis posterior
- capsulotomy posterior ankle joint and subtalar joint
- release plantar fascia
- open reduction and K wire talonavicular joint
- open reduction and K wire subtalar joint
Results


Gelder et al J Pediatr Orthop 2010
- 58 feet undergoing posteromedial release before age 2
- 16 year follow up
- 60% good / excellent results
- 40% fair / poor results
- majority loss dorsiflexion
- 9% required additional bony procedure for pain or overcorrection
External fixation
Results
Vaccalluzzo et al Arch Orthop Trauma Surg 2025
- systematic review of external fixation for recurrent CTEV
- overall success rate 81%
- complications common
- pin tract infection most common, toe contractures, digital ischemia.