


Epidemiology
Young men in 20's and 30's
High energy injuries - fall from heights / MVA
Commonly missed injury - up to 25%
Mayfield Classification
Stage I: Scapholunate ligament injury
Stage II: Capitolunate disruption
Stage III: Lunate-triquetral disruption
Stage IV: Dorsal radiocarpal ligament disruption
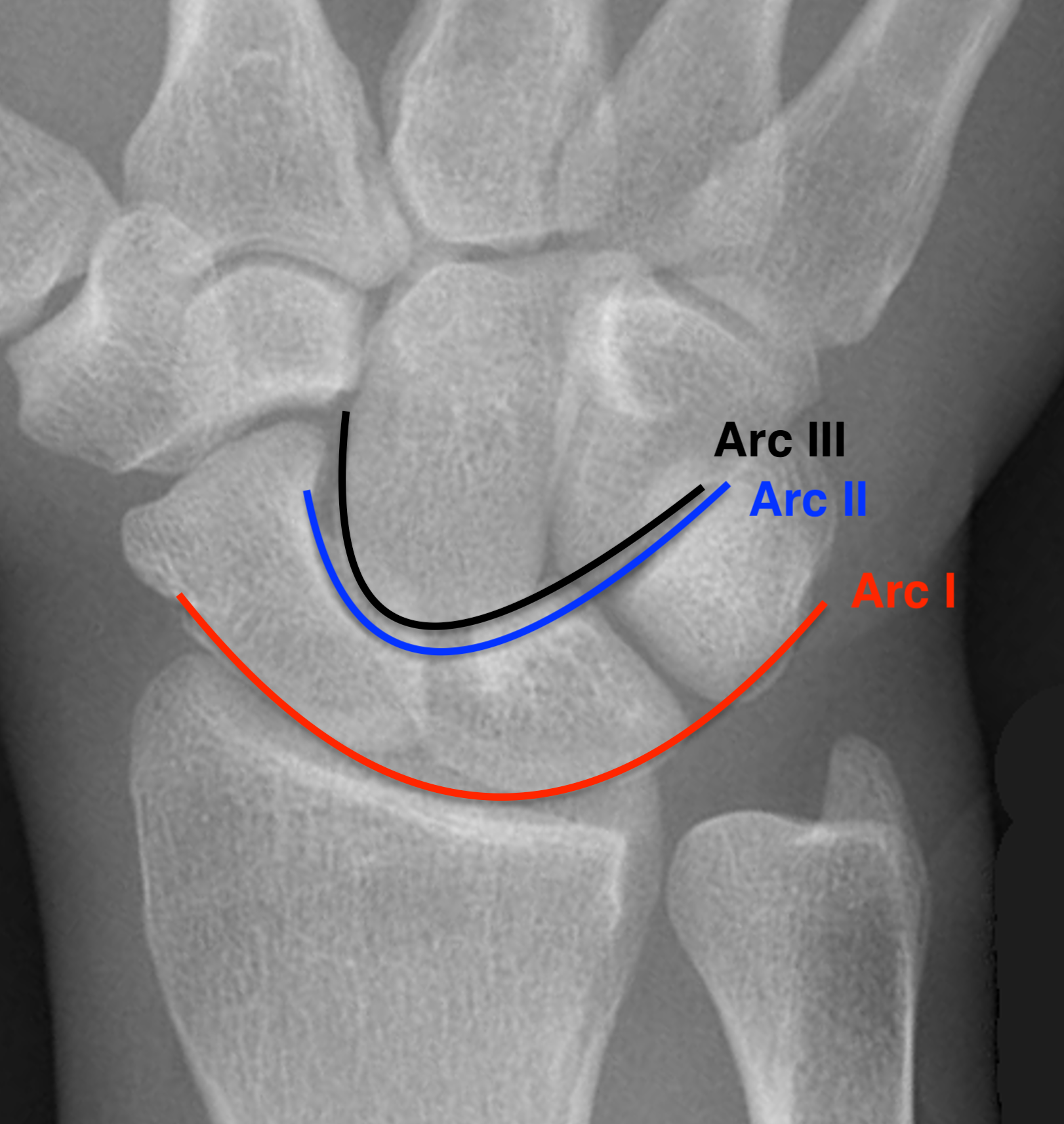
Gilula carpal arcs
| Giluala carpal arcs | Arc injuires |
|---|---|
|
Normally there are 3 smooth carpal arcs on PA xray
Arc I: Proximal cortical margins of proximal carpal row Arc II: Distal carpal margin of the proximal carpal row Arc III: Proximal cortices of the capitate and hamate |
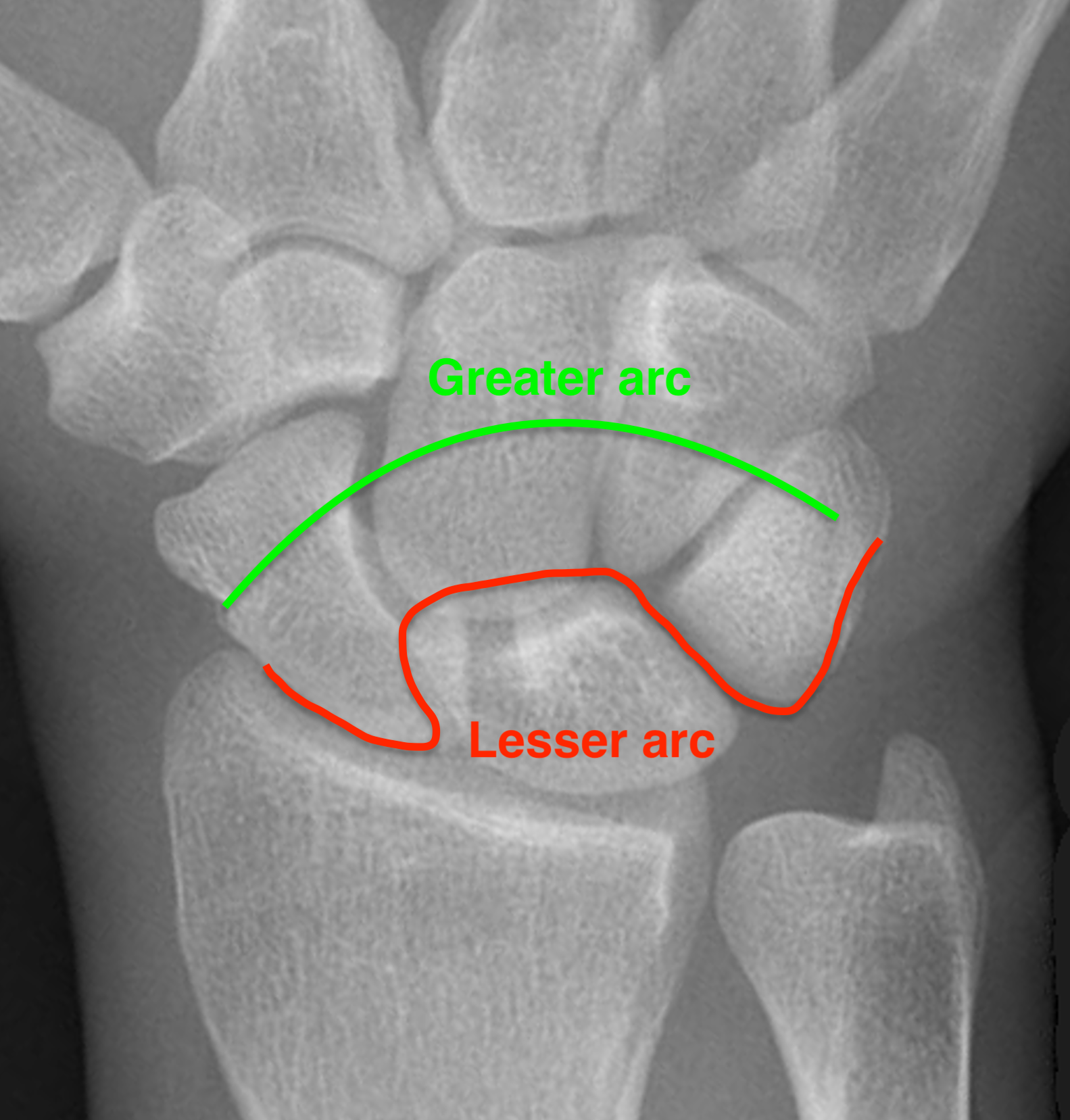
Greater arc injuries - ligamentous injury + fracture - fractures of scaphoid / capitate / radial styloid - scaphoid most common, radial styloid second)
Lesser arc injuries - Purely ligamentous injuries around the lunate
|
 |
 |
Presentation

Swollen and painful wrist
Median nerve symptoms
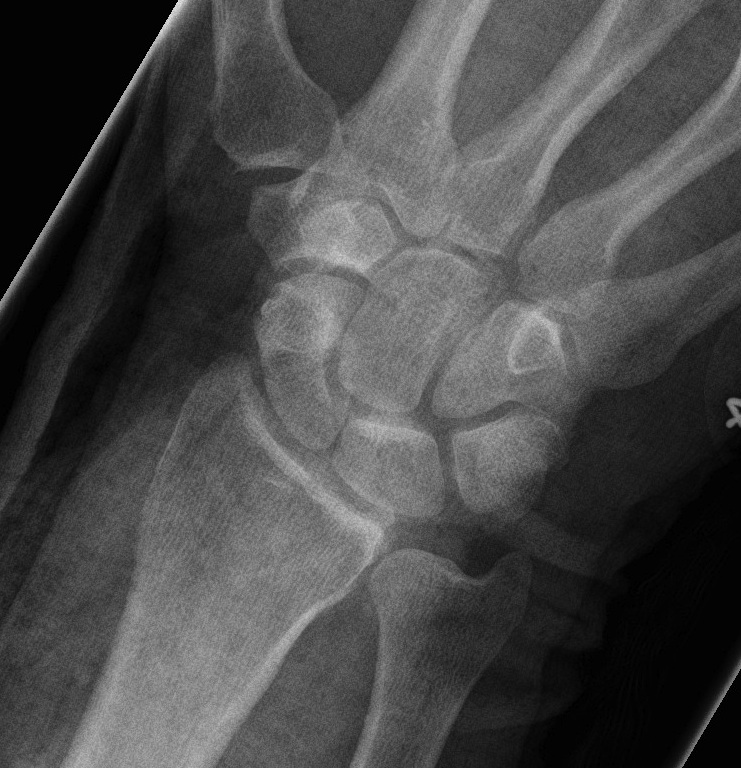
AP X-ray
Disruption of Gilula's 3 smooth carpal arcs / triangular lunate


Normal versus disruputed Gilula's carpal arcs

Normal versus disruputed Gilula's carpal arcs


Piece of pie / triangular appearance of lunate
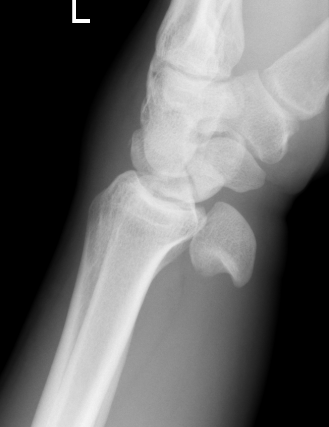
Lateral xray
Distal radius / lunate / capitate: not aligned, spilled teacup




Normal versus spilled tea cup appearance on lateral with spilled tea cup
Patterns of injury
1. Perilunate dislocation
Lunate remains aligned with distal radius
Capitate dislocates dorsally




2. Lunate dislocation
Lunate dislocates / usually volar
Carpus remain aligned with distal radius



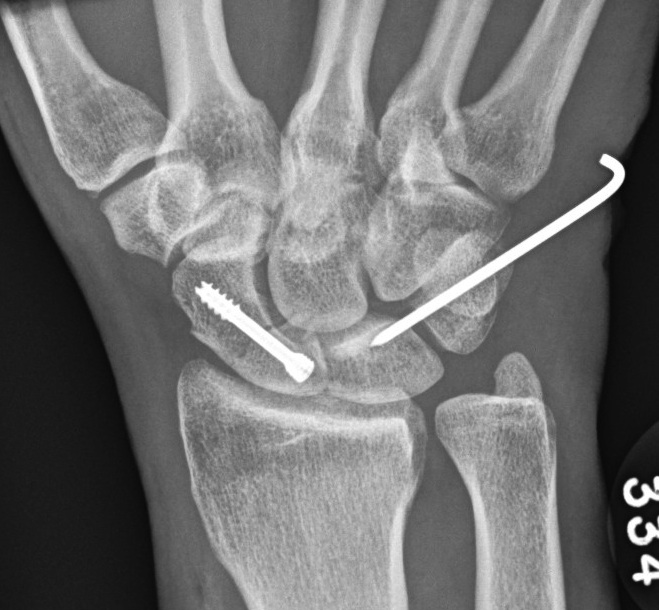
Perilunate fracture dislocations
Scaphoid > radial styloid > capitate
Trans-scaphoid injuries
- most common
- 2/3 of perilunate dislocations have a scaphoid fracture


Radial styloid fractures


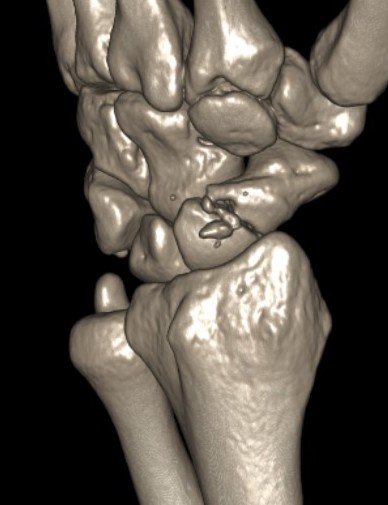
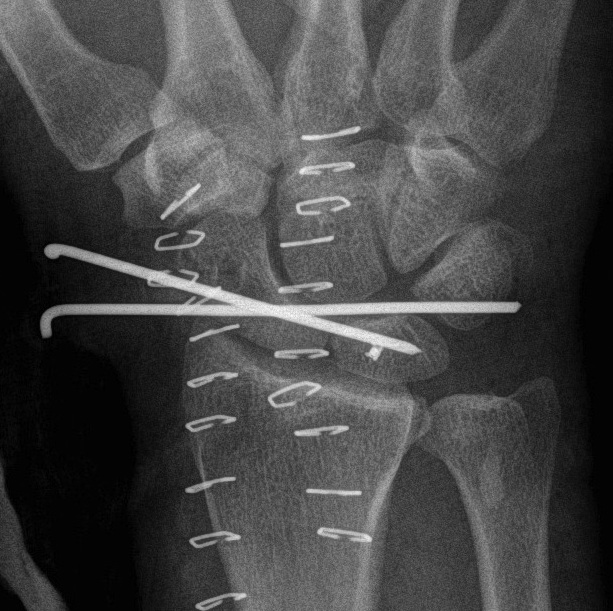
CT




Trans-scaphoid perilunate dislocation


Perilunate dislocation
Acute management
Closed reduction
1. Traction under anaesthesia
- conscious sedation
- finger traps with weight
2. Dorsiflex wrist
- counterpressure on palmar lunate
- gradual wrist flexion with pressure on dorsal capitate
Reduced success rate of closed reduction with dislocated lunate




Jagiella-Lodise et al Hand 2025
- 45 perilunate dislocations
- > 50% presented with median nerve symptoms
- closed reduction successful 80% of time
- closed reduction resolved median nerve symptoms 90% of the time
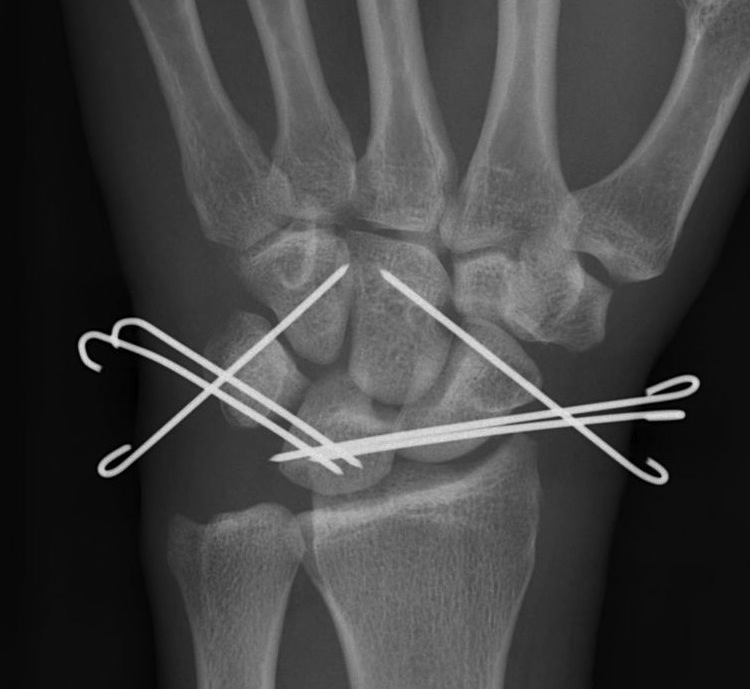
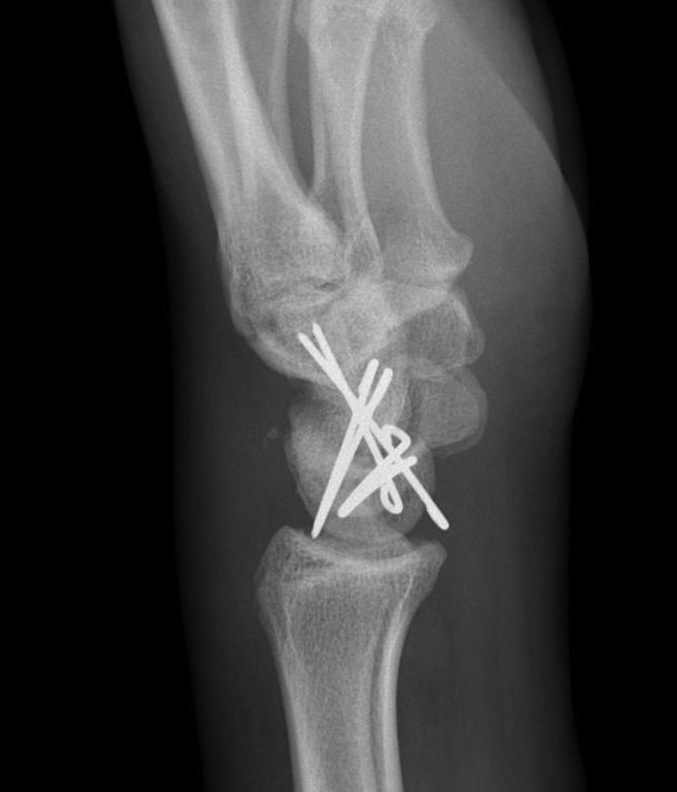
Perilunate dislocation / No scaphoid fracture


Technique
Dorsal approach
- 3/4 extensor compartment
- mobilise EPL laterally
- capsulotomy: T shaped or Berger (open dorsal between DRC and DIC ligaments)
- K wire joysticks in scaphoid and lunate and reduce
- K wires scaphocapitate / scapholunate / lunatetriquetral (areas of ligament rupture)
- +/- repair SL ligament if avulsed from scaphoid or lunate
- +/- repair LT ligament
- +/- reconstruction / internal brace SL and or LT ligament
- +/- SL screw
- +/- capsulodesis / tenodesis
Volar approach indications
- need to open reduce lunate
- perform carpal tunnel decompression
- repair rent in volar capsule / Space of Poirier
AO foundation surgical technique perilunate fractures PDF
Vumedi dorsal approach perilunate dislocation video
Vumedi arthroscopic assisted closed reduction and percutaneous pinning video
www.boneschool.com/scapholunate-ligament-injury
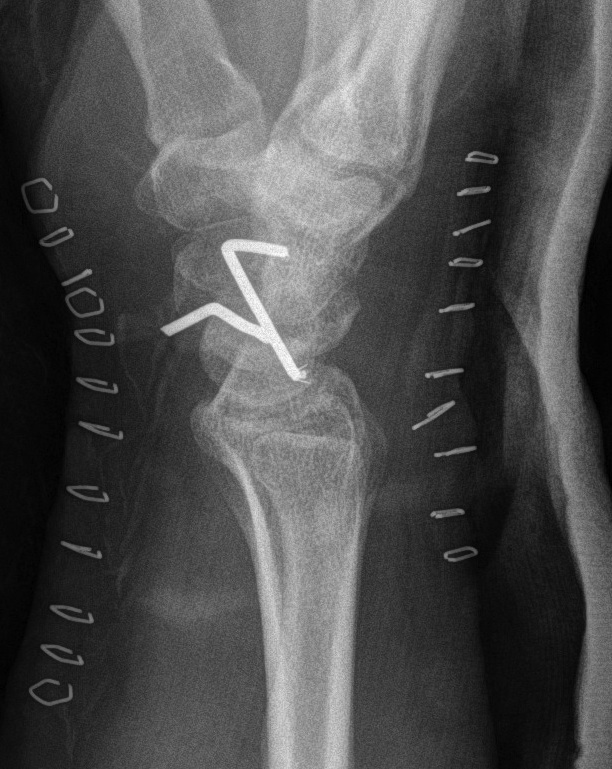


Perilunate fracture-dislocations / Trans-scaphoid perilunate

Dorsal approach
- 3/4 extensor compartment
- mobilise EPL laterally
- capsulotomy: T shaped or Berger (open dorsal between DRC and DIC ligaments)
- ORIF scaphoid fracture with headless compression screws
- assess stability of scapho-capitate and scapholunte joint (often ligaments intact and stable)
- K wires lunate-triquetral +/-
- +/- repair LT ligament
- +/- ORIF capitate


+/- volar approach
- reduce lunate
- carpal tunnel decompression
- repair rent in capsule
Youtube trans-scaphoid perilunate fracture dislocation video
Youtube trans-scaphoid perilunate fracture dislocation video 2




Results
Timing of surgery
van der Oest et al J Wrist Surg 2021
- systematic review
- best outcomes with surgery < 7 days
- worst outcomes with surgery > 6 weeks
Outcomes
Liechti et al Eur J Trauma Emerg 2023
- systematic review of 26 studies and 550 patients
- average ROM 75% of contralateral side
- average grip strength 75% of contralateral side
- mean Mayo outcome score 77 / fair
Approach
- systematic review of outcomes with dorsal / volar / combine approaches
- no difference in
Complications
Lee et al J Hand Surg Eur 2023
- systematic review of 43 studies and 800 patients
- osteoarthritis 30%
- carpal instability 15%
- lunate AVN 12%
- CRPS 11%
- scaphoid nonunion / AVN 9%
Loss of reduction
Liechti et al Eur J Trauma Emerg 2023
- systematic review of 26 studies and 550 patients
- complication rate 15%
- most common complication loss of reduction 10%
- loss of reduction perilunate dislocation: 24%
- loss of reduction perilunate fracture dislocation: 7%
- increased complication rate with combine volar dorsal approach versus isolated dorsal approach




Loss of reduction with proximal pole scaphoid AVN and lunate AVN
Chronic unreduced perilunate dislocations
Chronic presentations
Missed in 20%
- reasonable ROM
- little pain
May present with median nerve symptoms
May present with flexor tendon ruptures
Options
Open reduction
Scaphoidectomy + 4 corner fusion
Proximal row carpectomy
Wrist arthrodesis