
Definition
Recurrent lateral dislocation /subluxation of patella with minimal trauma
Epidemiology
Females > Males
2nd - 3rd decade
Anatomy
| Facets | Static constraints | Dynamic constraints |
|---|---|---|
| Medial and lateral facet | Bony - prominence of lateral femoral condyle | Quadriceps / VMO |
| Lateral larger | MPFL |
Etiology Patella Instability
Multifactorial / Combination of
- valgus malalignment
- ligamentous laxity
- MPFL tears
- Trochlea dysplasia
- Patella alta
- Abnormal rotational profile (femoral anteversion / external tibial torsion)
Examination
Ligamentous laxity / Beighton score > 4
- hyperextension of the MCP joints beyond 90o
- touch thumb passively to forearm
- elbows hyperextend beyond 0o
- knees hyperextend beyond 0o
- palms flat on floor while knees straight (1)




Patella Tracking / J Sign
- patient sitting over side of bed
- flex and extend knee
- lateral subluxation of patella as knee approaches full extension
![]()
![]()
Q (quadriceps) angle
- knee flexed 30o over pillow or examiner knee
- line from ASIS to centre of patella
- line from centre of patella to tibial tuberosity
- angle between lines is Q angle
- abnormal: > 15o in males and > 20o in females


Patella mobility
- knee flexed 30o over pillow or examiner knee
- move patella medially and laterally
- graded in number of quadrants patella displaces
- lateral glide: >3 quadrants suggests incompetent medial restraints
- medial glide: < 1 suggests tight lateral retinaculum


Apprehension test
- push patella laterally
- patient feels apprehension due to patella instability
External tibial torsion
- intermalleolar axis > 30o
- thigh foot angle > 15o


Thigh-foot angle
Femoral anteversion
- patient prone
- hip internal rotation > 15o

Increased femoral anteversion on left
Investigations
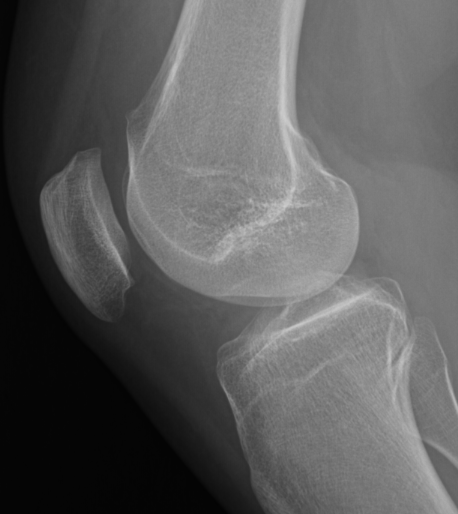
Patella alta
30o flexion lateral xray
| Blumensaat's line | Blackburn-Peele ratio | Insall ratio |
|---|---|---|
|
Cross inferior pole of patella |
Distance between - tibial and patella articular surface - divided by length of patella articular surface |
Length of patella tendon / length patella |
|
Pole above line - alta Pole below line - baja |
Patella alta > 1 |
Patella alta 1.2 Patella baja < 1 |
 |
 |
 |
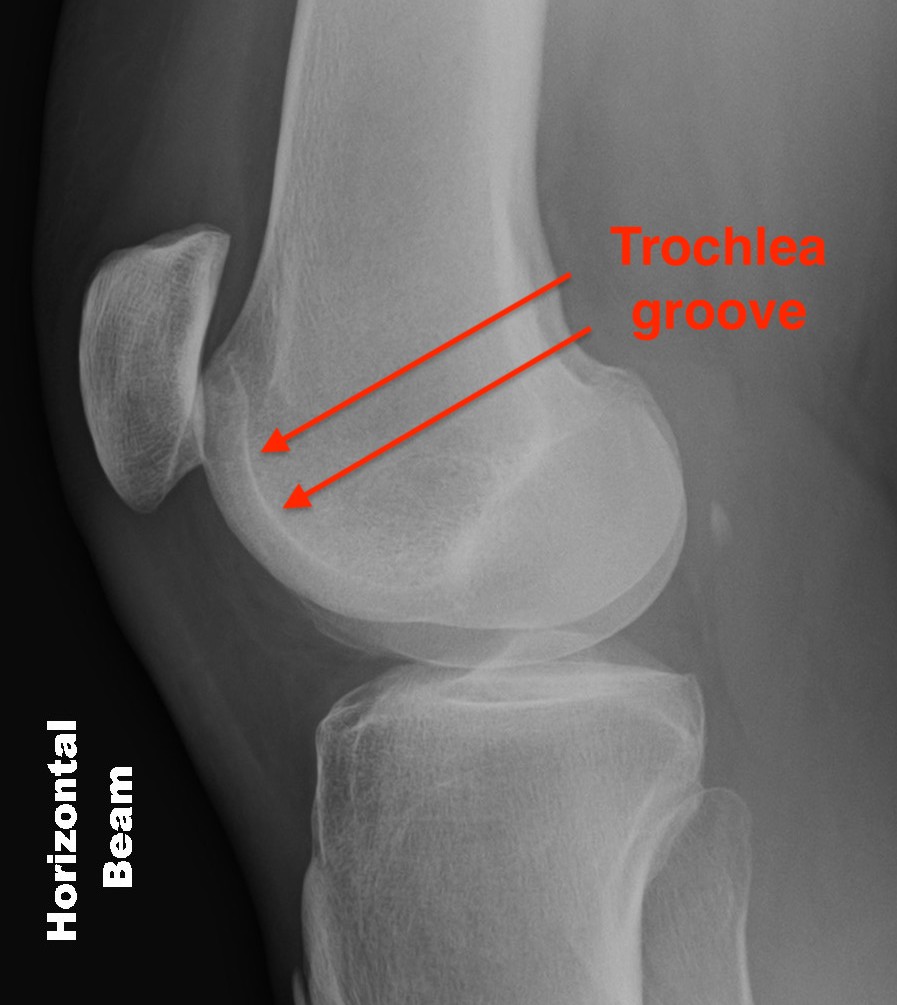
TT-TG
Tibial Tuberosity Trochlea Groove (TTTG)
- superimpose 2 axial slices
- axial slice of trochlea
- line perpendicular through trochlea groove
- perpendicular line through tibial tuberosity
- distance between two lines
There are no absolute cut offs for instability, or to guide surgery


- MRI of 87 patella instability patients and 500 non patella instability in pediatric patients
- control group: mean TTTG 8 mm
- instability group: mean TTTG 16 mm
- systematic review of TTTG CT versus MRI
- measured TTTG on CT greater than on MRI
- CT control group: mean TTTG 13 mm
- CT instability group: mean TTTG 18 mm
- MRI control group: mean TTTG 10 mm
- MRI instability group: mean TTTG 15 mm
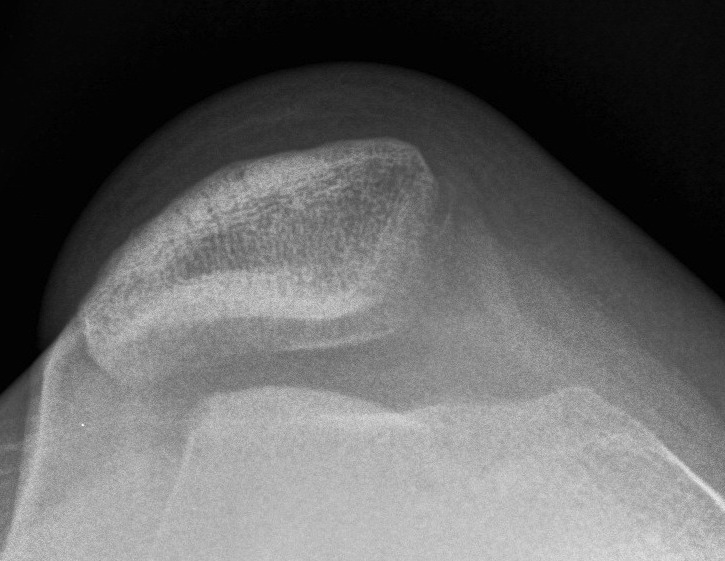
Trochlea Dysplasia
Dejour Crossover Sign
- lateral x-ray at 30o with condyles superimposed
- identify base of trochlea
- normal: clearly defined trochlea groove
- abnormal / Crossover: line of floor of trochlea crosses lateral lip of condyle

Normal trochlea / no crossover


Crossover with supratrochlear spur

Crossover with large supratrochlear spur
Trochlea dysplasia / Sulcus angle
- normal < 140o
- > 140o flattened

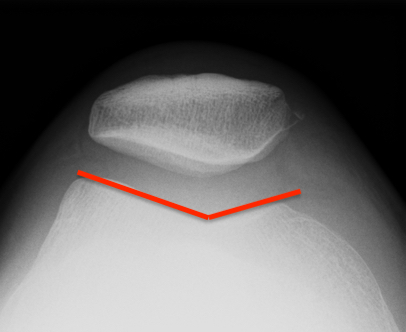
Normal trochlea / sulcus

Trochlea dysplasia with reduced sulcus angle
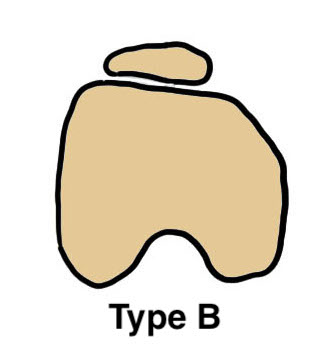
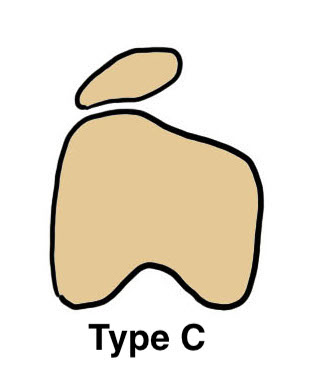
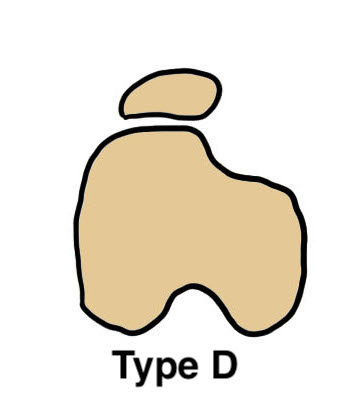
Dejour trochlea dysplasia classification
Type A: Shallow trochlea
Type B: Flat trochlea groove with trochlea spur
Type C: Lateral trochlea convex, hypoplastic medial trochlea
Type D: Trochlea spur + cliff like fall off between lateral and medial trochlea
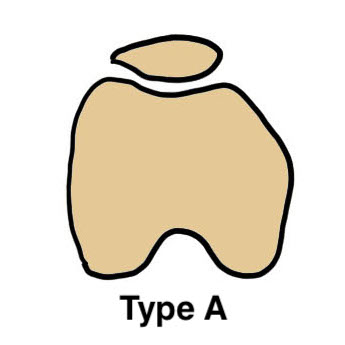

Type A

Type B
Type C
Type D
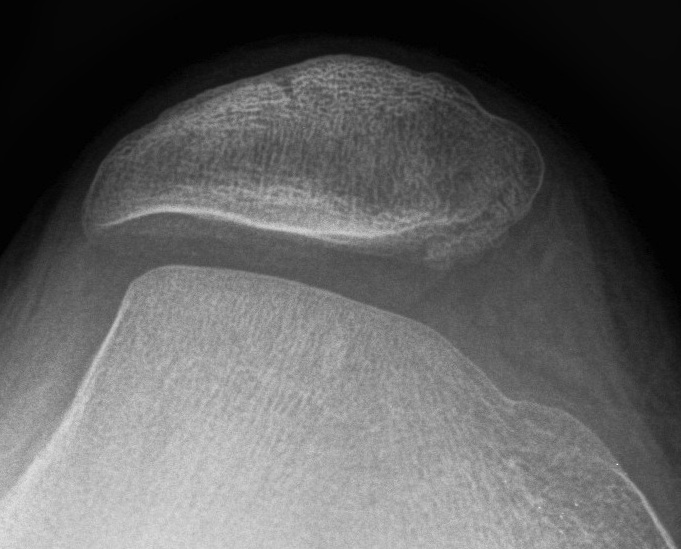
Other findings on imaging
Xray
Bony MPFL avulsion


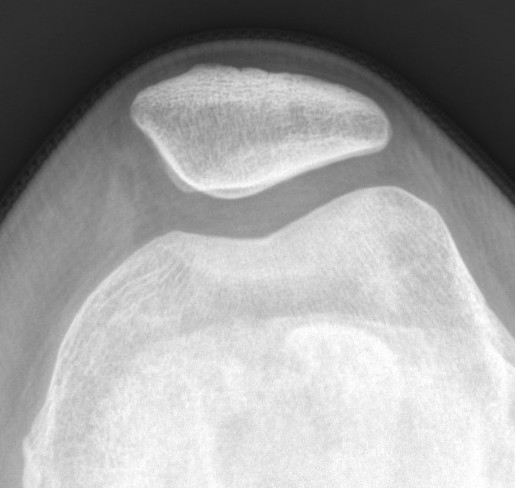
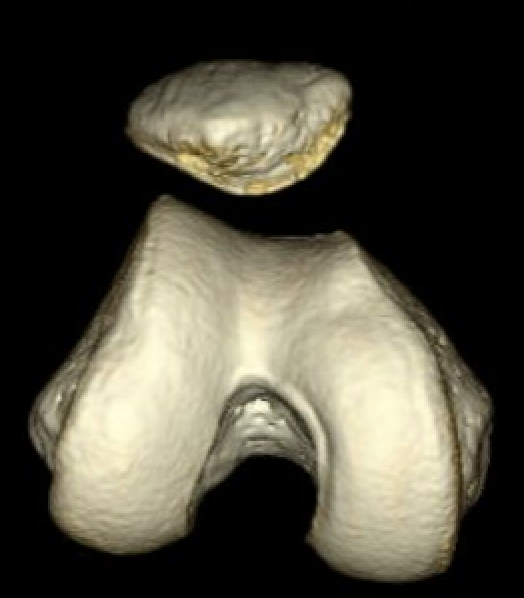
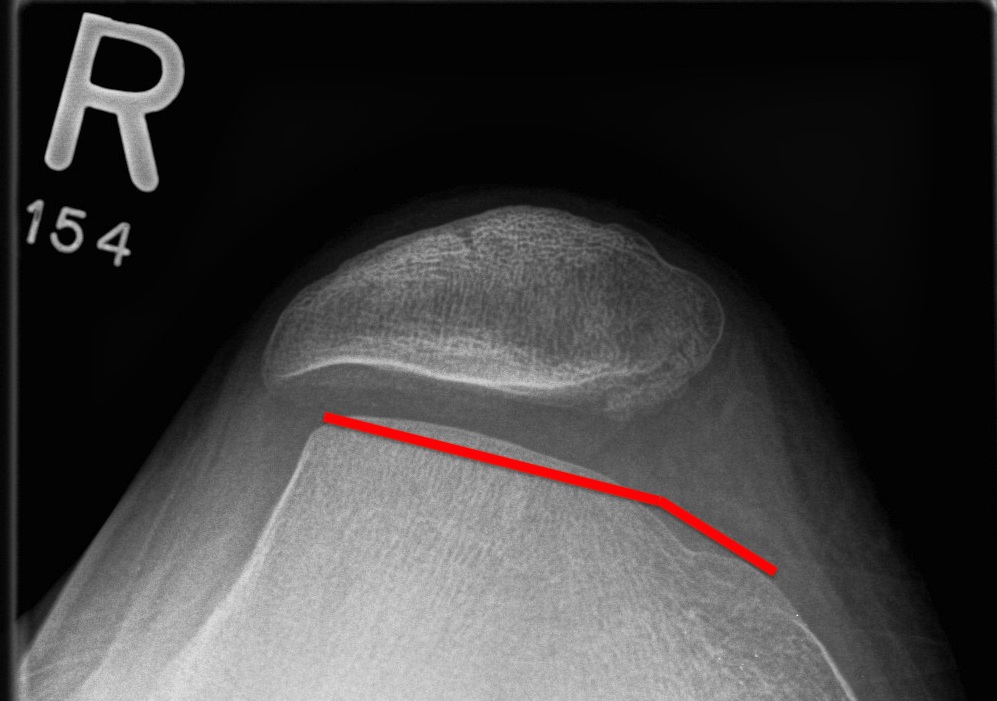
Patella subluxation
Patella should be well engaged in groove
Central ridge should lie at or medial to bisector of the trochlea groove
Patella well engaged in groove versus laterally subluxed patella
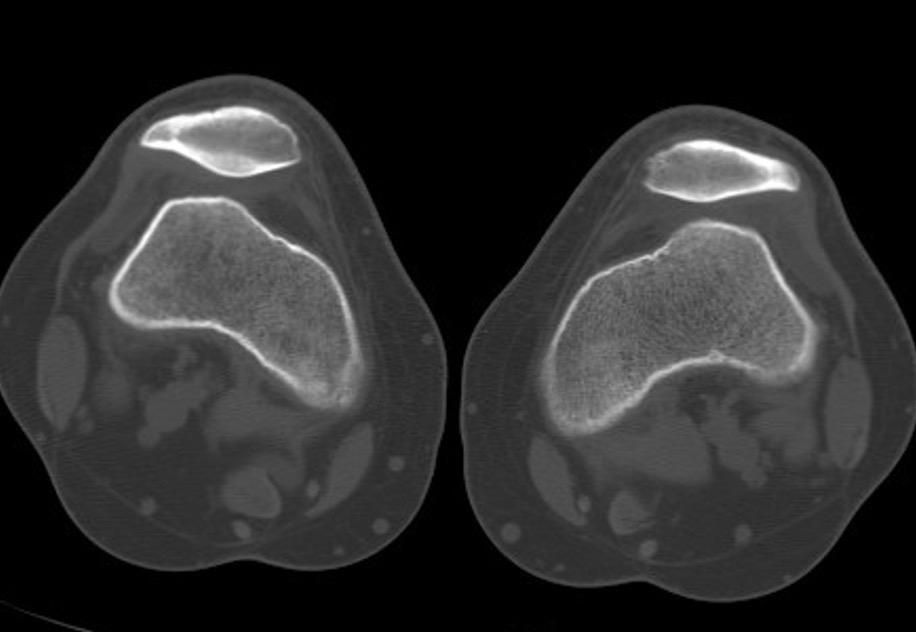
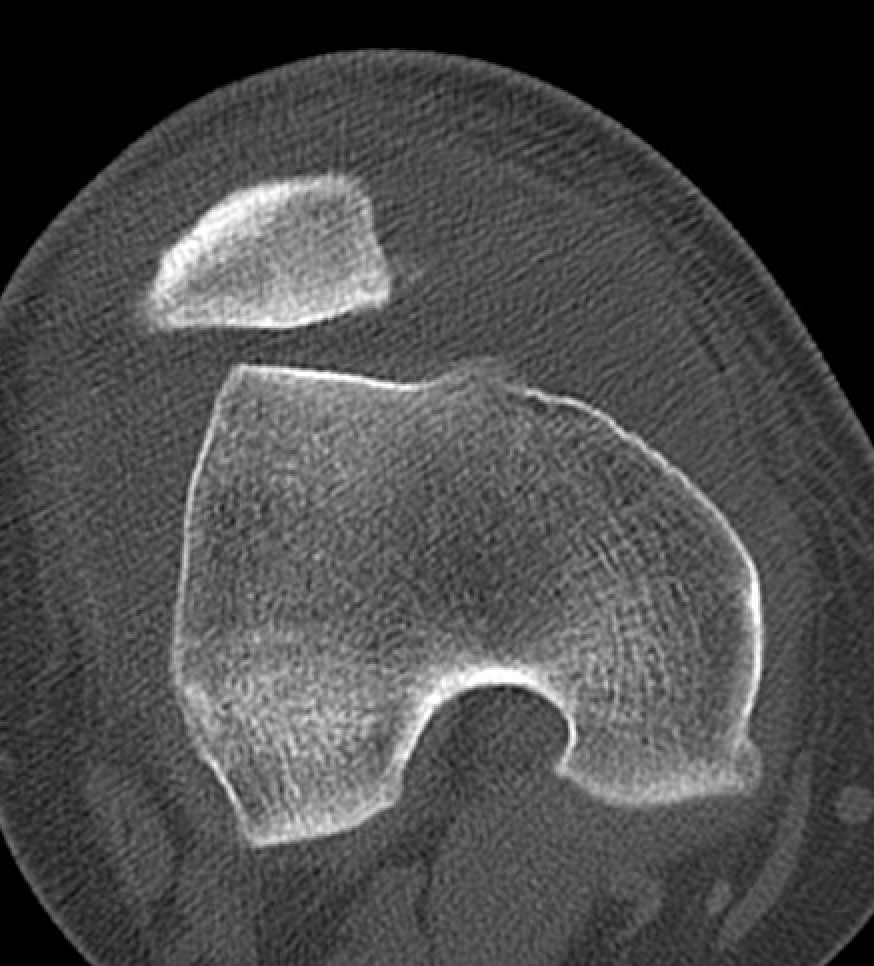
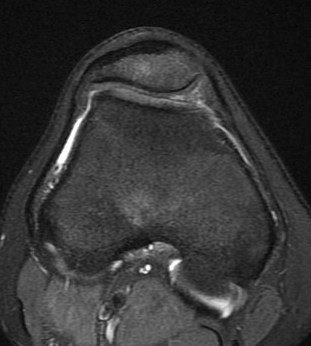
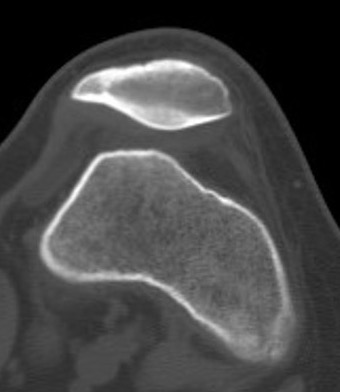
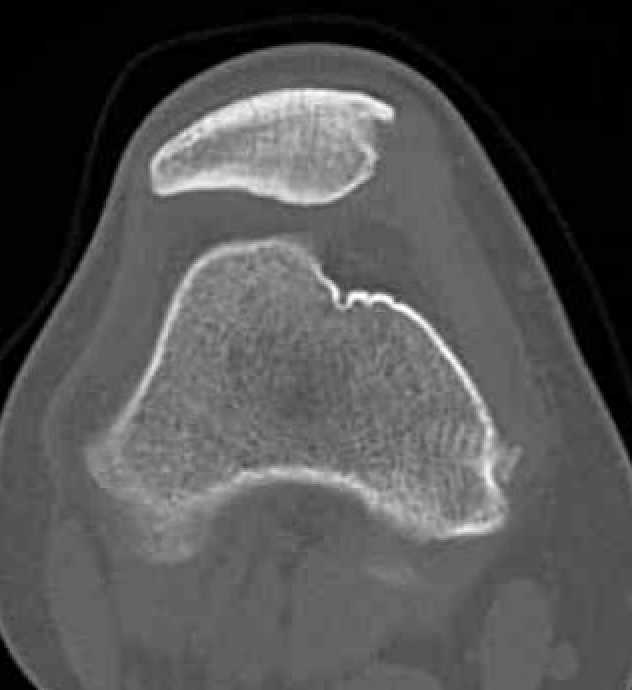
CT
Lateral subluxation with Type C trochlea dysplasia
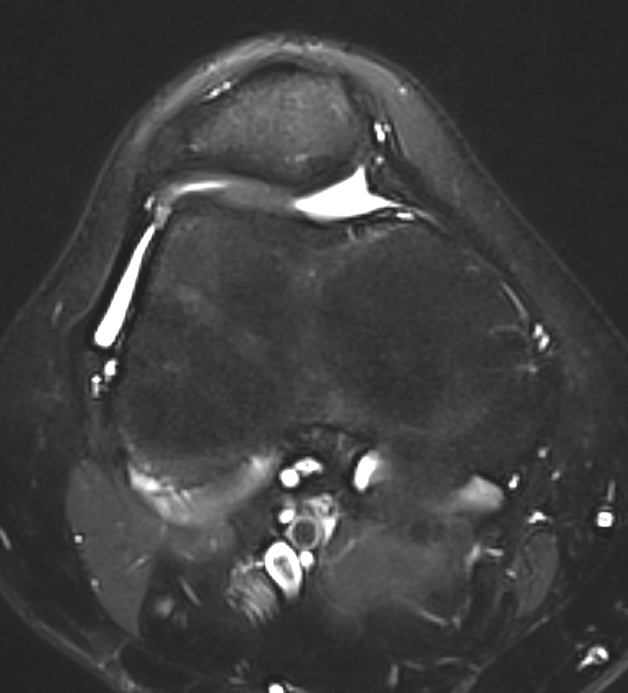
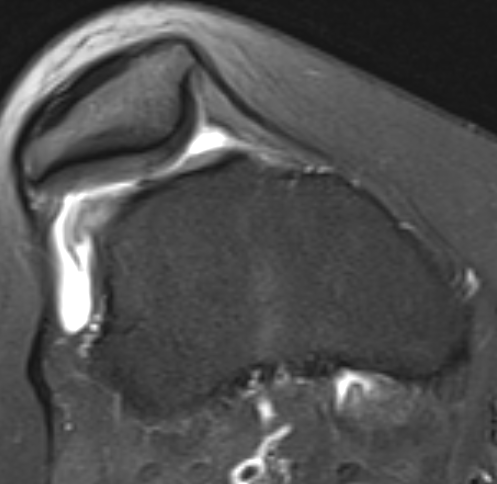
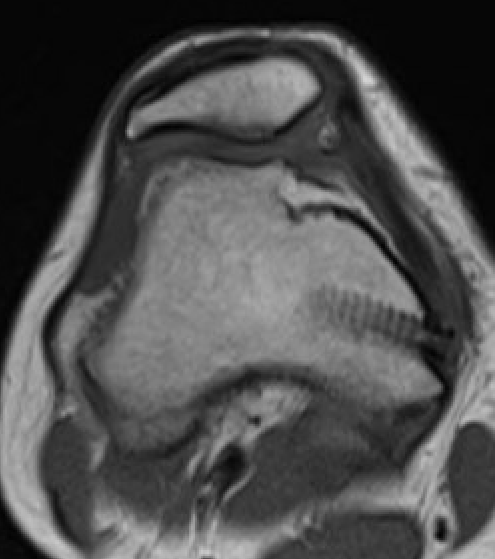
MRI
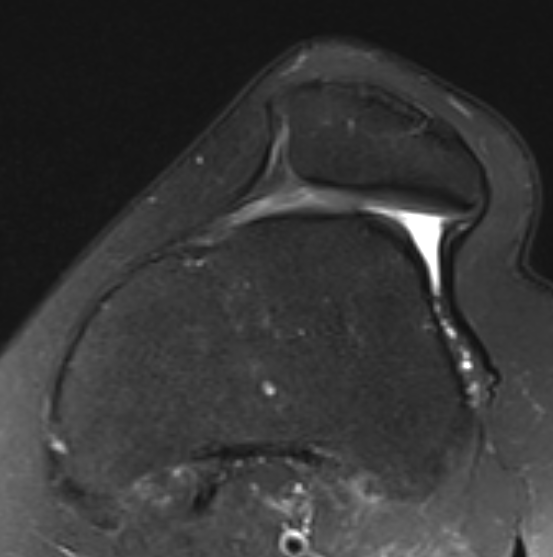
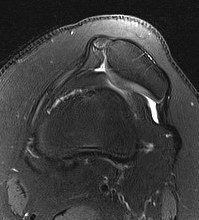
Lateral subluxation with trochlea dysplasia type B
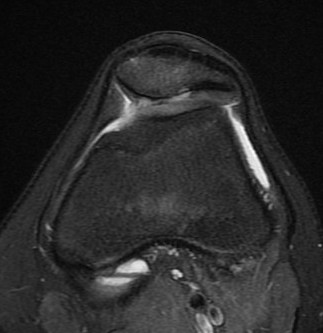
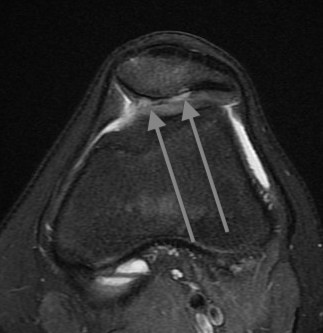
Articular cartilage damage on patella