


Indications
Recurrent disabling patella instability
Options
MPFL reconstruction
Tibial tuberosity osteotomy
Trochleoplasty
Derotation osteotomy
Results
MPFL v MPFL + TTO
- systematic review of isolated MPFL v MPFL + TTO
- 31 studies and 1400 patients
- isolated MPFL: mean Kujala 85, redislocation 3%
- MPFL + TTO: mean Kujala score 84, redislocation 3%
TTTG > 20
- systematic review of isolated MPFL v MPFL + TTO with TTG > 20
- 13 studies and 400 knees
- no difference in redislocation rates or complications
- improved Kujala scores with isolated MPFL
MPFL reconstruction
Indication
Mild patella instability
TTTG < 20
Options
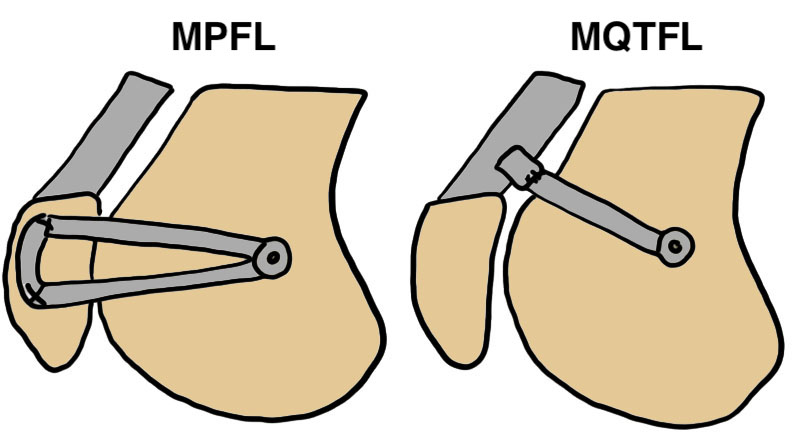
MPFL reconstruction - use graft to connect femur to the patella
Medial quadriceps tendon femoral ligament (MQTFL) - use graft to connect femur to the quadriceps tendon
Combined
MPFL technique

Patella inlay with tunnel/screw versus patella onlay technique with suture anchors
Vumedi MPFL reconstruction with hamstring autograft video
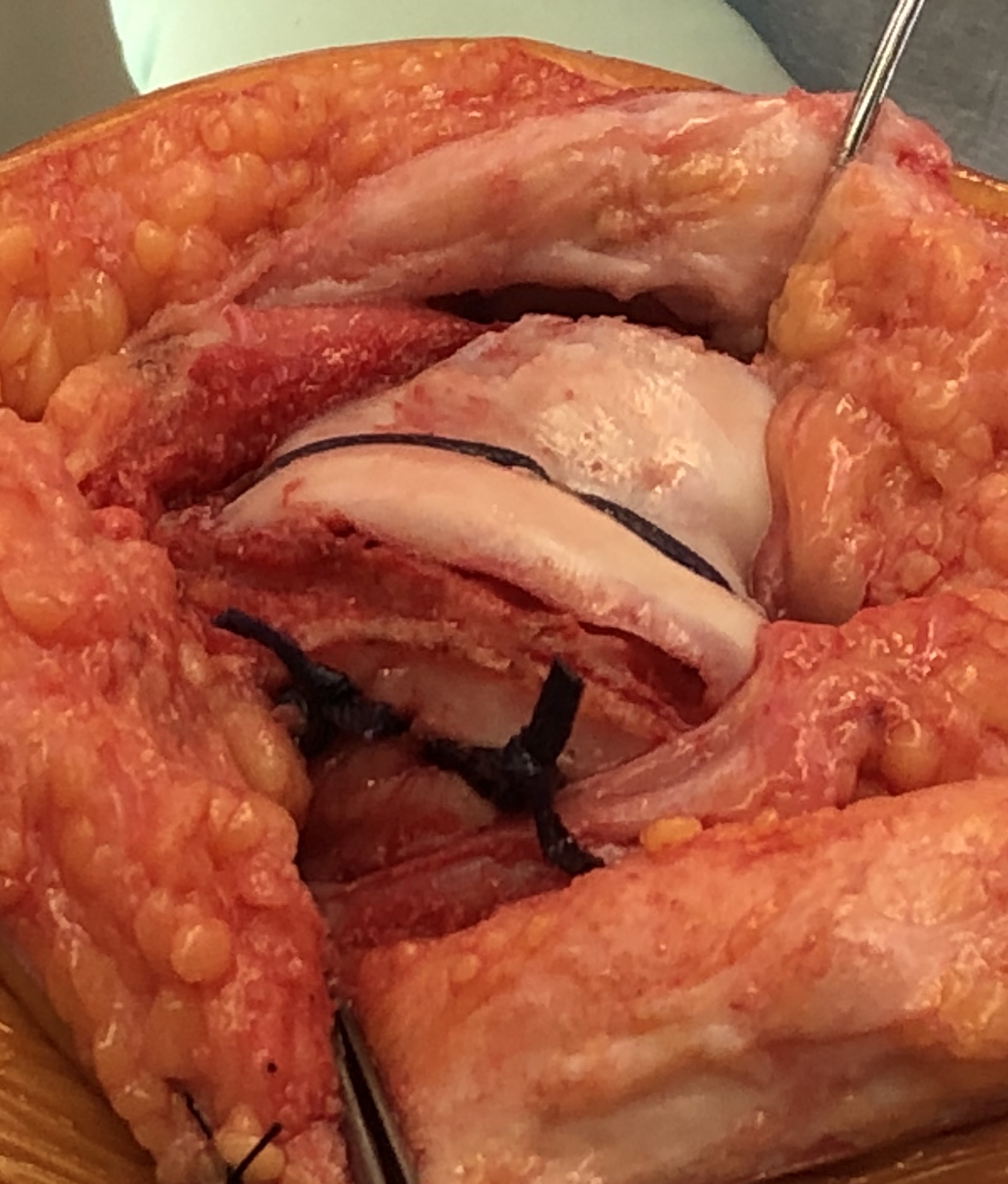
Patella
- expose medial patella
- identify superior half of patella
- fixate graft with screws / bone anchors
- identify layer between medial retinaculum and capsule
- pass graft superficial to capsule
Schottle's Point
- radiographic landmark for isometric insertion point MPFL on femur
- 1 mm anterior posterior cortex
- 2 mm distal to MFC origin
- proximal to Blumensaat's line

Femur
- dissection down to bone
- protect saphenous nerve
- use xray to find Schottle's point
- aim femoral pin anterior to Blumensaat's line / 30o
- drill for size of graft
- pass graft and fixate with screw


Results
MPFL reconstruction
- systematic review of isolated MPFL for recurrent patella instability
- mean postoperative Kujala score 86
- 84% return to sports
- recurrent instability 1%
- positive apprehension sign 4%
- reoperation rate of 3%
Autograft versus allograft
Perez-Espina et al J Pediatr Orthop 2026
- systematic review of MPFL autograft v allograft in adolescents
- 23 studies and 800 knees
- autograft: recurrent dislocation 6%, return to sport 71%
- allograft: recurrent dislocation 9%, return to sport 91%
Patella tunnel versus suture anchor fixation
- 46 MPFL reconstruction using transosseous tunnel versus suture anchors on patella
- transosseous tunnel: 2 patella fractures, 1 redislocation
- suture anchor fixatiion: 0 patella fracture, 0 redislocation
MQTFL reconstruction
Technique
Results
Migliorini et al Eur J Orthop Surg 2026
- systematic review of MQTFL for 300 knees
- recurrent instability 6%
- reoperative rate 2%
Complications
Anterior femoral tunnel

Infection


Patella fracture



Tibial Tuberosity Osteotomy


Indication
TTTG > 20
Severe lateral patella subluxation
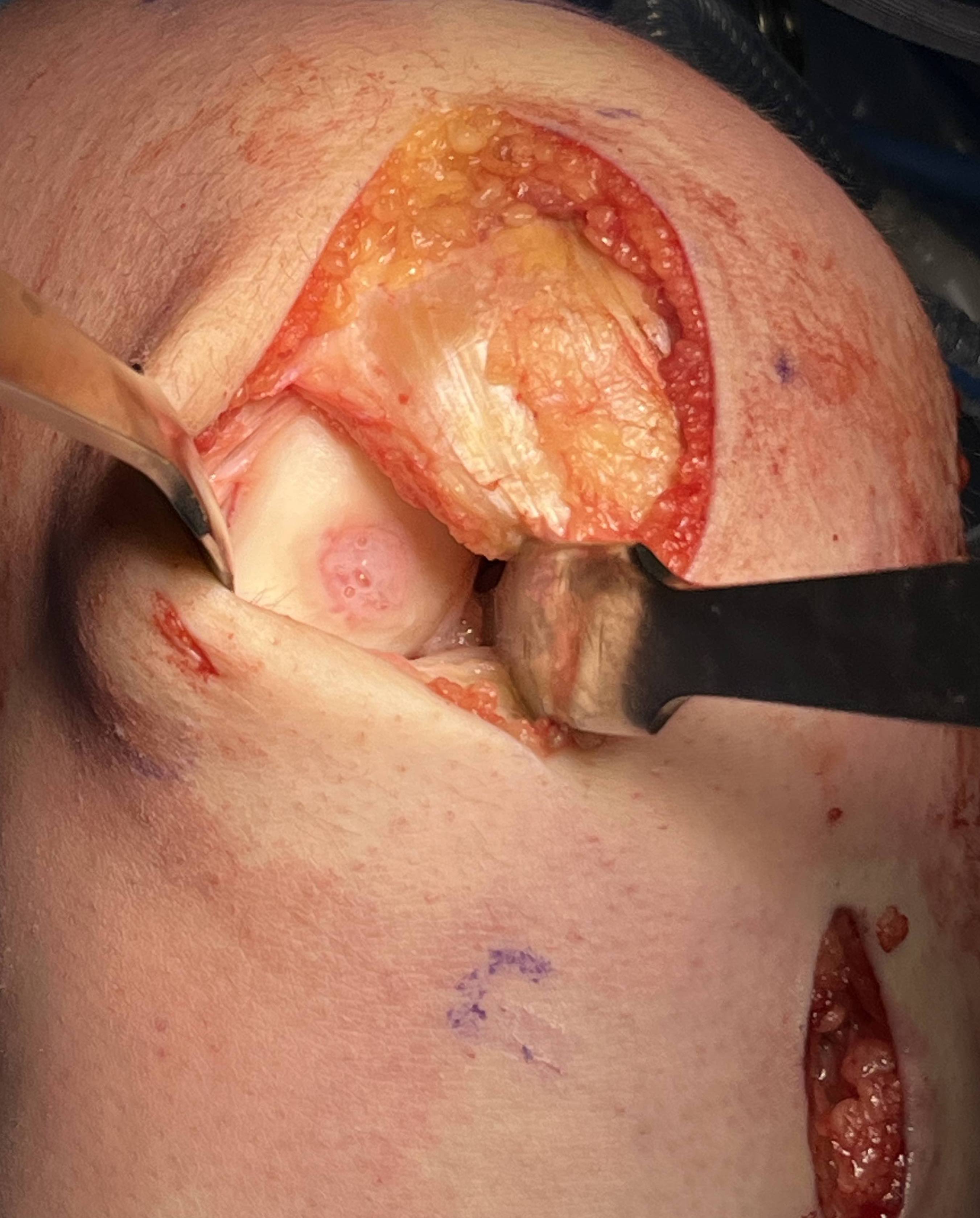
Technique
Vumedi tibial tuberosity osteotomy v+ MPFL video
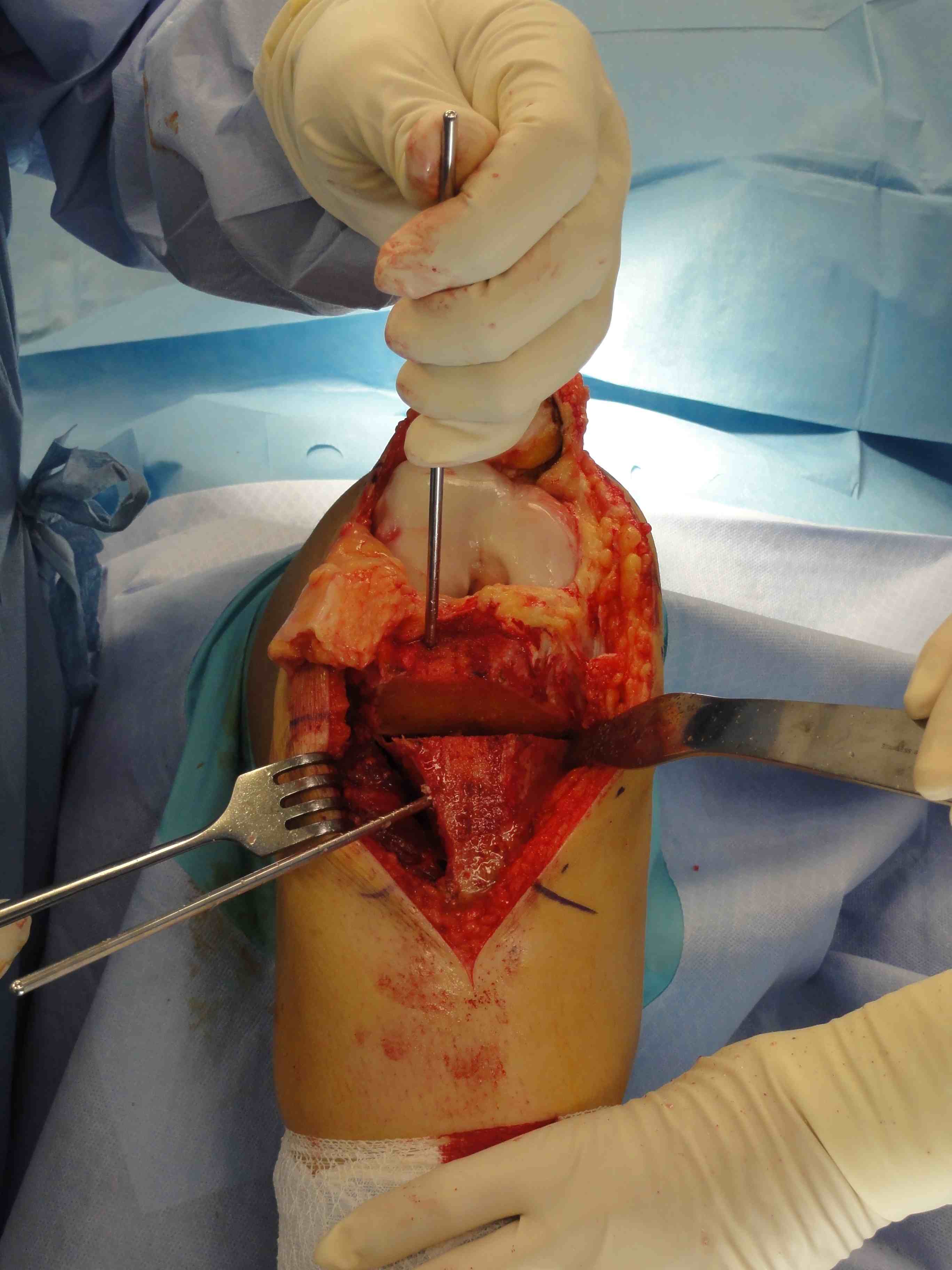
Tibial tuberosity osteotomy
- incision midline over tibial tuberosity
- expose tibial tuberosity medial and laterally
- identify and protect patella tendon insertion
- often need lateral release to reduce patella
- insert K wires to guide osteotomy
- some obliquity to allow antero-medialisation
- osteotomy 1 cm deep, 6 cm long
Lateral release
- usually need large lateral release in severe cases
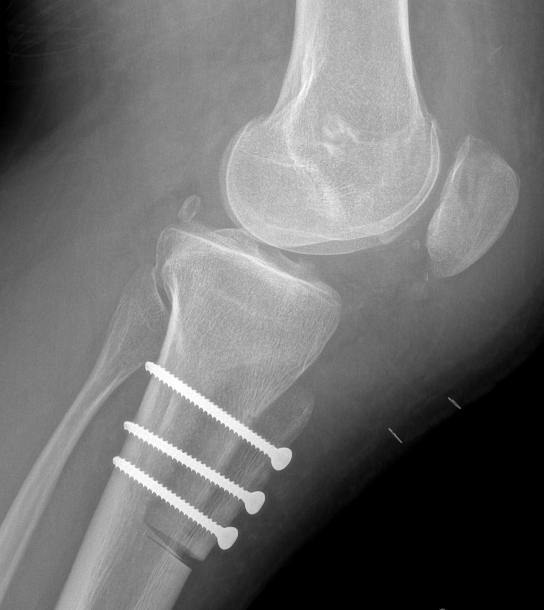
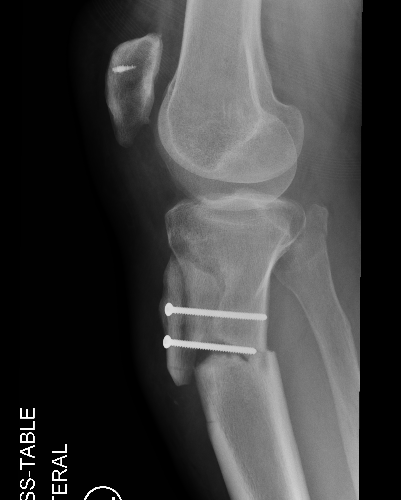
Distalization
- can resect 1 cm off the tibial bone block
- allows distalization of the tibial tuberosity osteotomy
- pulls tibia down into the groove



Distalization by resecting 1 cm from bone block and distalizing tibial tuberosity


Post tibial tuberosity osteotomy with distalization
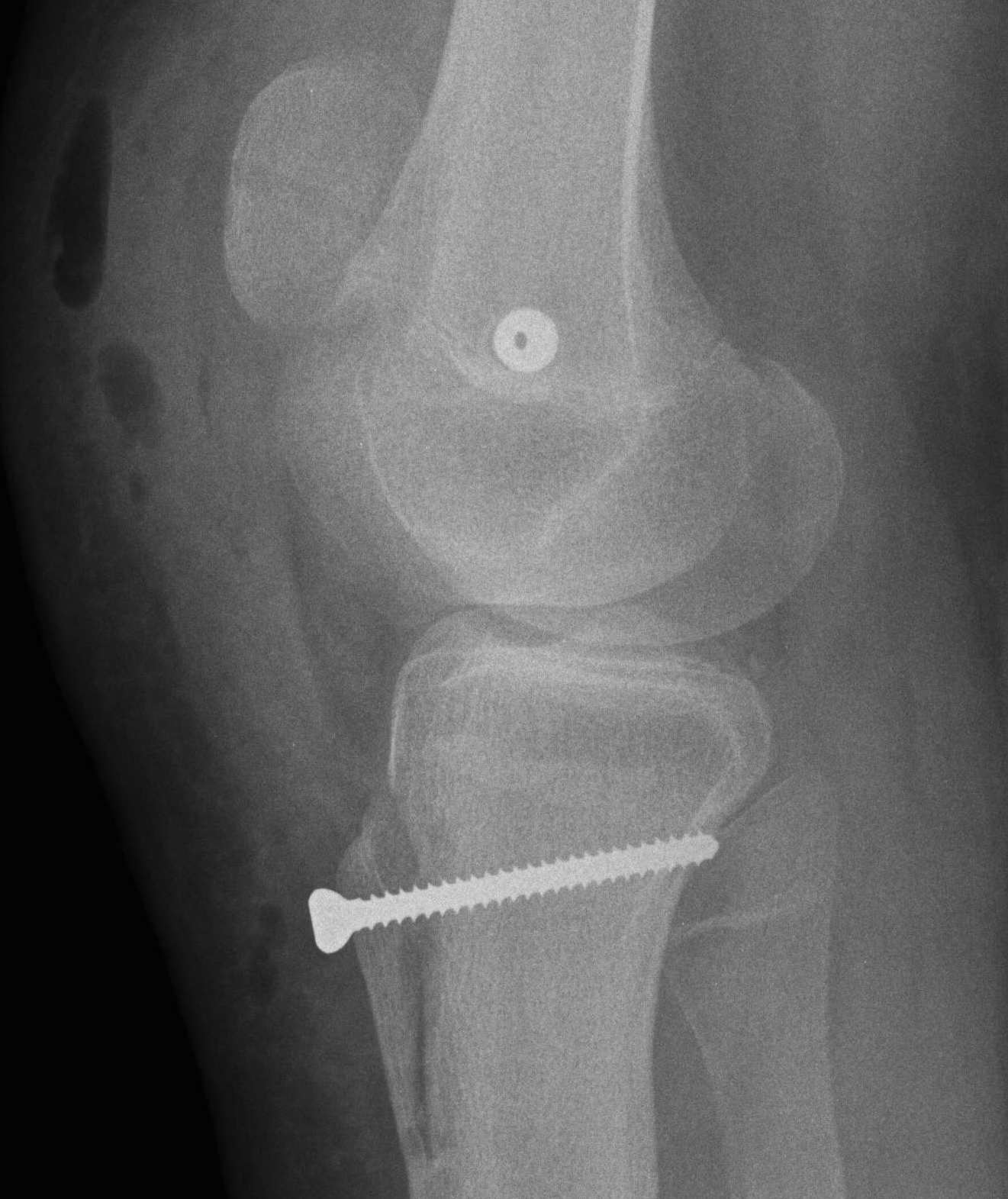
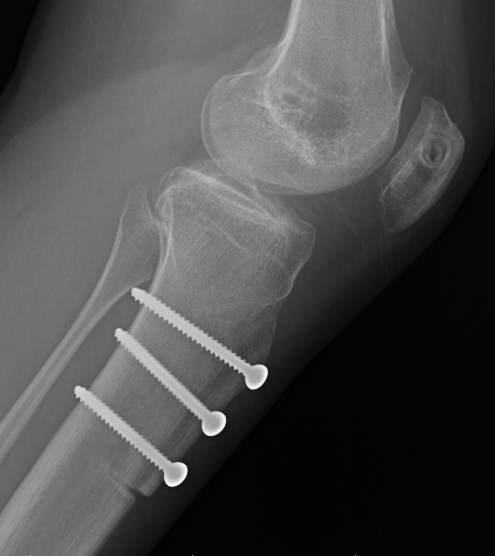
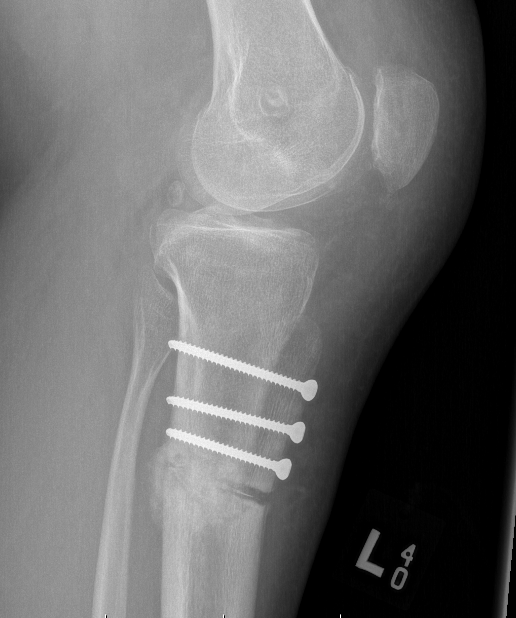
Fixation
- secure with 2 or 3 bicortical 4.5 mm fully threaded screws with lag screw technique
- +/- distal plate over osteotomy to minimize stress fracture risk


MPFL reconstruction
- standard technique as above
- hamstring / medial patella anchors / femoral fixation Schottle's point


Patella femoral chondral defects
Consider cartilage regeneration procedure
- microfracture / MACI / de novo / AMIC
www.boneschool.com/knee-cartilage-defects

Results
Complications
Berk et al Orthop J Sports Med 2023
- review of 344 TTO
- stiffness 16%
- superficial infection 8%
- hemarthrosis 6%
Periprosthetic fracture



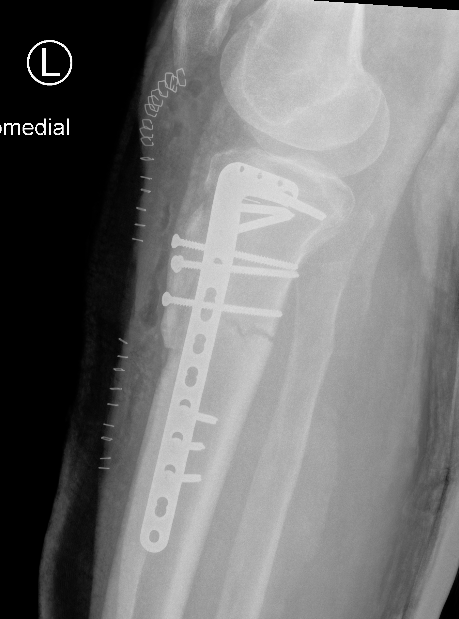


Use of distal plate to avoid stress riser
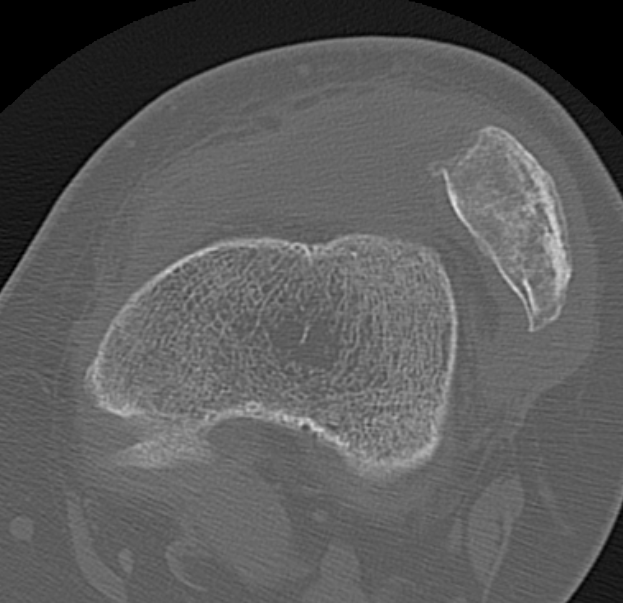
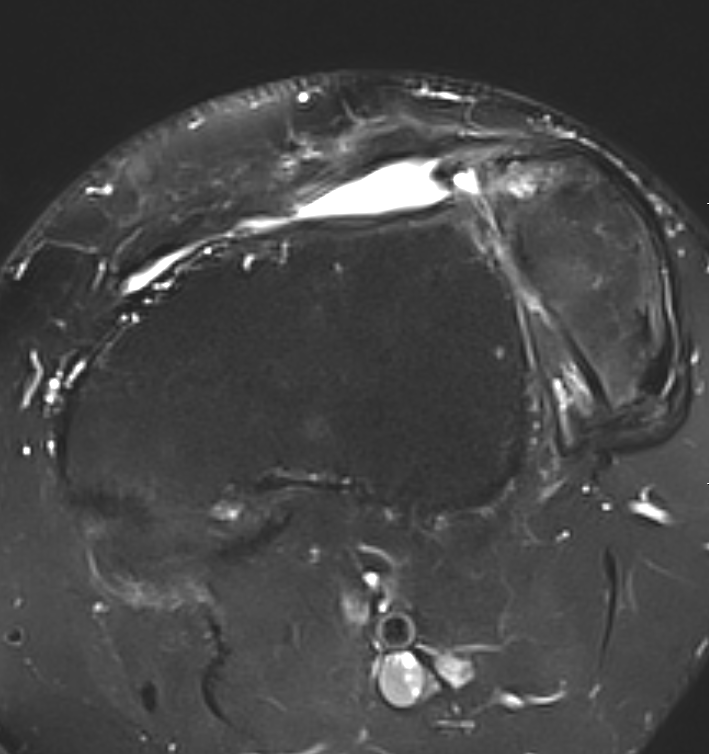
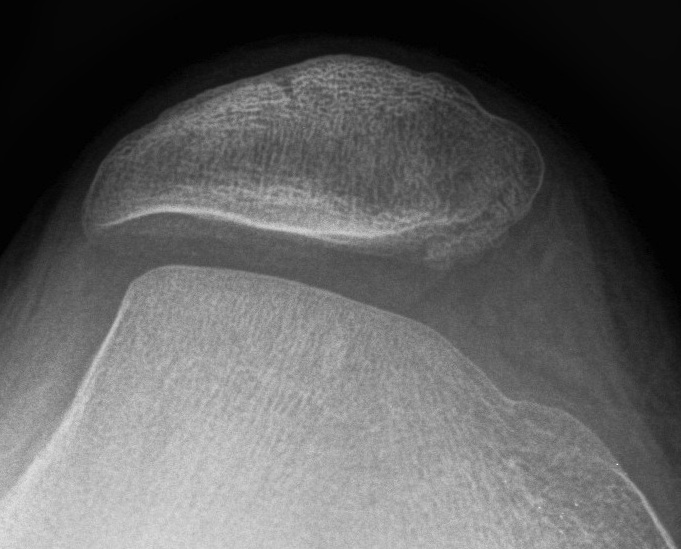
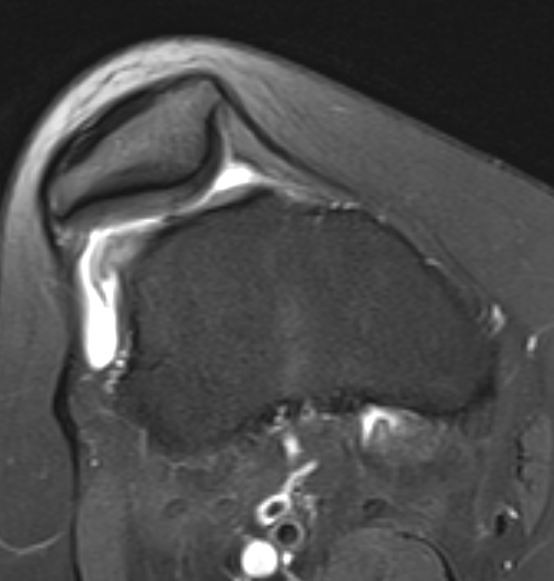
Trochleoplasty


Indication
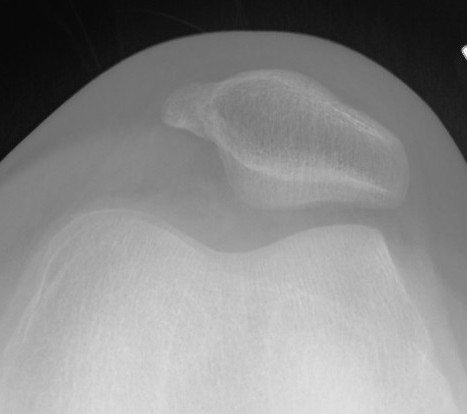
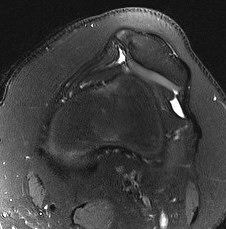
Trochlea dysplasia

Options
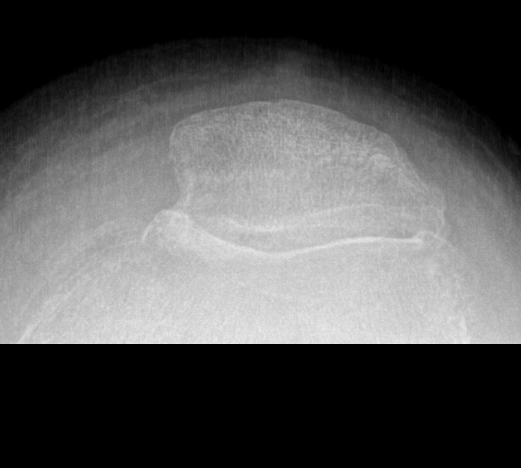
1. Sulcus deepening of trochlea - Dejour
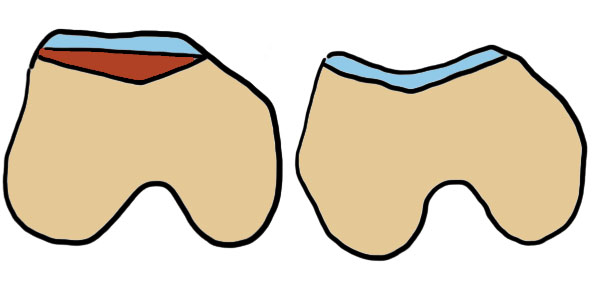
2. Lateral condyle elevation and bone graft - recreate groove

3. Lateral condyle / lateral bump reduction
Techniques
Vumedi Dejour sulcus deepening trochleoplasty video
Arthroscopy techniques sulcus deepening trochleoplasty + MPFL
Arthrex trochleoplasty techniques
Results
Trochleoplasty v Tibial tuberosity osteotomy
- systematic review of trochleoplasty v TTO in setting of trochlea dysplasia
- 10 studies and 360 knees
- TTO: 21/230 (9%) recurrent instabilty
- trochleoplasty: 3/132 (2%) recurrent instability
Femoral derotation osteotomy
Indication
Increased femoral anteversion
Results
- 144 patients treated with MPFL + TTO
- poorer outcome scores with femoral anteversion > 30 degrees
- systematic review of FDRO + MPFL
- better outcome scores with combined surgery in setting of increased femoral anteversion
- no nonunion
Tibial Derotation Osteotomy
Indication
Excessive external tibial torsion > 30 degrees
1 / 5000 people


Results
- tibial derotation osteotomy for 15 knees with external tibial torsion and patella instability
- mean age 34, mean preoperative ETT was 62 degrees
- 2 nonunions - one bone grafted, one revised to TKA
- systematic review of derotation tibial osteotomy for PFJ instability
- 8 studies and 245 knees
- 94% patient satisfaction