Types
| Infantile | Adolescent |
|---|---|
|
Onset 1 - 3 years Bilateral Most common |
Onset > 6 years Unilateral Rare |
Definition
Infantile tibia vara
- progressive varus deformity of knees
- secondary to abnormality of medial upper tibial physis
Epidemiology
African descent / females / obesity / bilateral
Etiology
Disruption of normal medial endochondral bone formation
Unknown / multifactorial
- genetic and racial predisposition
- abnormal compression on medial side of proximal tibial physis
- obesity
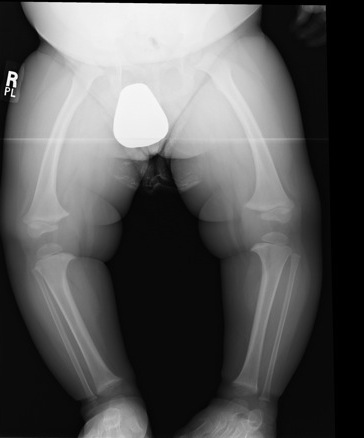
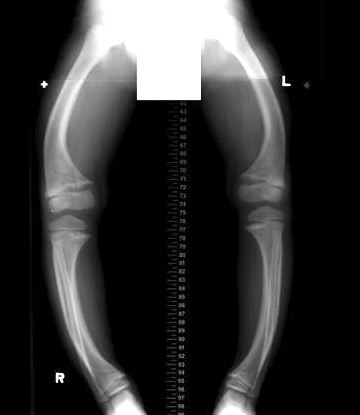
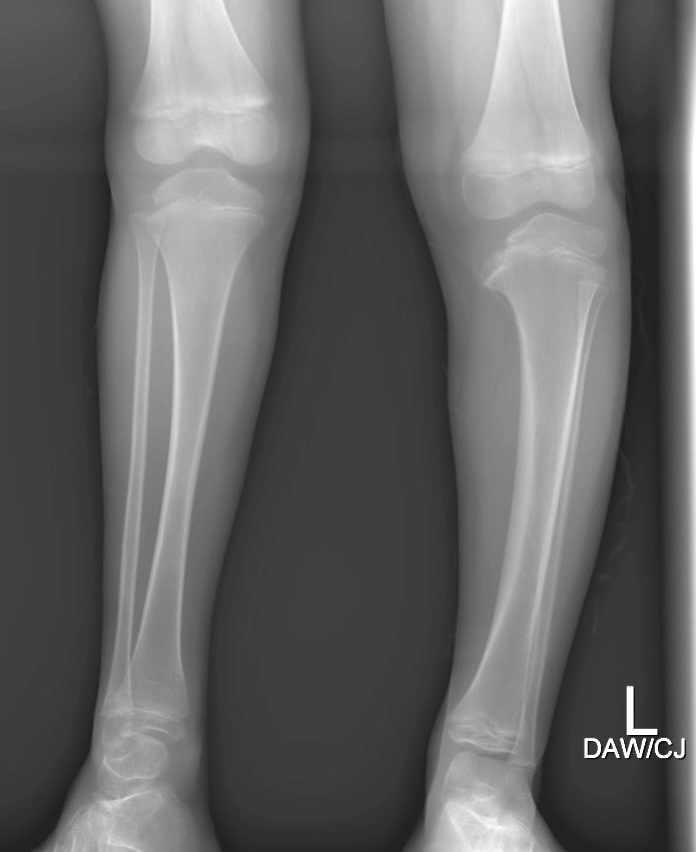
Clinical
Bilateral & symmetrical bowing
- age 1 - 3
- walking
- normal physiological varus should resolve by age 2
Varus knee
Internal tibial torsion - due to the tethering affect of the fibula
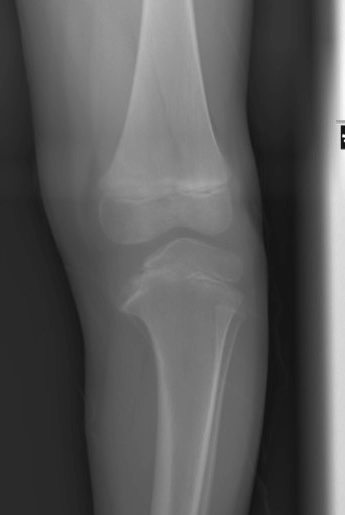
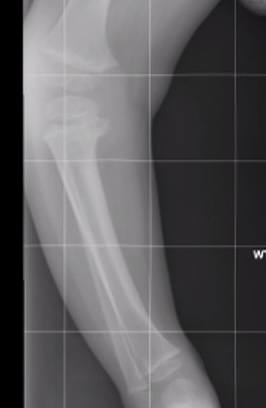
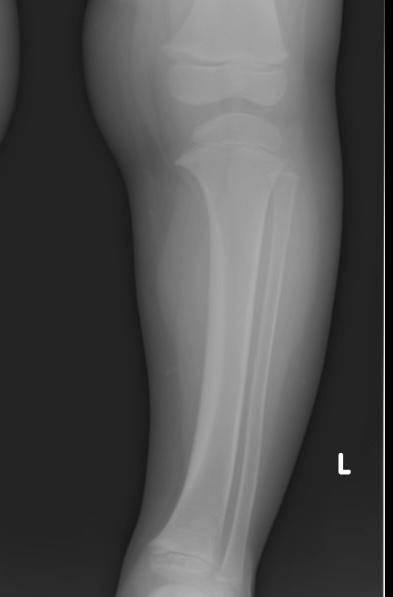
X-ray

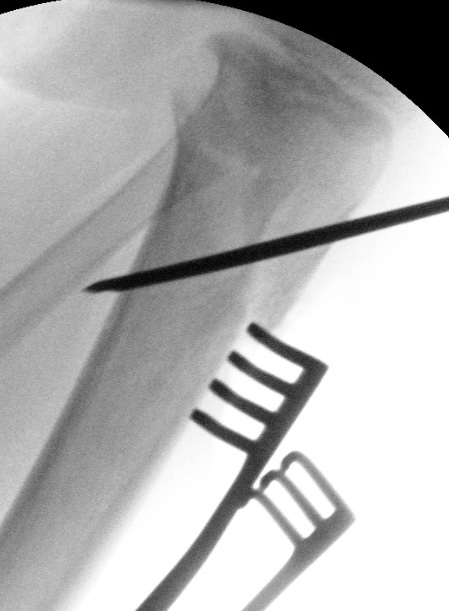
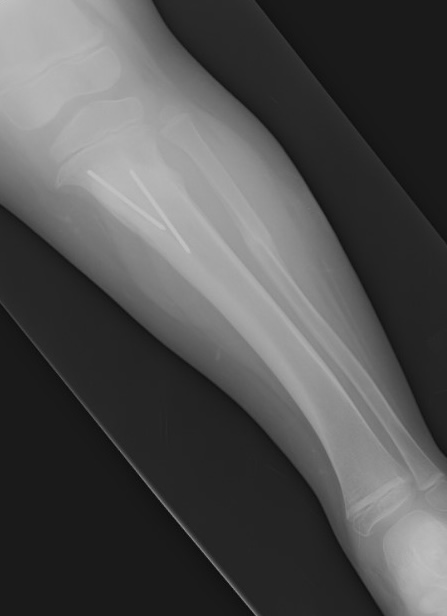
Findings
- medial beaking of the epiphysis
- widened and irregular medial physis
- medial sloping of the epiphysis
- metaphyseal varus
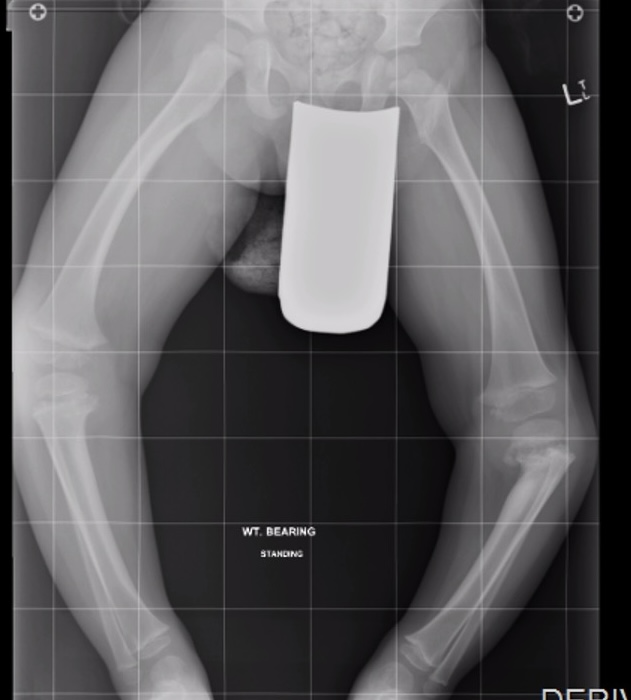
Severe knee varus / lateral thrust / lateral collateral ligament insufficiency
Distal femoral varus also common



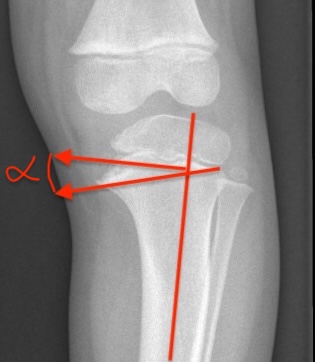
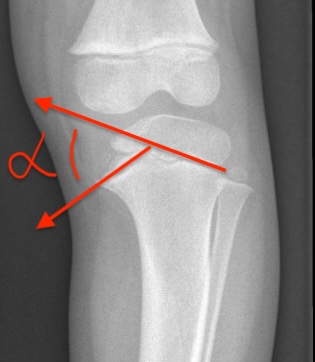
| Metaphyseal-Diaphyseal Angle | Medial physeal slope |
|---|---|
|
Line perpendicular to axis of tibia Line through medial and lateral metaphyseal beaks
|
Line through medial physis Line through lateral physis |
|
Physiologic bow legs < 11° Blount's > 11° Definitive Blount's > 16o |
High risk of progression if > 60° |
 |
 |
CT
Used to identify presence of physeal bar
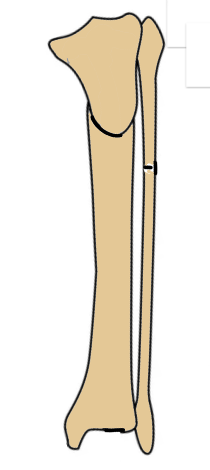
Langenskiold Classification
Six stages
- stages I - III: reversible with bracing
- stages IV - VI: permanent damage to eiphysis / need surgery
| Stage I | Stage II | Stage III |
|---|---|---|
| Medial beak | Medial saucer shaped defect | Develop step |
| Age 2 - 3 | Age 2 - 4 | Age 4 - 6 |



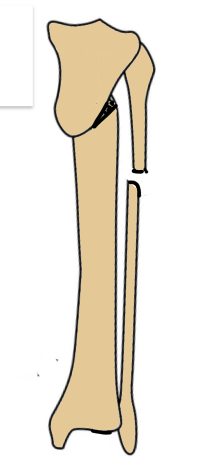
| Stage IV | Stage V | Stage VI |
|---|---|---|
|
Narrow physis Step deepens |
Medial epiphysis splits into two Physeal bar |
Medial growth arrest Develop severe varus |
| Age 5 - 10 | Age 9 - 11 | Age 10 - 13 |


Differential diagnosis

Rickets Achondroplasia
Physiological varus - normal growth plate, metaphyseal-diaphyseal angle < 11°
Ricket's / renal osteodystrophy - widened physes / cupped metaphyses / flared distal distal
Skeletal dysplasia - metaphyseal chondrodysplasia, achondroplasia
Trauma / tumour / infection
Osteogenesis imperfecta
Juvenile rheumatoid arthritis
Natural history
Progresses to severe osteoarthritis by early adulthood
Disease progression
- metaphyseal-diaphyseal angle >16° - 95% chance of progression
- metaphyseal-diaphyseal angle < 11° - 95% chance of spontaneous resolution
- metaphyseal-diaphyseal angle < 11 - 16° - close observation
Management
Brace / KAFO

Montenegro NB, Massa BSF, De Angeli LRA. Available from URL: http://www.scielo.br/aob.
Indications
< 3 with unilateral disease
Langeskiold stage I & II
Able to wear brace / obesity
Wear at night time
Results
Up to 50% failure
Poor compliance
Surgical options
Guided growth / temporary hemiepiphysiodesis
Osteotomy and acute correction
Osteotomy and gradual correction with frame
Medial tibial plateau elevation
Combined
Results
- systematic review of surgical treatment of 1600 knees with Blount's
- acute correction 47%, hemiepiphysiodesis 22%, gradual correction 18%, combined 13%
- overall recurrence 18%
- recurrence: gradual correction 7%, hemiepiphysiodesis 29%
- increasing recurrence rate with increasing age
Guided growth / temporary hemiepiphysiodesis

Indication
Lagenskiold stage I & II
Mild to moderate deformity
No physeal bar in medial growth plate
Technique


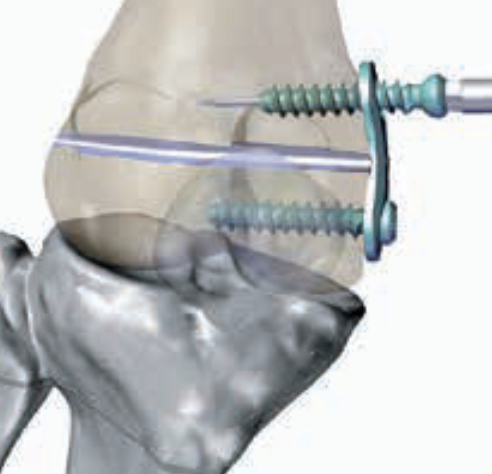

Eight plate surgical technique PDF
Arthroscopy techniques guided growth PDF
Results
Jain et al J Pediatr Orthop 2020
- 61 limbs with Blount's treated with tension band plates
- 41% overall surgical failure rate: more common with severe deformity
- 11% mechanical failure - more common with titanium and cannulated screws



Osteotomy with acute correction
Indication
Langenskiold Stage III - VI
Medial physeal bar
Moderate deformity
Types
Opening / closing wedge
Dome
Oblique osteotomy - Rab biplanar oblique osteotomy


Technique
Rab oblique osteotomy

Rab oblique osteotomy
Surgical technique oblique osteotomy PDF
Osteotomy performed distal to tibial tuberosity
- must osteotomise fibula
- must release anterior compartment to prevent compartment syndrome
- also correct deformity internal tibial torsion at same time
- fixation with K wires / screws / plates
- cast postoperatively
- +/- temporary hemiepiphysiodesis lateral
- +/- medial physeal bar resection
- +/- medial tibial plateau elevation
Results
Mare et al J Pediatr Orthop 2021
- 20 patients mean age of 4 treated with acute proximal dome osteotomy
- 40% recurrence at 4 year follow up
- increased risk with increased Langenskiold stage / severe deformity / increased medial physeal slope
Osteotomy with gradual correction using external fixation



Technique
Vumedi Taylor Spatial Frame for severe Blount's deformity video
Vumedi principles of frame correction for Blount's disease video
POSNA Taylor Spatial Frame Correction for severe Blount's video
Results
Mare et al Strategies Trauma Limb Recon 2022
- 25 severe or recurrent Blount's treated with hexapod external fixation
- alignment after correction: 55% good, 35% acceptable, 10% poor
- mean time in external fixator 136 days
- 100% incidence pin site infections
Lateral epiphysiodesis + medial metaphyseal elevation osteotomy

Indications
Langenskiold Stages V & VI
Medial physeal bar
Technique
Lateral epiphysiodesis
Fibular osteotomy
Lateral compartment release
Medial elevation osteotomy
+/- epiphysiodesis of contralateral knee to prevent leg length discrepancy
Results
Hussein et al J Orthop Surg Res 2025
- 24 patients with Langenskiold Stage V and VI
- medial plateau elevation and external fixator
- mean time in frame 14 weeks
- recurrence in 21%