



Anatomy
| Scapholunate ligament | Scapholunate joint |
|---|---|
|
C shaped
3 components - dorsal ligament: thickness and most important - membranous - volar ligament thickness
|
Scaphoid and lunate move together - flex with radial deviation - extend with ulna deviation |
Pathology
Most injured carpal ligament
FOOSH
- axial loading
- capitate driven into interval between scaphoid and lunate
| Dynamic instability | Static instability | SLAC |
|---|---|---|
|
SL ligament torn
Scaphoid and lunate not separated
|
DISI (dorsal intercalated instability)
Takes 3 - 12 months to develop |
Arthritic changes
Takes 3 - 15 years |
|
Ligament tears - scaphoid most comon - midsubstance - off lunate least common |
Scaphoid and lunate separate on xray
Scaphoid flexes due to attachment to distal row
Lunate extends due to triquetrum attachment |
Radial styloid
Radio-styloid joint
Midcarpal joint as capitate descends into SL gap |
Examination
Swelling and tenderness over scapho-lunate joint
Scapholunate ballottement
- stabilize scaphoid and lunate
- move them relative to each other
Kirk-Watson test
- thumb on dorsum wrist / index finger on scaphoid tuberosity
- passive ulna deviation: the scaphoid is displaced dorsally over the lip of the radius
- passive radial deviation: scaphoid proximal pole reduces with a clunk


X-ray



Scapholunate gap > 3 mm
AP
| Terry Thomas sign | Cortical ring sign | Scaphoid shortened |
|---|---|---|
|
Increased scapholunate interval > 3 mm compared with other side |
End on view of distal scaphoid due to flexion | Shortened due to flexion |
 |
 |
 |
Lateral xray
Increased scapholunate angle > 60o
- scaphoid flexed & lunate extended
- usually 30 - 60o


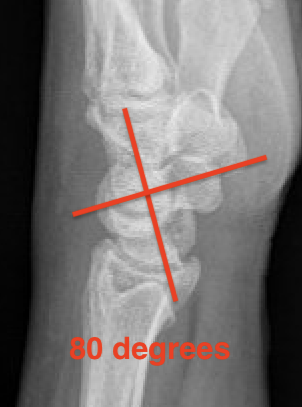
Scapholunate angle 80o
Stress views
Bilateral clenched wrists
- in ulnar deviation
- in radial deviation

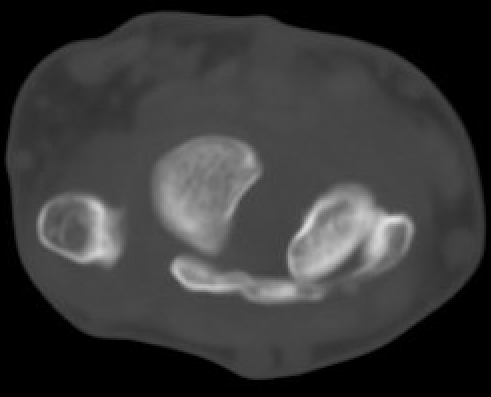
CT


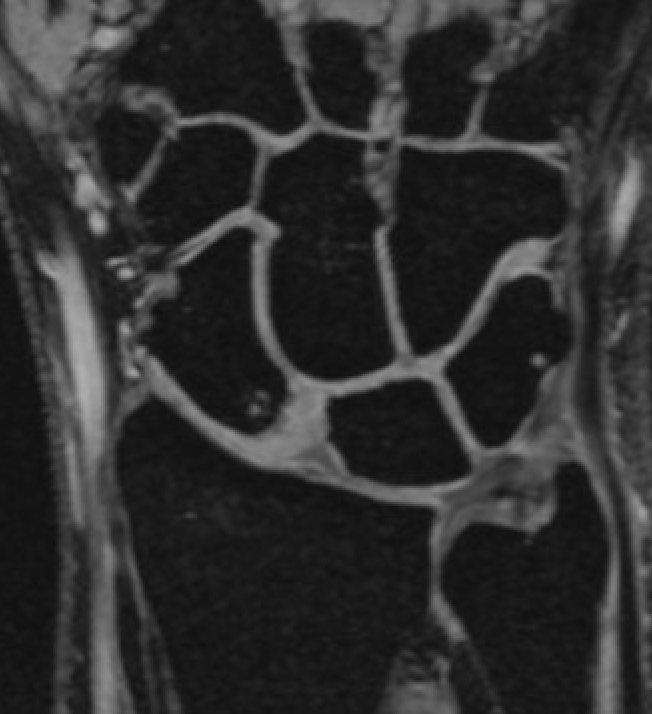
MRI

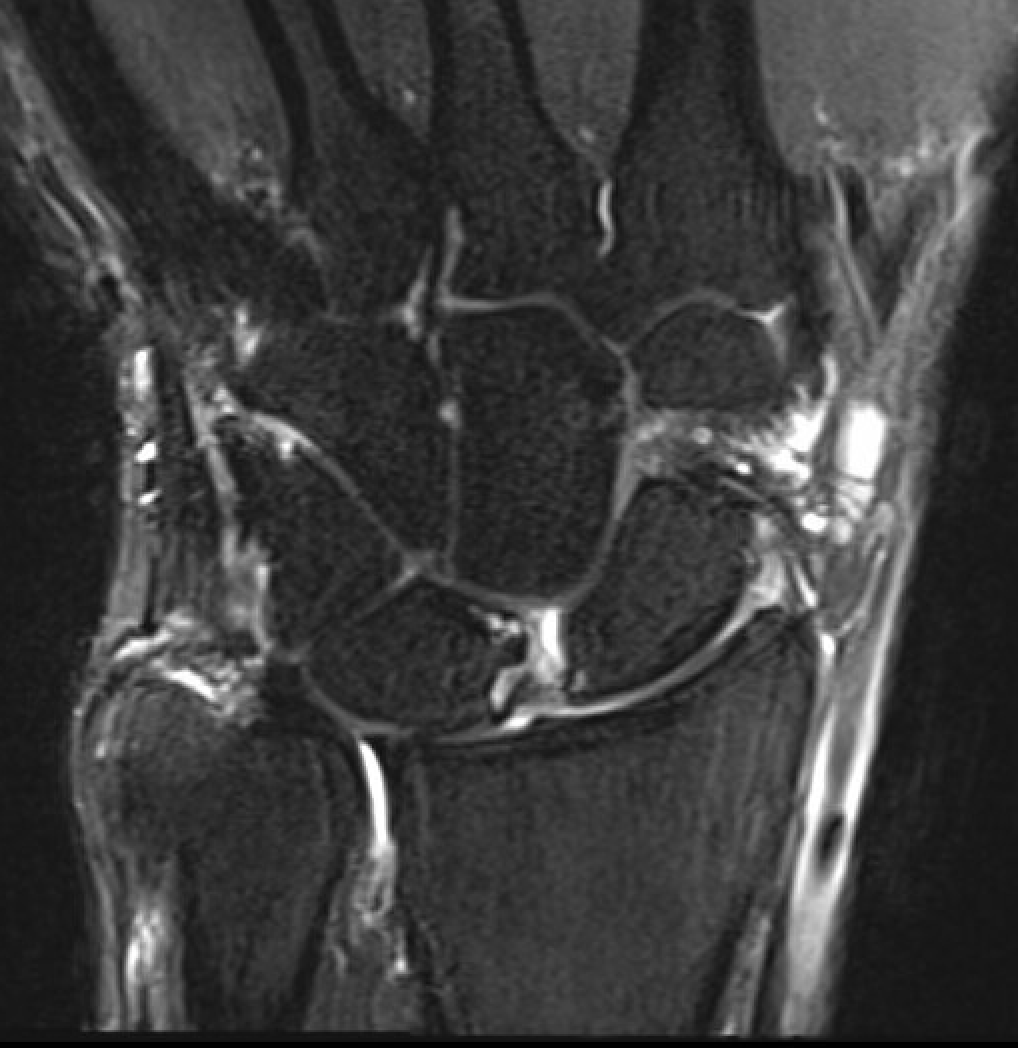
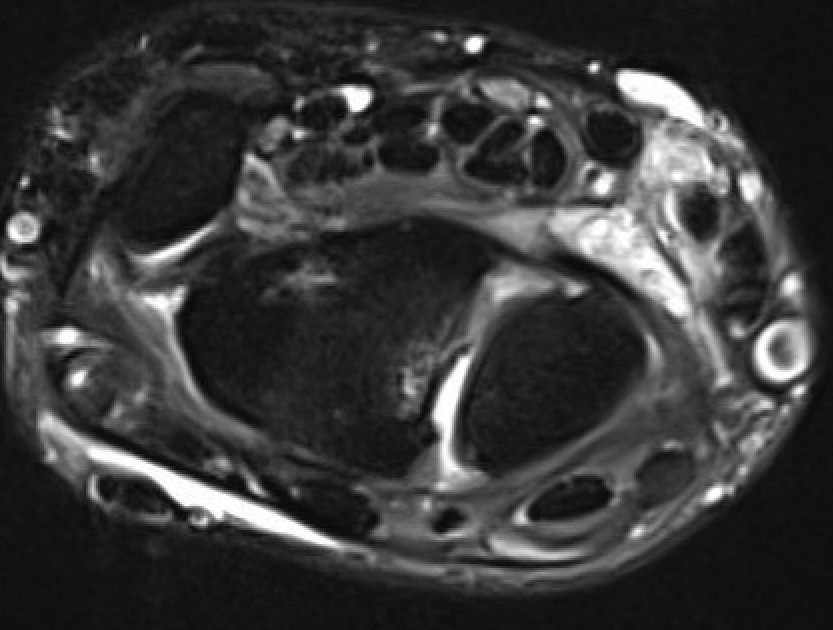
SL ligament injury with minimal disassociation / SL separation / dynamic instability
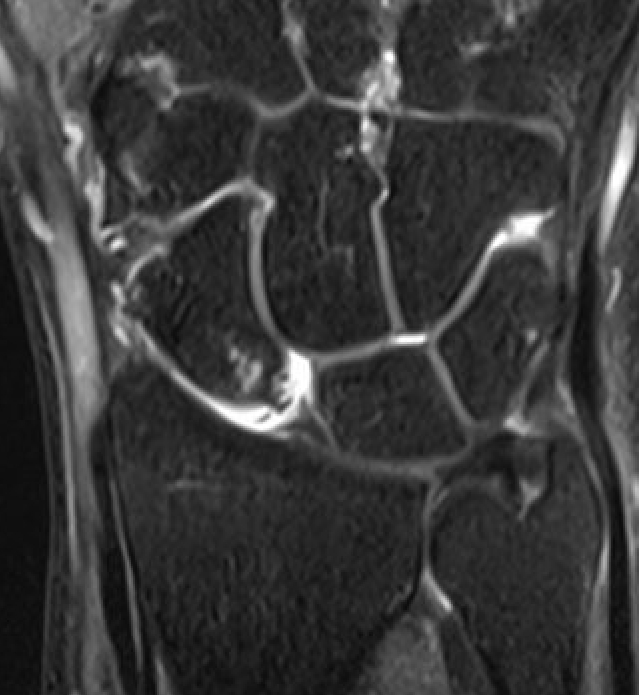
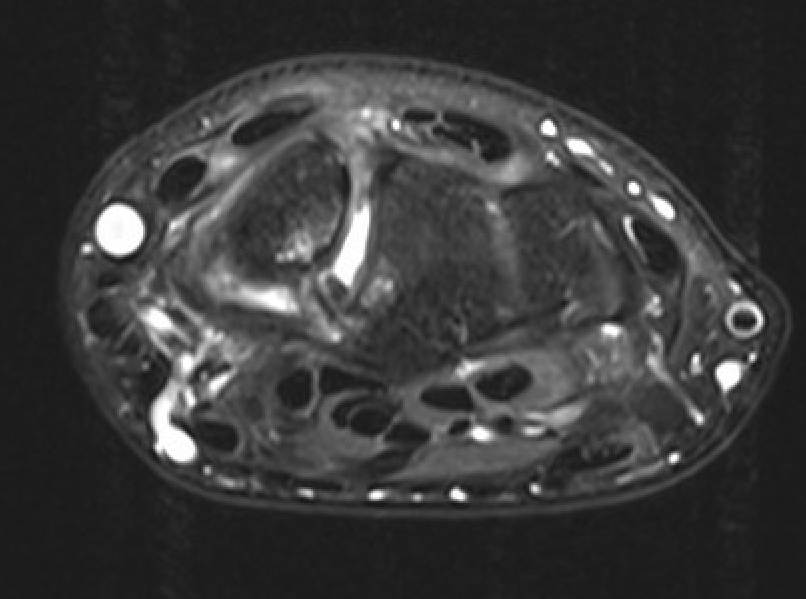
SL ligament injury with SL separation and static instability
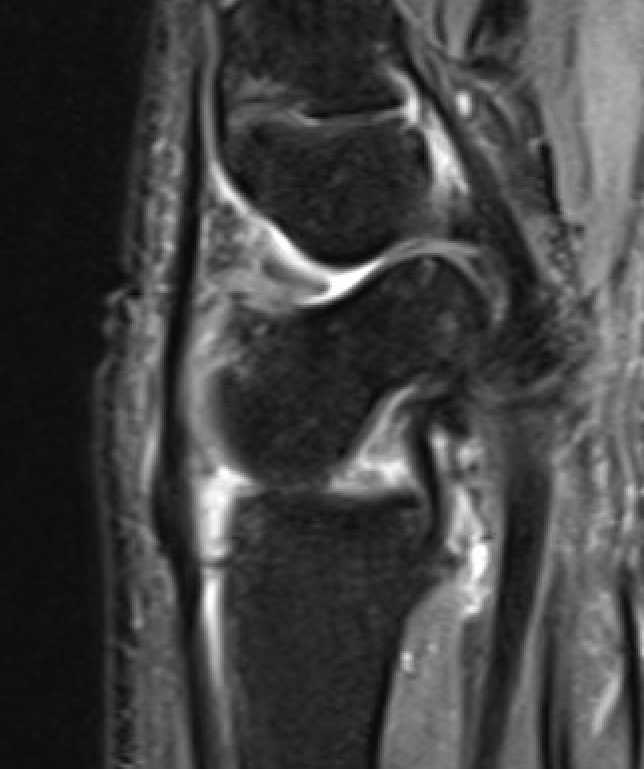
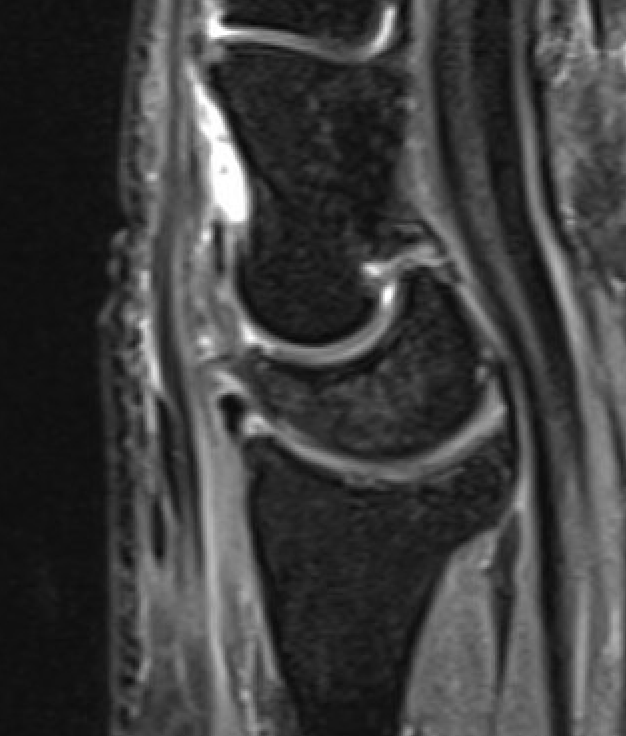
Increased scapholunate angle
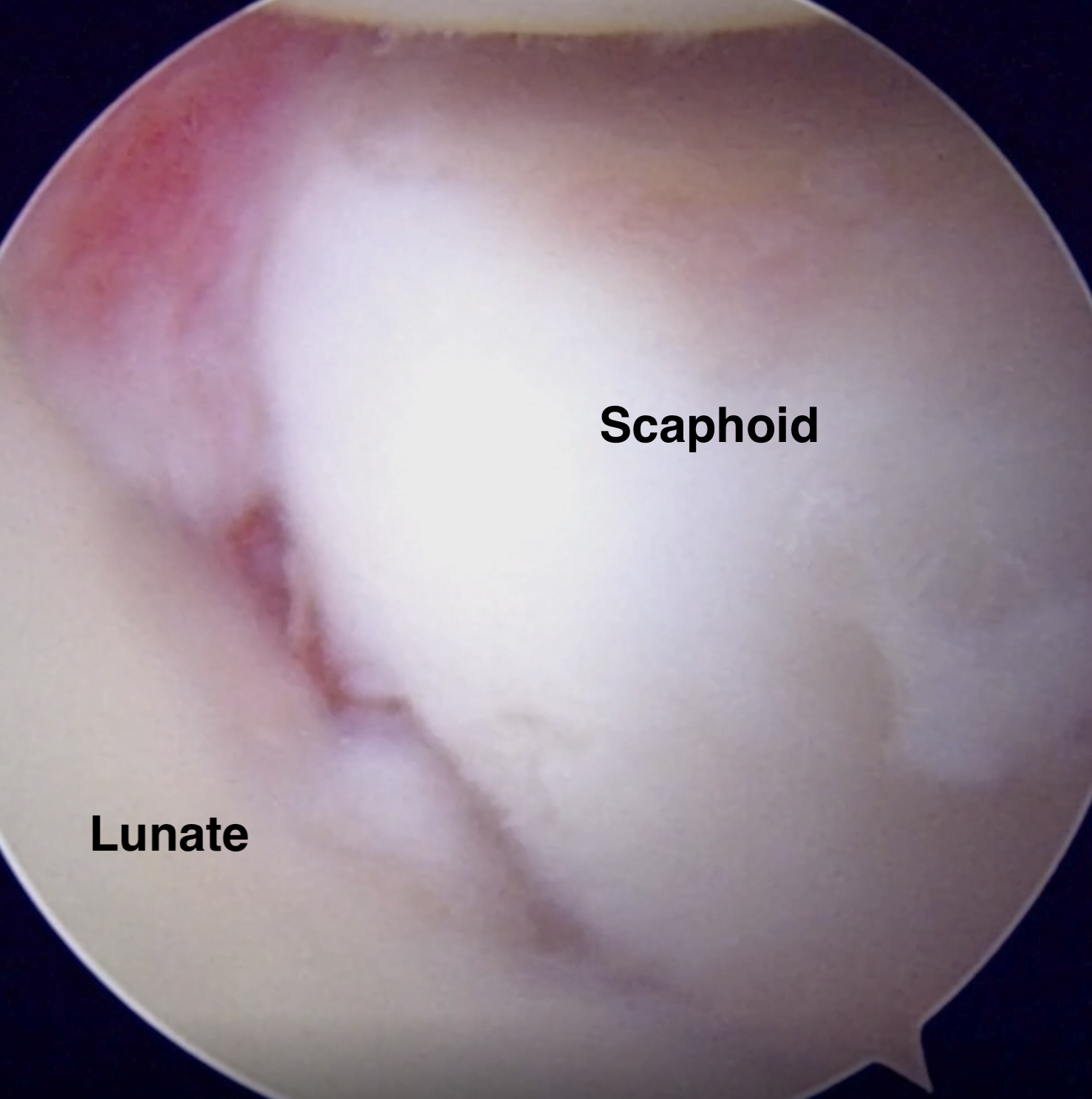
Arthroscopy

Normal scapholunate ligament radiocarpal arthroscopy
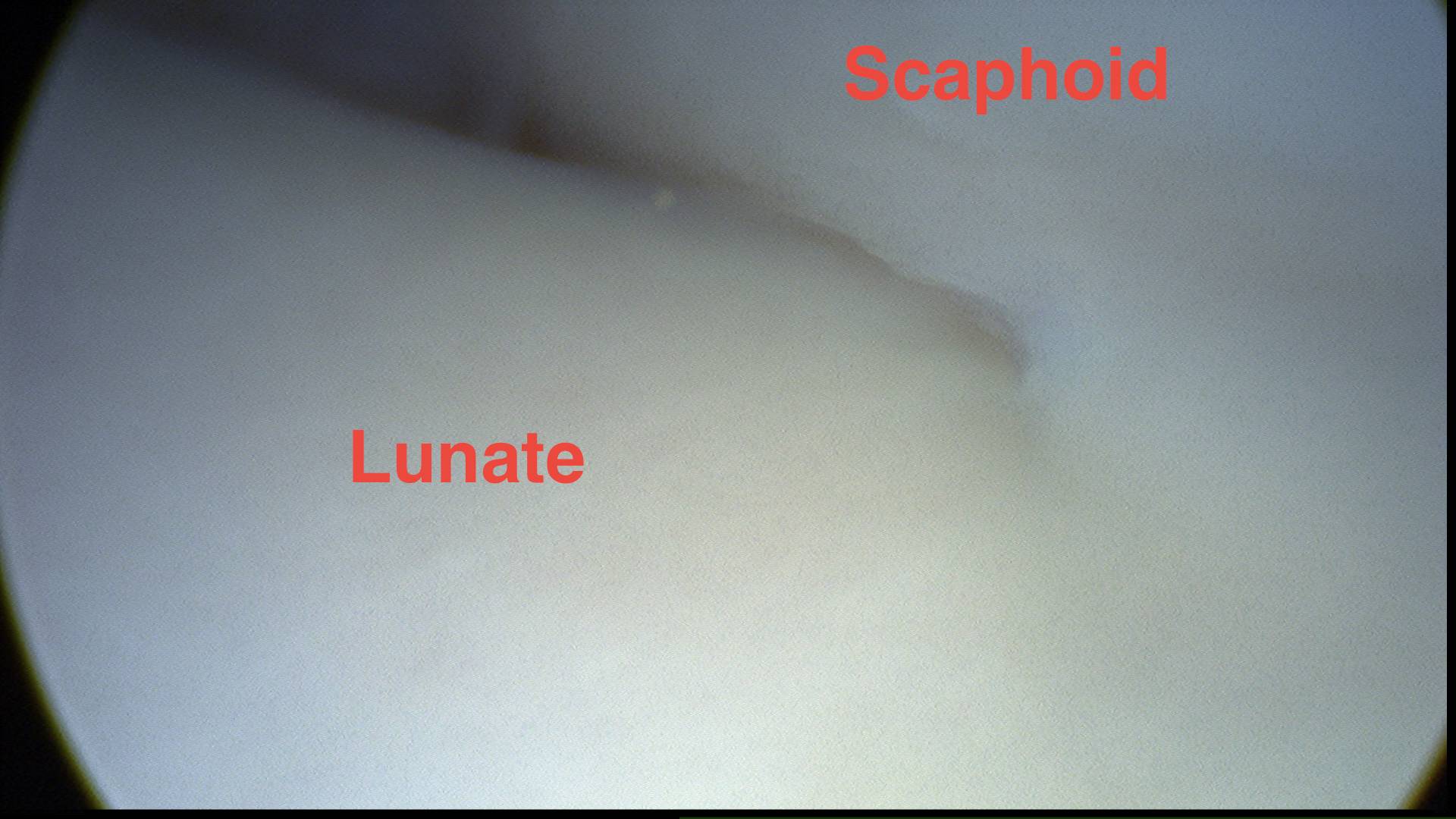
Normal scapholunate ligament midcarpal arthroscopy
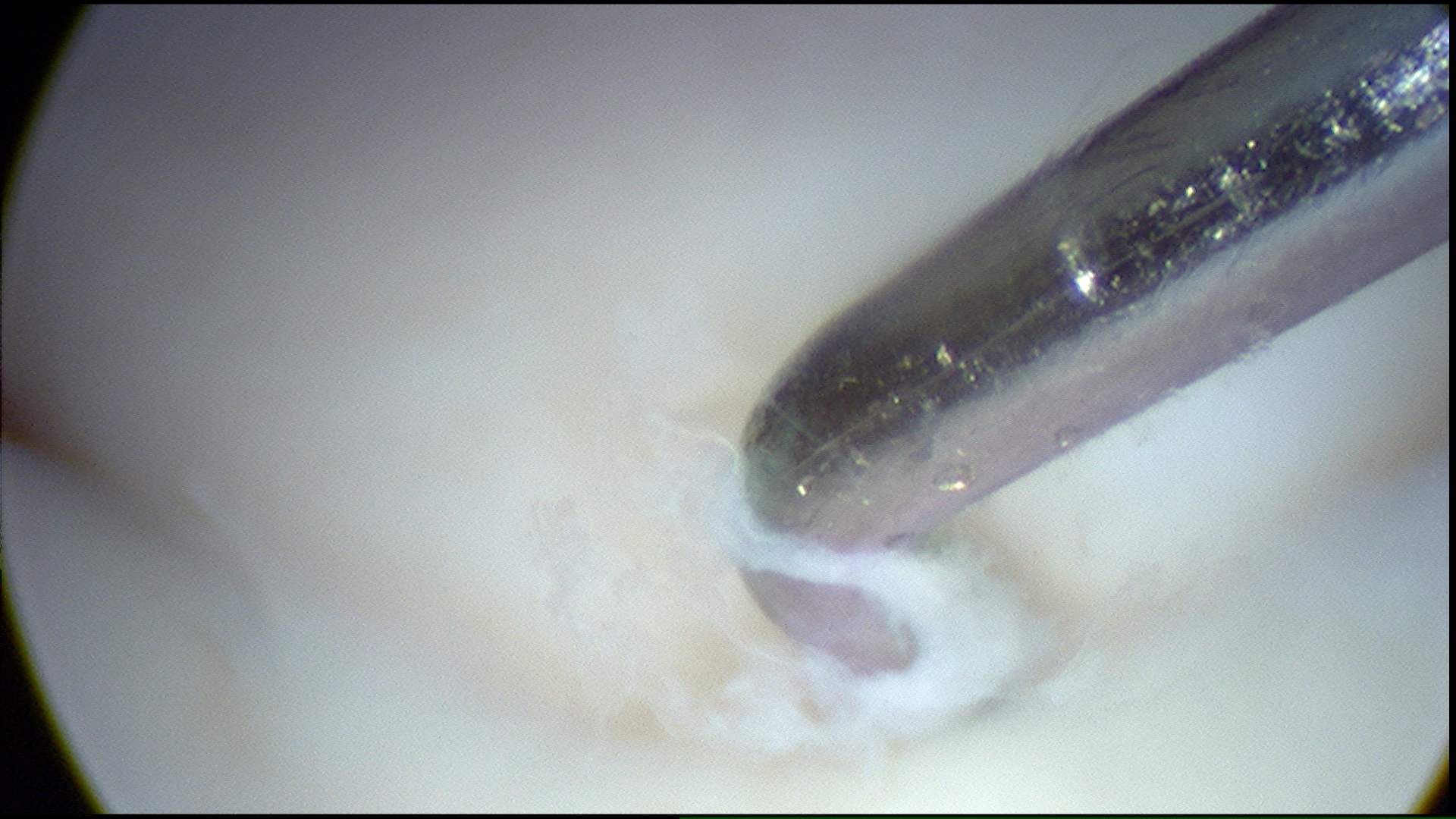
Torn scapholunate ligament midcarpal arthroscopy
Modified Geissler classification
Grade I: SL ligament attenuation/hemorrhage, no intercarpal incongruency
Grade II: SL ligament attenuation, intercarpal incongruency, 1 mm probe can be passed but not rotated through carpal gap
Grade III: SL ligament attenuation, intercarpal incongruency, 1 mm probe can be passed and rotated through carpal gap
Grade IV: Drive-through sign with 2.7 mm scope
Operative management
Options
Acute scapholunate ligament injury - repair +/- augment
Chronic scapholunate ligament injury / reducible carpus - capsulodesis / tenodesis / RASL / ligament reconstruction
Irreducible carpus / SLAC wrist
- proximal row carpectomy / limited arthrodesis / wrist arthrodesis
Acute scapholunate ligament injury
Options
Scapholigament repair +/- capsulodesis
Indications
Acute injury: 1 - 2 months
Amenable to repair: avulsion dorsal SL ligament from scaphoid or lunate
Open technique

Dorsal approach
- 3 / 4 interval (3rd and 4th extensor compartments)
- capsulotomy: T shaped or Berger radially based capsule flap
- place K wires into scaphoid and lunate and reduce scapholunate joint
- repair with anchors / drill holes
+/- K wires scaphoid - lunate & scapho-capitate joints
+ / - Augmentation - internal brace / capsulodesis / tenodesis / SL screw
Arthroscopic technique
Arthroscopic SL ligament repair and dorsal capsulodesis PDF
Results
Timing
Chen et al J Hand Surg Glob 2021
- 12 acute SL repair (< 6 weeks) v 12 subacute SL repair (< 12 weeks)
- SL repair with anchors + K wire scapholunate and scaphocapitate joint 6 - 8 weeks
- cast 6 - 8 weeks
- 60 - 75% also underwent capsulodesis
- no difference between 2 groups at 6 year follow up
- 1/12 (8%) acute developed SLAC
- 3/12 (25%) subacute developed SLAC
Arthroscopic repair
Lee et al J Orthop Surg Res 2023
- 19 acute SL injury treated with SL repair and dorsal capsulodesis
- at one year, 95% good or excellent results
- 84% return to previous activities
- failure of repair 5%
Chronic scapholunate ligament injury with reducible carpus and no SLAC
Indications
Chronic injury > 12 weeks
Non reconstructable injury / midsubstance
Reducible carpus - able to reduce scapholunate and scaphocapitate joint
No SLAC / arthritic changes
Options
|
Tenodesis / capsulodesis
|
Scapholunate ligament reconstruction / ligamentoplasty |
|---|---|
|
Capsulodesis - dorsal capsulodesis to distal scaphoid
Tenodesis - FCR tenodesis distal scaphoid to lunate / distal radius
|
RASL (Reduction and Association ScaphoLunate) - temporary screw fixation scapholunate joint
Scapholunate ligament reconstruction - with FCR / palmaris / bone-tissue-bone - +/- internal brace |
Results
Capsulodesis v tenodesis
- systematic review of chronic SL injury
- improved outcomes with capsulodesis v tenodesis
Capsulodesis / tenodesis v ligament reconstruction
- systematic review of capsulodesis v tenodesis v bone-tissue-bone reconstruction
- best outcome scores with bone-tissue bone
- highest rate of excellent outcomes with bone-tissue-bone 64%
Athlani et al Hand Surg Rehab 2019
- 20 chronic SL injuries treated with 3 ligament tenodesis versus ligament reconstruction
- 2 year followup
- better results with ligament reconstruction
Lami et al J Hand Surg Global 2025
- systematic review of capsulodesis v tendodesis v ligament repair v ligament reconstruction
- repair: SLAC 31%
- ligament reconstruction: SLAC 15%
- capsulodesis: SLAC 11%
- tendodesis: SLAC 14%
Capsulodesis
| Blatt capsulodesis | Modified Blatt capsulodesis | Modified Viegas / Berger |
Mathoulin capsulodesis |
|---|---|---|---|
|
Dorsal approach - proximally based capsular flap - reduce SL joint with K wires - K wire SL joint and SC joint
Attach capsule - distal pole of scaphoid - prevents flexion of scaphoid
|
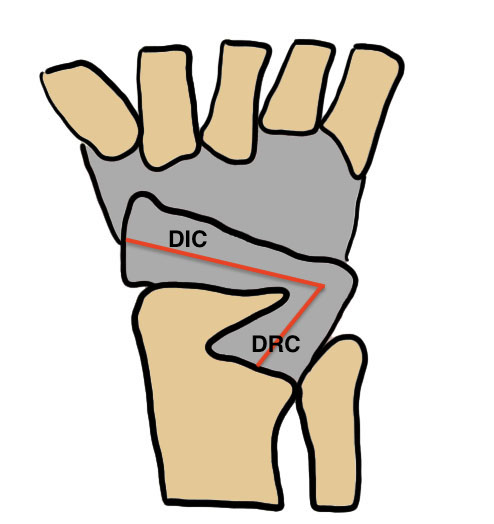
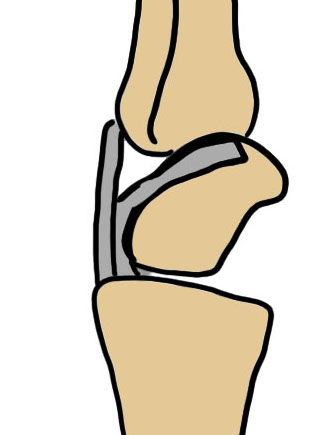
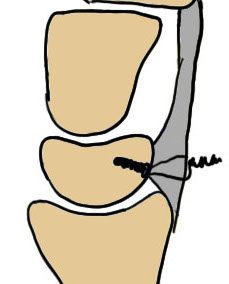
Dorsal approach - reduce and K wire SL joint - identify DIC ligament
Dettach DIC ligament from trapezium
Reattach to distal scaphoid |
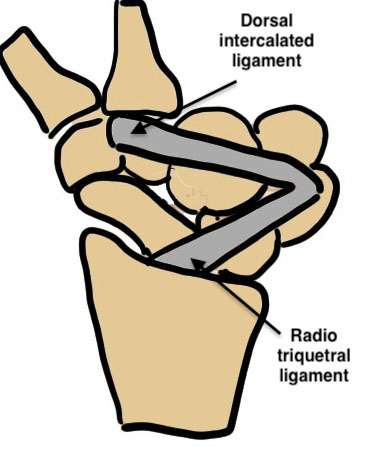
Dorsal approach - elevate radial based V shaped flap - between DIC and DRT ligaments - tie DIC / DRT ligaments to SL joint |
Arthroscopic technique - reduce SL joint - tie down dorsal capsule onto SL joint |
| Vumedi modified Blatt procedure | |||
 |
|
 |
 |

Techniques
Vumedi modified Blatt procedure
Results
Terras et al Acta Orthop Belg 2025
- systematic review of dorsal capsulodesis for chronic SL injury
- reduced stiffness with modified Viegas / Berger versus Blatt
- best results with all-arthroscopic Mathoulin
Tenodesis
Brunelli - replaces scaphotrapezial ligament, attaches to distal radius
Modified Brunelli - passes under / through radiotriquetral liagment, suture to itself
Three-ligament tenodesis - replaces scapotrapezial / scapholunate / radiotriquetral
| Brunelli Wrist Tenodesis | Modified Brunelli | Garcia-Elias Three-ligament tenodesis |
|---|---|---|
|
Dorsal approach - T capsulotomy or Berger - reduce SL joint with K wires - K wire SL joint and SC joint
Second volar approach - harvest half FCR, 8 cm long - leave attached distally
Drill hole in scaphoid tuberosity - pass volar to dorsal - insert dorsally to the distal radius |
Dorsal approach - T capsulotomy or Berger - reduce SL joint with K wires - K wire SL joint and SC joint
Second volar approach - harvest half FCR, 8 cm long - leave attached distally Drill hole in scaphoid tuberosity - aim to exit close to SL joint - pass volar to dorsal
Pass under radiotriquetral liagment Suture to carpus / itself |
Dorsal approach - T capsulotomy or Berger - reduce SL joint and K wire - K wire SL joint and SC joint
Second volar approach - harvest half FCR, 8 cm long - leave attached distally
Drill hole in scaphoid tuberosity - aim to exit close to SL joint - pass volar to dorsal
Anchor to lunate
Pass through radiotriquetral ligament
Suture to carpus / itself
|
 |
 |
 |
Techniques
Vumedi modified Brunelli video
Vumedi Three-ligament tenodesis video
Results
Goeminne et al J Wrist Surg 2024
- systematic review of modified Brunelli v three-ligament reconstruction
- 600 patients
- return to work 65%: modified Brunelli 45%, 3LT 70%
- better ROM with 3LT
- SLAC 15%
- 3 cases of scaphoid necrosis
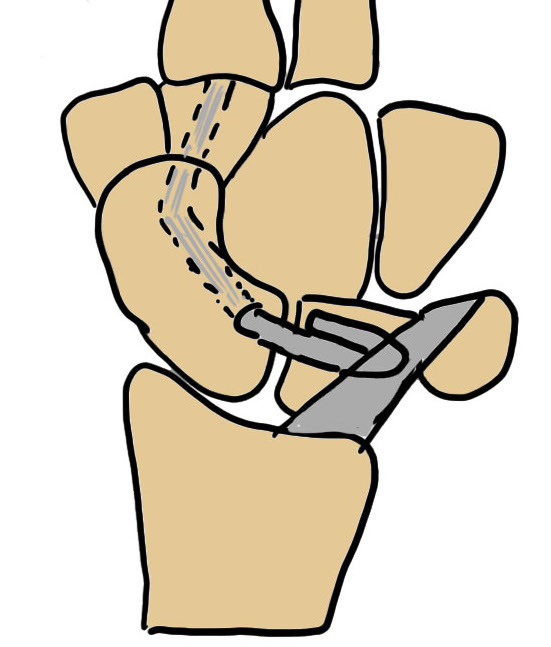
RASL (Reduction and Association ScaphoLunate)


Technique
Reduce SL joint with K wires
- secondary radial incision
- headless compression SL screw
- ? remove at 3 months
- creates mobile synchondrosis
Results
Aibinder et al J Wrist Surg 2018
- 12 patients with chronic SL injury treated with RASL
- 7 year follow up
- 7/12 developed degenerative changes
- 8/12 developed screw lucency requiring removal
Scapholunate ligament reconstruction / ligamentoplasty
Options
- autograft / allograft ligaments
- internal brace
- bone-retinaculum bone autografts




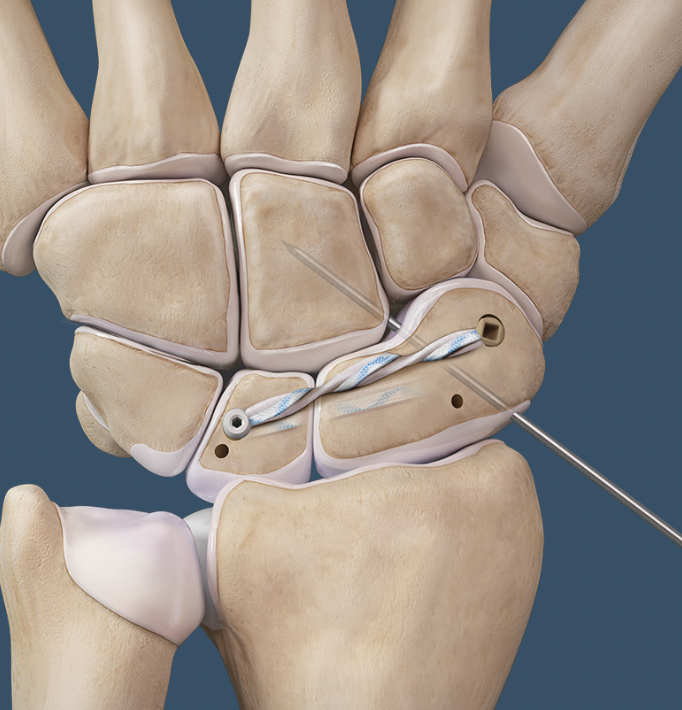
Open dorsal scapholunate ligament reconstruction
Arthrex all dorsal SL ligament reconstruction with internal brace PDF
Arthrex all dorsal SL ligament reconstruction with internal brace video
Vumedi dorsal SL ligament reconstruction with internal brace video
Arthroscopy techniques dorsal SL ligament reconstruction with internal brace
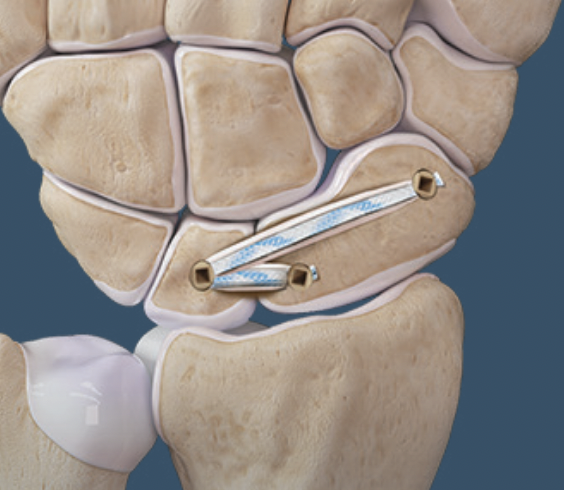
Interosseous scapholunate ligament reconstruction
Arthrex interosseous SL ligament reconstruction with internal brace PDF
Arthrex interosseous SL ligament reconstruction with internal brace video
Arthroscopic scapholunate ligament reconstruction
Arthroscopy techniques arthroscopic scapholunate ligament reconstruction PDF
Complications
Surgical failure

