

Indications
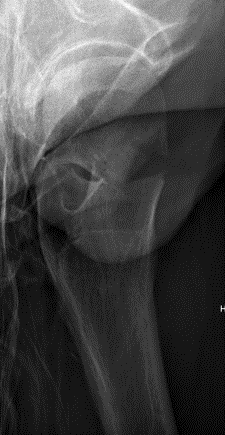
Displaced fracture - risk of AVN and nonunion
Patient too young for THA
Issues


Vumedi approach to young displaced femoral neck fracture
Timing of surgery
Closed versus open reduction
Capsulotomy
Open approach - Smith-Petersen versus Watson Jones
Fixation - screws / DHS / FNS +/- medial buttress plate
Timing of surgery
Papakostidis et al Injury 2015
- systematic review of 7 studies
- no association between timing of surgery and AVN
- increased incidence of nonunion with surgery > 24 hours
- retrospective review of displaced fractures in 29 patients < 60
- significant reduction in AVN if fixed within 12 hours
Closed versus open reduction
Union rates increased with anatomical reduction
- RCT of 92 patients with displaced subcapital fractures < 50 years
- randomized to open versus closed reduction
- no difference in union rates between groups
- increased nonunion with non anatomical reduction
Haidukewych et al JBJS Am 2004
- 51 displaced subcapital fractures < 50
- 10% incidence of nonunion
- 27% osteonecrosis
- nonunion 4% with good to excellent reduction
- nonunion 80% with poor reduction (>10 mm of displacement, >20°, any varus)
Assessment of reduction
1. Femoral neck shaft angle
2. Restoration of Shenton's line
Closed reduction / Leadbetter Maneuver
FATI CAR
- Flexion / Adduction / Traction / IR
- Circumduction / Abduction
- Reduction check in extension
- "Foot in Palm Test"
- if sufficiently reduced will sit without ER
Capsulotomy
Theory
- there is evidence of increased hip intracapsular pressure after fracture
- this may reduce blood flow to the femoral head
No conclusive evidence that capsulotomy reduces rates of AVN
Options with closed reduction
- percutaneous needle / knife drainage of hematoma
Approaches
Smith Petersen
- direct visualization of fracture
- likely better to allow anatomical reduction
- easier to do medial plating to hold reduction prior to definitive fixation
- need separate approach for fixation
Watson Jones
- less direct visualization of fracture
- same approach for fixation
Technique Smith Petersen Approach
Vumedi technique Smith Petersen
AO surgery foundation Smith Peterson PDF
Radiolucent table + floppy lateral with sandbag under affected hip
Vertical incision below ASIS
Superficial dissection
- between TFL (lateral) and sartorius (medial)
- interval more clear distally
- divide fasica over TFL with LFCN medial
- reflect muscle of TFL laterally
Deep dissection
- between G medius laterally and direct head rectus femoris medially
- +/- tenotomy of direct head rectus femoris


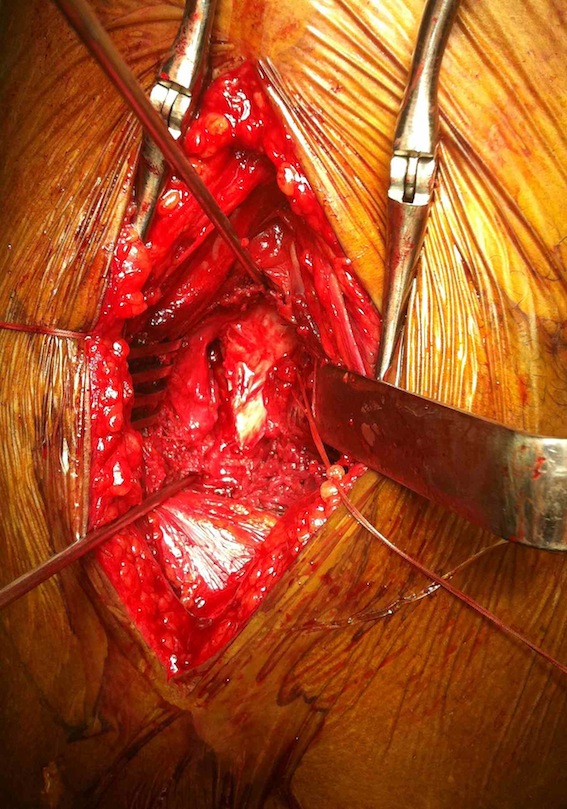
Smith Petersen anterior approach, with capsulotomy and reduction with pins
Technique Watson Jones approach
Vumedi surgical Watson Jones technique
AO surgery foundation Watson Jones PDF
Radiolucent table + floppy lateral with sandbag under affected hip
Lateral incision between anterior aspect greater trochanter and ASIS
Flexing hip 20-30o helps exposure
Superficial dissection
- identify interval between gluteus medius and tensor fascia lata (TFL)
- divide fascia lata
- identify fat pad inferiorly, muscle gluteus medius superiorly
- develop this interval to anterior femoral neck
- lateral femoral circumflex artery in this interval
- place retractors over inferior femoral neck and superior femoral neck
Deep dissection
- remove fat pad
- release reflected head of rectus femoris off anterior capsule
Capsulotomy
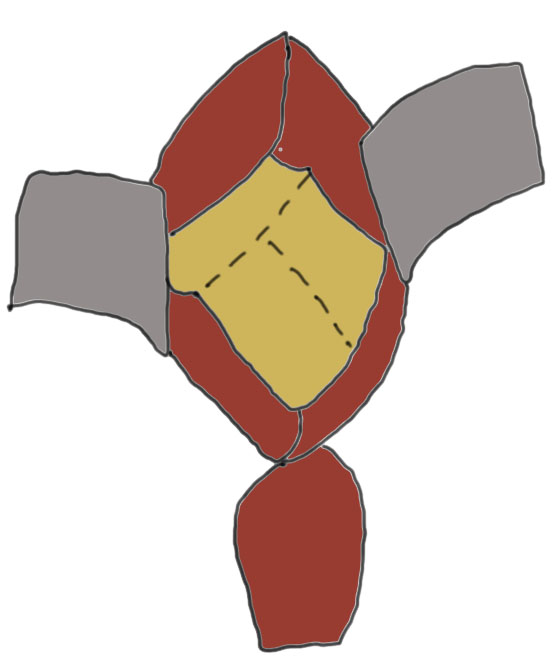
Capsulotomy
- transverse limb at head neck junction to preserve blood supply
- vertical down centre of femoral head
- avoid dissecting superior aspect of femoral neck where major artery of MCFA runs
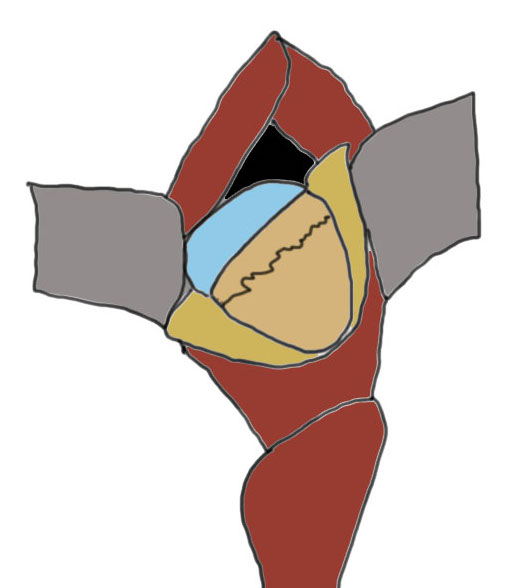
- tag and reflect capsule
- place retractors inside the capsulotomy to expose the femoral neck
- can place superior retractor on ilium
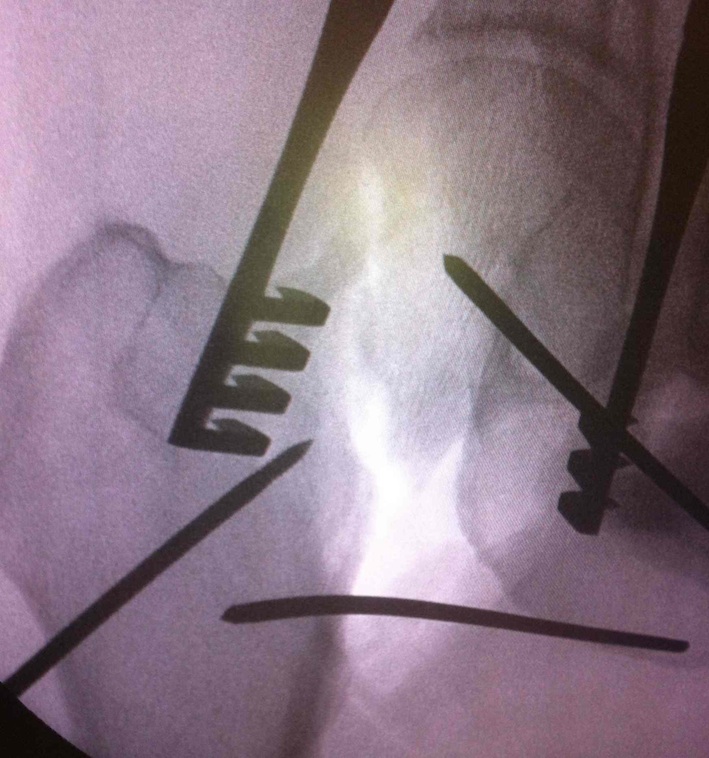
Reduction techniques
Obtain anatomical reduction under direct vision
- Steinman pin in femoral head
- second Steinman pin in femur to correct external rotation force
Check reduction on image intensifier
- ensure no varus on AP
- obtain lateral by adducting and IR hip / ensure good reduction on lateral
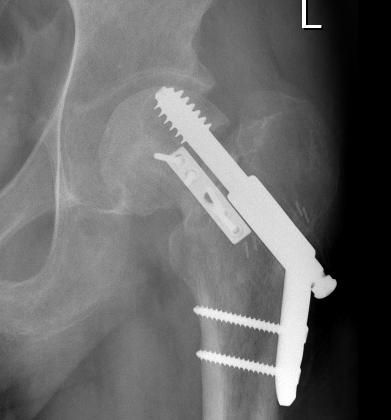
Fixation
DHS /Cannulated screws / FNS
Unstable fracture - augment with a medial buttress plate on inferior neck

Medial buttress plate
Non-Union

Options
Valgus osteotomy
THA
Valgus osteotomy
Aim
- convert shear forces into compressive forces across fracture
Indications
- patient must have at least 15o adduction
Template
- aim to reduce the angle of the neck fracture to between 20 - 30o from horizontal
- measure angle of fracture from horizontal (usually 40 - 50o up to 70o)
- difference is angle of correction (20 - 30o)
Technique
Vumedi valgus osteotomy femoral neck fracture nonunion
Results
Norouzi et al Eur J Trauma Emerg Surg 2009
- 33 cases of nonunion of femoral neck fracture
- combination failure post surgery and missed / neglected fractures
- union in 32/33 after 5 months with valgus osteotomy