
Technique
Vumedi surgical techique video
Position
- supine on radiolucent table
Incision with knee at 90°
- midpoint tibial tuberosity & fibular head
- extend proximally
- incise deep fascia / ITB in line with incision
- reflect underlying Tibialis anterior & EDL to expose tibia
- expose proximal tibia anteriorly and posteriorly
- homan retractor anteriorly under patella tendon
- dissect soft tissue subperiosteally off posterior tibial cortex
- retractor to protect posterior structures
Release Tibio-fibular joint
- protect the CPN by staying superior to neck
- insert osteotome into joint +/- remove sliver of head medial fibular head
Osteotomy
- guide wires at superior level osteotomy
- 2cm distal to joint in AP and lateral
- parallel to joint in AP and lateral plane
- inferior guide pins at level of desired wedge
- attempt to leave medial cortex intact
- try to remove wedge of bone intact
- medial aspect of wedge difficult to remove
Check correction
- drop rod
- Fujisawa point
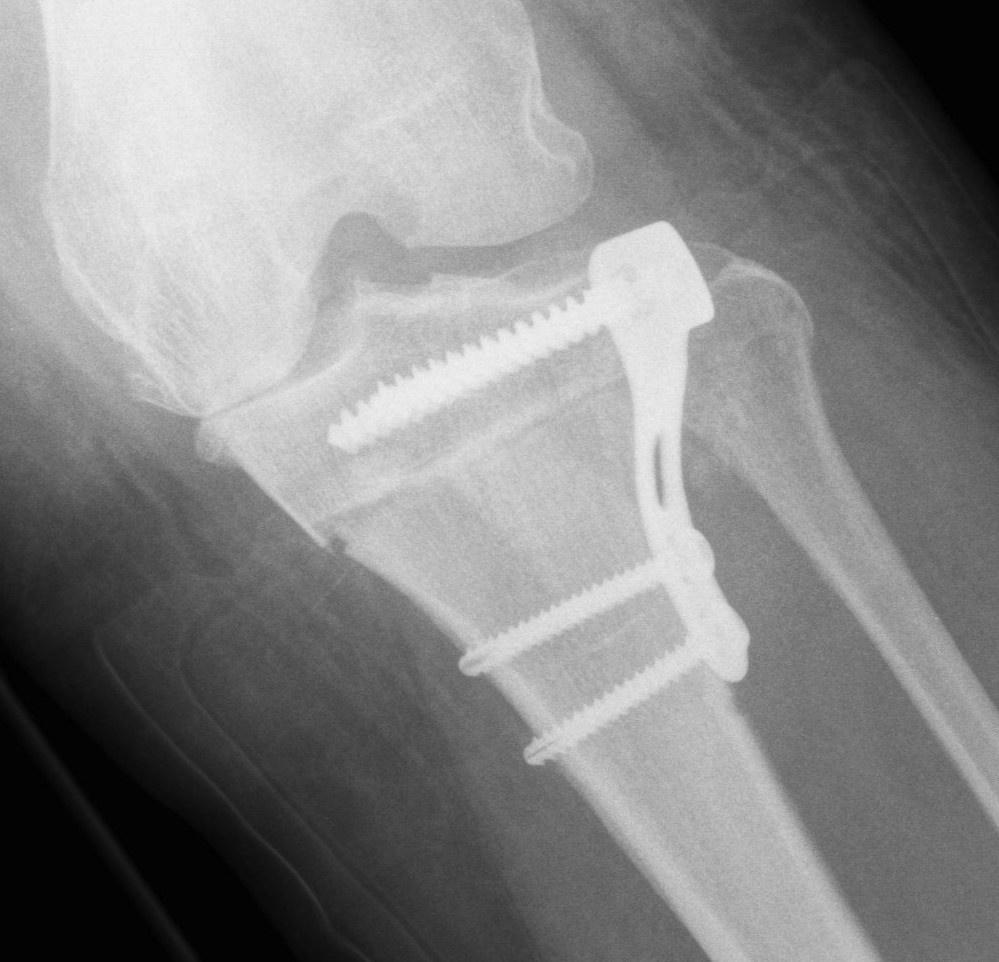
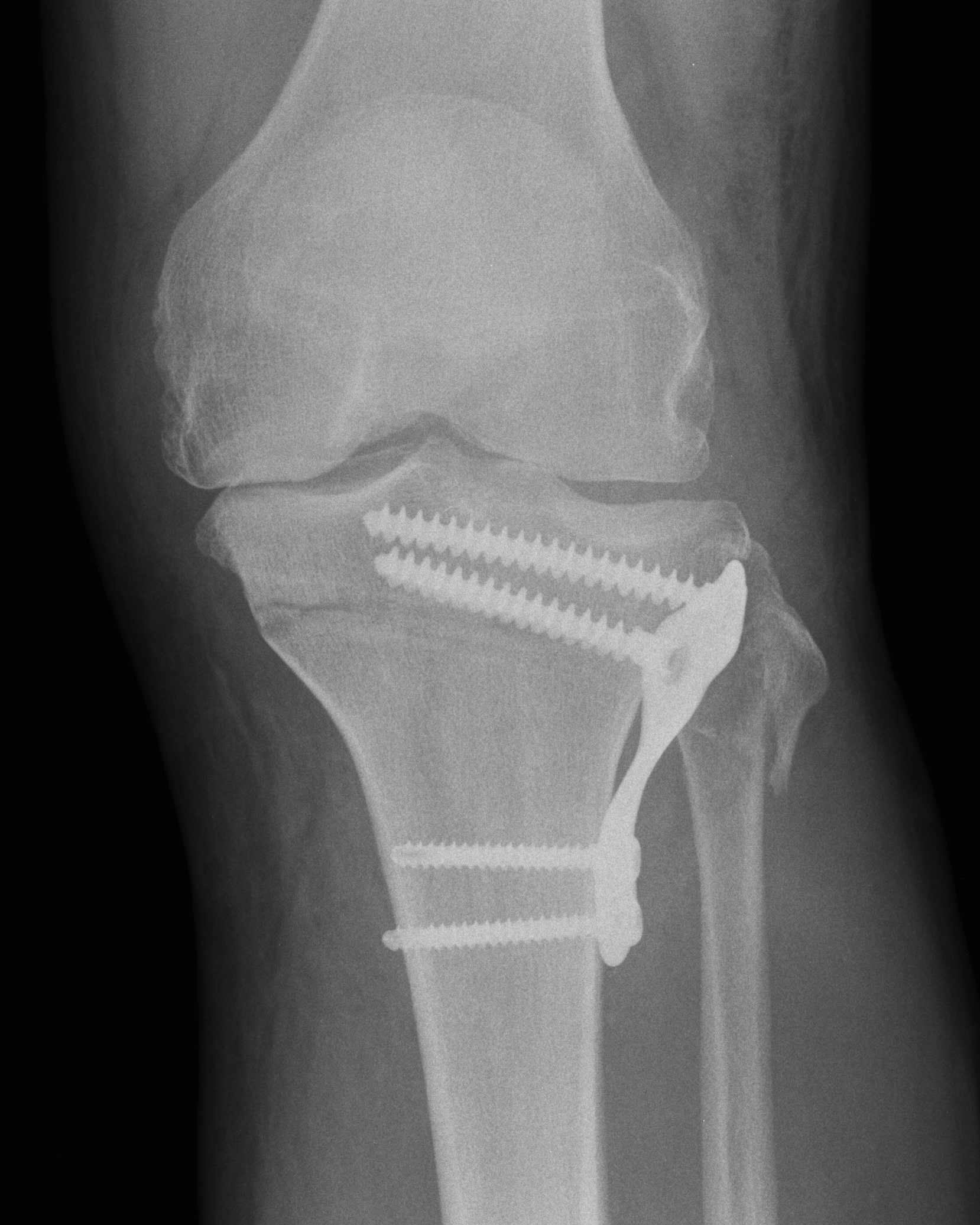
Stabilise osteotomy with plate
Complications
Medial hinge fracture

van Raaij et al Acta Orthop 2008
- 44 closing wedge HTO
- 36/44 (82%) had fracture
- no significant malunion
Undercorrection


CPN injury / compartment syndrome / foot drop / EHL weakness
Mechanism
- direct injury to CPN during proximal tibio-fibular joint release
- injury to nerve branches to EHL
- compartment syndrome from elevated anterolateral compartment pressures