Incidence
Up to 8% patients with ACL reconstruction will have recurrent instability and graft failure
- increased with surgical inexperience
Graft can
1. Be inadequate from the start
- inadequate tension
- poor tunnel placement
2. Stretch
- poor tunnel placement
- impingement
- non isometric
3. Rupture
- may be trauma
- may be surgical issues
Causes Rupture
A. Technical Failure
Non anatomic tunnel placement
Inadequate notchplasty
Improper tensioning
Graft impingement
Failure graft fixation
Insufficient graft material
B. Biological Failure
Failed ligamentisation
Infection
C. Failures due to trauma
Early (before graft incorporation)
Late (after incorporation)
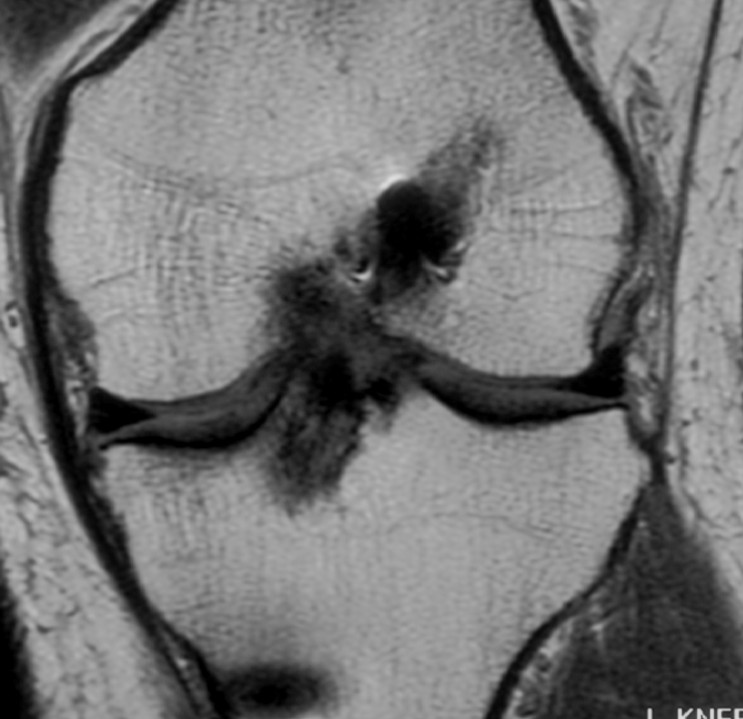
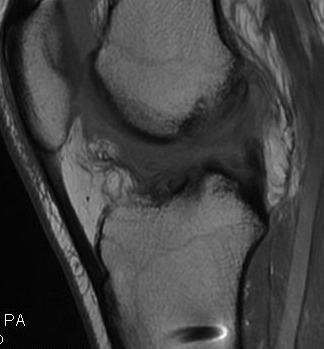
Graft rupture best seen on T1

D. Failures due to laxity of secondary restraints
Rotatory instability / Varus / Valgus instability
- posterolateral corner / PCL
Skeletal malalignment
Technical Issues
A. Non anatomic Tunnel Placement
Most common
- 70 - 80% Technical Failures
Mal-positioned grafts incur excessive tension
- impinge and become lax
Femoral Tunnel
Most common error in ACL Reconstruction
- errors in femoral placement are less forgiving
- either get a loss of motion or graft failure
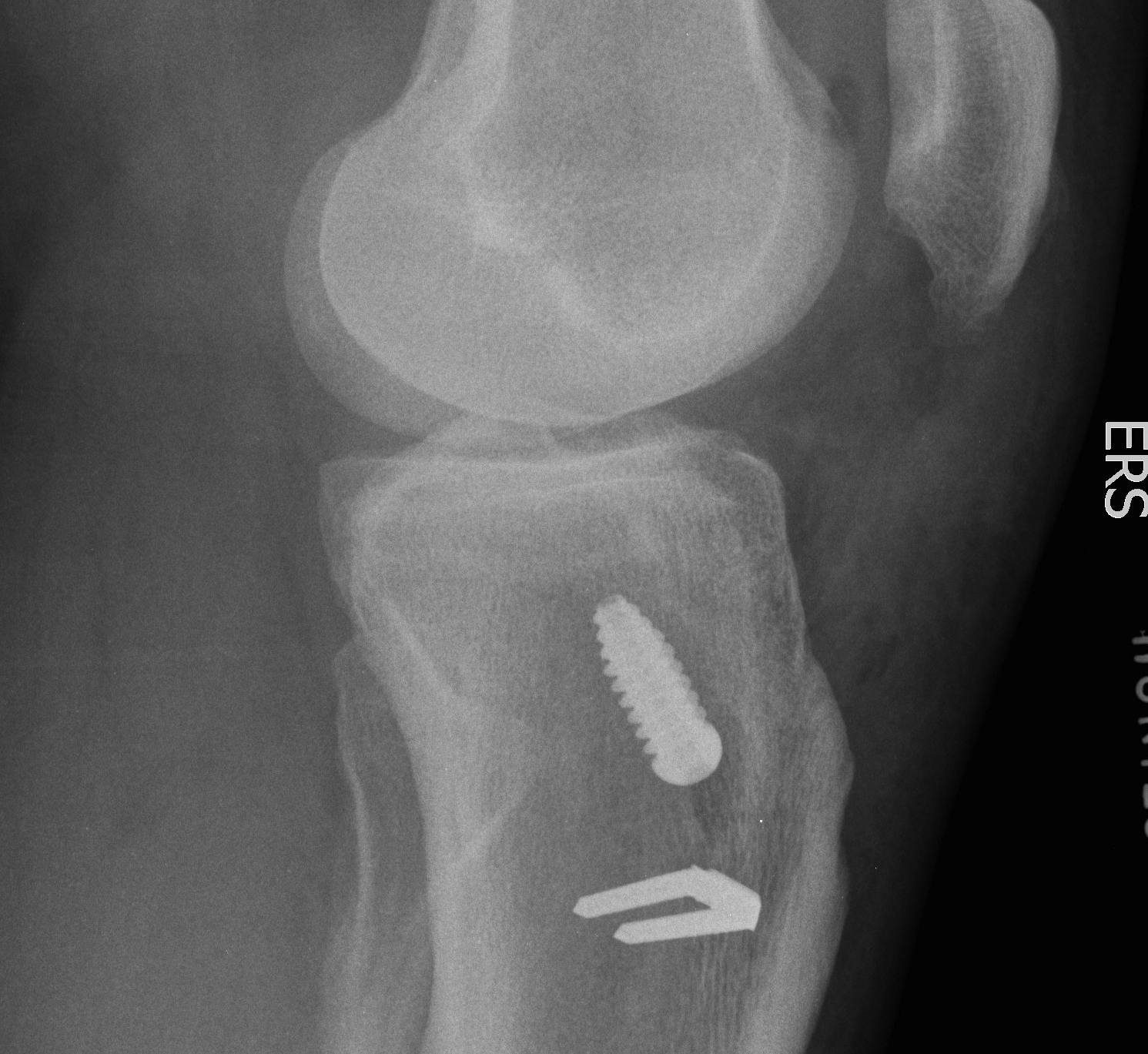
Optimal placement
- lateral radiograph
- intersection of Blumensaat's line and
- line extended from the posterior femoral cortex


A. Anterior femoral placement
- increases tension in flexion / loss of flexion
- stretching of the graft required to obtain flexion
B. Posterior femoral placement
- increases tension in extension
- need to stretch to obtain extension
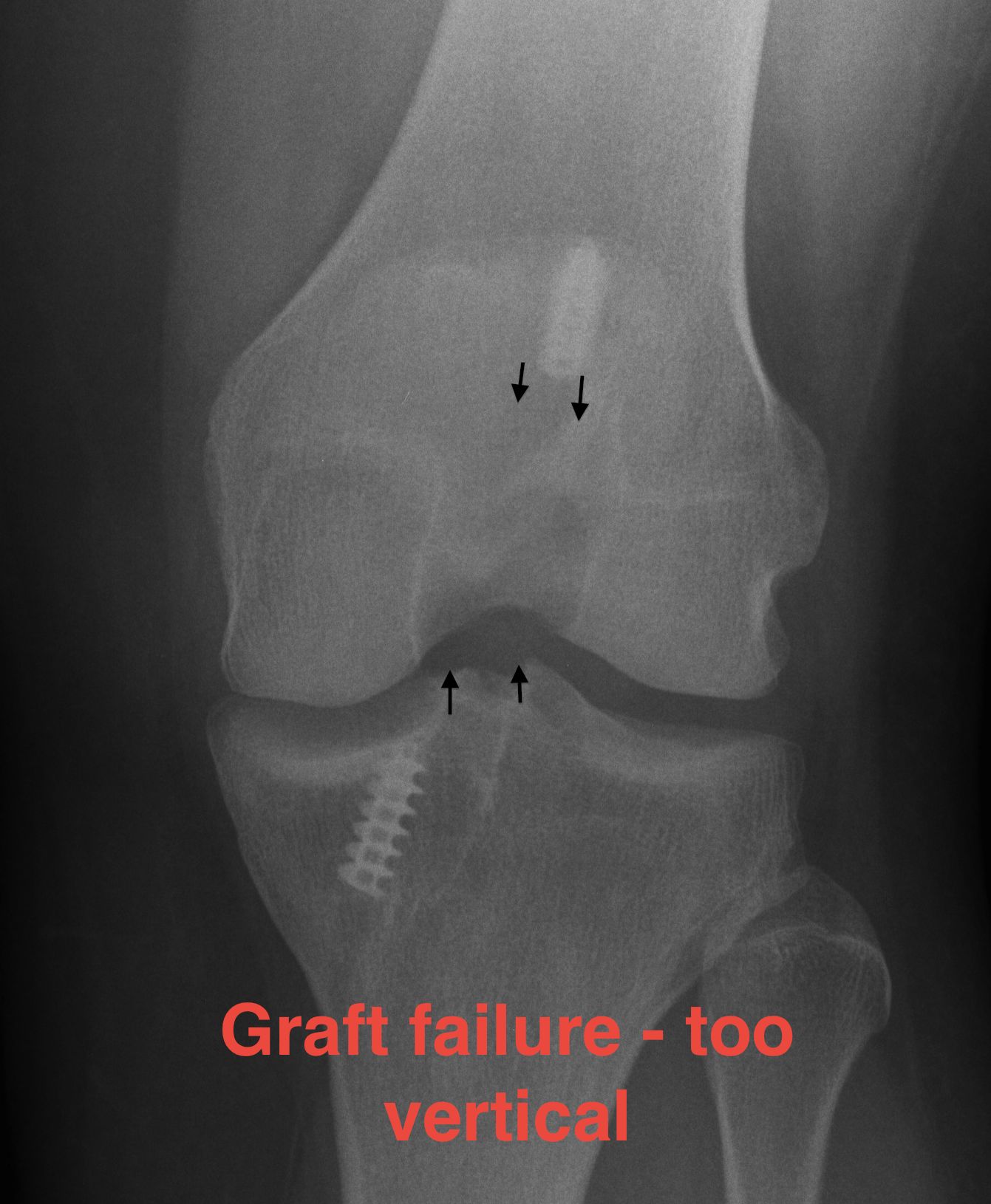
C. Superior femoral placement
- 12 o'clock position
- AP stability
- rotationally unstable / continue to pivot shift


Tibial Tunnel
More forgiving
Ideal Tibial tunnel placement
- posterior and parallel to the tibial intersection of Blumensaat's line in full extension
- this will prevent it impinging on the notch
A. Anterior placement
- increases tension in flexion
- may result in notch impingement in extension
- stretching of graft
B. Posterior placement
- causes PCL impingement
- reduces the graft's ability to control AP translation

C. Lateral placement
- causes impingement on the medial wall of the lateral femoral condyle
B. Inadequate notchplasty
Graft is often larger than native ACL
- especially with BPTB
- need to assess
- debride anterior lateral part of notch and roof
Impingement
- loss of extension
- formation Cyclops lesion
C. Improper Tensioning
Under tensioning
- non-functioning graft
Over tensioning
- constrain the knee
- affect graft incorporation
The ideal tension is unknown
- tension BPTB graft to 5-10 lb at 10-15 degrees flexion
- tension hamstring graft to 10-15 lb at 20-30 degrees of flexion
- cyclically preload & maintain tension until secured
D. Graft Fixation Failure
Takes 6-12 weeks for graft incorporation to occur with hamstrings
Graft fixation needs to be strong for this period
E. Tunnel Lysis

Very common, cause unknown
No evidence that contributes to instability
Important in revision setting
Cause
- more common tibial side than femur
- tends to stop after 3/12
- postulated to be from synovial fluid pistoning
- hence fluid finds it easier to come down tibial tunnel as screw placed outside in
- also seen more on femoral side with endobutton (windscreen wiper effect)