Issues
Immediate ACL reconstruction
Early v delayed ACL reconstruction
Repair v Reconstruction
Graft choices
Allograft
Synthetic
Single versus double bundle
Anterolateral ligament (ALL) reconstruction / Extra-articular tenodesis
Trans-tibial v anteromedial drilling
Position of knee during tibial fixation
Tunnel placement
Immediate ACL Reconstruction
Issue
Does early ACL reconstruction in the acute injury period increase risk of stiffness?
Results
Deabate et al Am J Sports Med 2020
- meta-analysis of 8 RCTs
- 3 with 3 week cut off, 5 with 10 week cut off
- no evidence of increased risk of stiffness, complications, or poorer outcomes
https://pubmed.ncbi.nlm.nih.gov/31381374/
Early versus delayed ACL reconstruction
Issue
Does delayed ACL reconstruction or long wait to surgery result in increased injury?
Results
Prodomidis et al Am J Sports Med 2020
- systematic review and meta-analysis of timing of ACLR and meniscal tears
- meta-analysis of 5 RCTS demonstrated surgery > 3 and > 6 months after injury associated with increased medial meniscal tears
- https://pubmed.ncbi.nlm.nih.gov/33166481/
Repair versus Reconstruction
Concept
Early after ACL injury
Suture repair +/- internal splint +/- scaffold
Results
Murray et al Am J Sports Med 2020
- RCT of 100 patients average age 17
- injury < 45 days, midsubstance tear
- suture repair + scaffold
- no difference in laxity or functional outcome
- 14% repair v 6% reconstruction required revision at 2 years
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7227128/pdf/10.1177_0363546520913532.pdf
Graft Choices
Options
Bone patella tendon bone
Hamstring tendons
Quadriceps
Patella tendon


Disadvantages
- risk of patella fracture
- increased anterior knee pain compared to hamstring / quadriceps



Hamstring
Advantage
- less PFJ pain compared with patella tendon
Disadvantage
- some weakness of hamstrings which may be important in some athletes (sprinters)
Quadriceps
Advantage
- reduced AKP compared with patella tendon
- potentially thicker graft compared to hamstring
Revision Results
Persson et al Am J Sports Med 2014
- Norwegian ACL registry of 12,600 patients
- at mean follow up of 5 years, revision rate 4.2%
- revision rate patella tendon 2.1%
- revision rate hamstring 5.1%
- in 15 - 19 age group, 5 year revision rate 9.5% (HS) v 3.5% (PT)
- > 30 age group, 5 year revision rate 2.1% (HS) v 1.2% (PT)
https://pubmed.ncbi.nlm.nih.gov/24322979/
Lind et al KSSTA 2020
- Danish ACL registry, revision rate at 2 years
- revision rate quadriceps tendon 4.7%
- revision rate hamstring tendon 2.3%
- revision rate patella tendon 1.5%
https://pubmed.ncbi.nlm.nih.gov/31641810/
- NZ ACL registry
- 1200 young women between 15 and 20
- hamstring graft failure 7.7%
- BPTB graft failure 1%
Anterior knee pain
Marques et al Orthop J Sports Med 2020
- 438 patients, overall incidence of 6%
- 10% in PT, 3% in HS group
- risk increased by extension deficit (24% v 5%)
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7605008/
Allograft
Advantage
No donor site morbidity
Indications
Revision
Older patient
Disadvantage
Disease transmission
Cost
Slower incorporation
Increased failure rate
Results
Zeng et al Arthroscopy 2016
- meta-analysis of 9 RCTs autograft v allograft
- increased failures rates and poorer outcomes for irradiated allograft
- no difference for non irradiated allograft
https://pubmed.ncbi.nlm.nih.gov/26474743/
Synthetics
Advantage
No donor site morbidity
Disadvantage
Synovitis
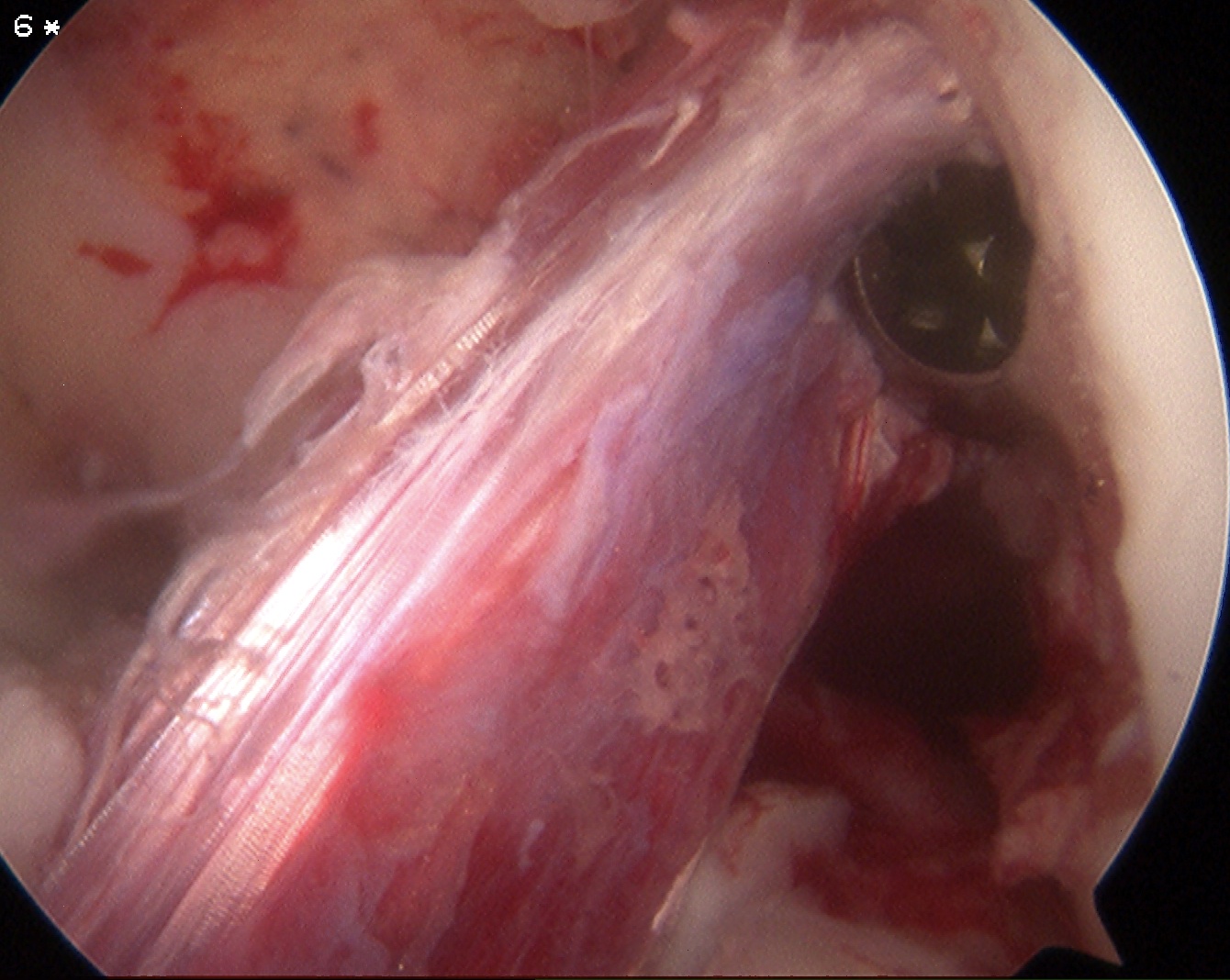
Results
- 55 cases single surgeon LARS at mean follow up 7 years
- 33% mechanical failure
- 40% secondary surgery
- giant cell synovitis seen at arthroscopy
Single v Double Bundle
Concept
Anatomically reproduce both bundles of ACL
? increase stability
Issues
Technically difficult
Results
Mascarenhas et al Arthroscopy 2016
- systematic review of meta-analysis
- improved stability in AP planes and rotational
- no difference in clinical outcomes or retear
Anterolateral ligament reconstruction / Extra-articular tenodesis
Concept
Injury to ALL at time of ACL injury
Contributes to rotational instability
Results
- meta-analysis
- addition of ALL / LET improves pivot shift
Getgood et al Am J Sports Med 2020
- RCT of hamstring ACL +/- LET
- 600 patients, grade 2 pivot, ligamentous lax, < 25
- addition of LET / ALL reduced clinical failure and re-rupture
Pinheiro et al Am J Sports Med 2023
- ACLR in 200 elite male professional soccer players
- 53% played at least one season at pre-injury performance
- 30% pre-injury performance at 2 years
- 22% pre-injury performance at 5 years
- LET doubled chance of return to play
- age > 25 and chondral defects poor prognosis
Trans-tibial v anteromedial portal drilling
Concept
Transtibial
- drill tibial tunnel
- insert guide through tibial tunnel to drill femoral tunnel
- tunnels more vertical
- tibial tunnel position dictates femoral tunnel position
Anteromedial portal drilling
- drill femoral tunnel through anteromedial portal
- anatomic ACL reconstruction
- allows femoral tunnel position at anatomic site of ACL insertion
- less vertical graft
- potentially more stable knee
Results
Loucas et al Orthop J Sports Med
- systematic review
- anteromedial drilling associated with improved AP and rotational stability
- anteromedial drilling associated with improved clinical outcome scores
https://pubmed.ncbi.nlm.nih.gov/34277881/
Knee position during graft fixation
Concept
Secure ACL graft on tibial side at full extension
- don't lose knee extension
- graft potentially not as tight
Secure ACL graft on tibial side at 30 degrees of flexion
- graft will tighten as go to full extension, potentially more stable knee
- can limit patient's ability to achieve full extension
Results
Chahal et al Arthroscopy 2021
- RCT of patella tendon fixation at 0 versus 30 degrees
- 169 patients
- no difference in reoperation, knee extension loss, stability or functional outcome
- patients fixed in full extension had increased activity scores and less pain
https://pubmed.ncbi.nlm.nih.gov/34952186/
Tunnel Placement
1. Intra-operative tunnels
Isometricity does not exist
- no point on femur that maintains fixed distance from point on tibia
- up to 3 mm elongation acceptable
- graft should tighten with increased extension
A. Tibial tunnel
Sagittal plane
- 7 mm anterior to PCL & central
- posterior 1/2 ACL footprint
Coronal plane
- 2/3 way towards medial tibial spine from anterior horn of lateral meniscus
Tunnel angle
- usually 55o
- reduce angle to shorten tunnel if have short graft
B. Femoral tunnel
More vertical placement of tunnel
- increased AP stability
- less rotational stability / pivot shift
Coronal plane
- 2 o'clock rather than 1 (right knee)
- 10 o'clock rather than 11 (left knee)
Sagittal plane
- want to be posterior
- identify back wall in flexion
- want 2mm of back wall behind tunnel
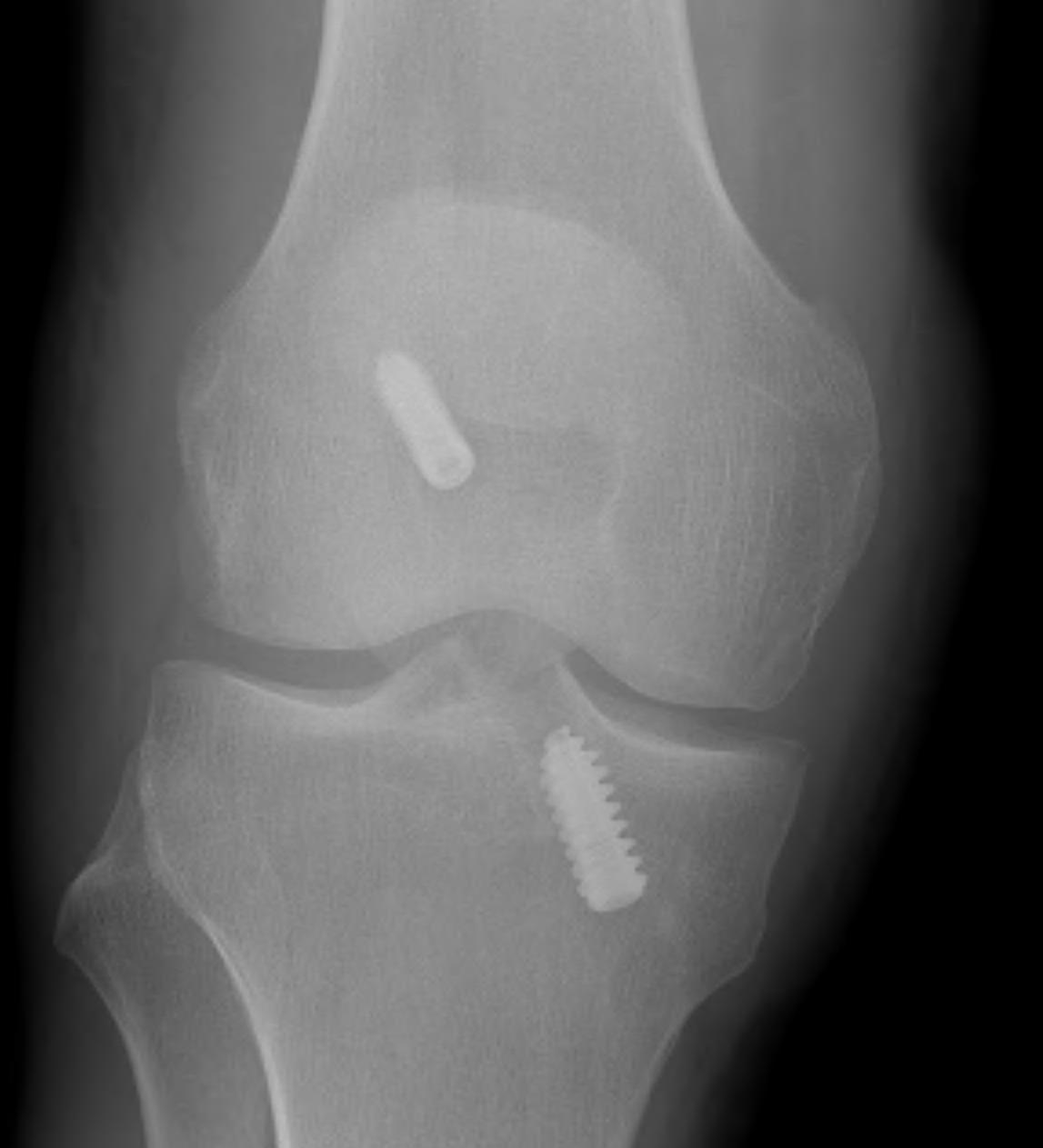
2. X-ray assessment
Lateral x-ray
Femoral tunnel
- intersection of line posterior femoral cortex and Blumensaat's line
Tibial tunnel
- posterior to Blumensaat's line in full extension
- parallel to Blumensaat's line
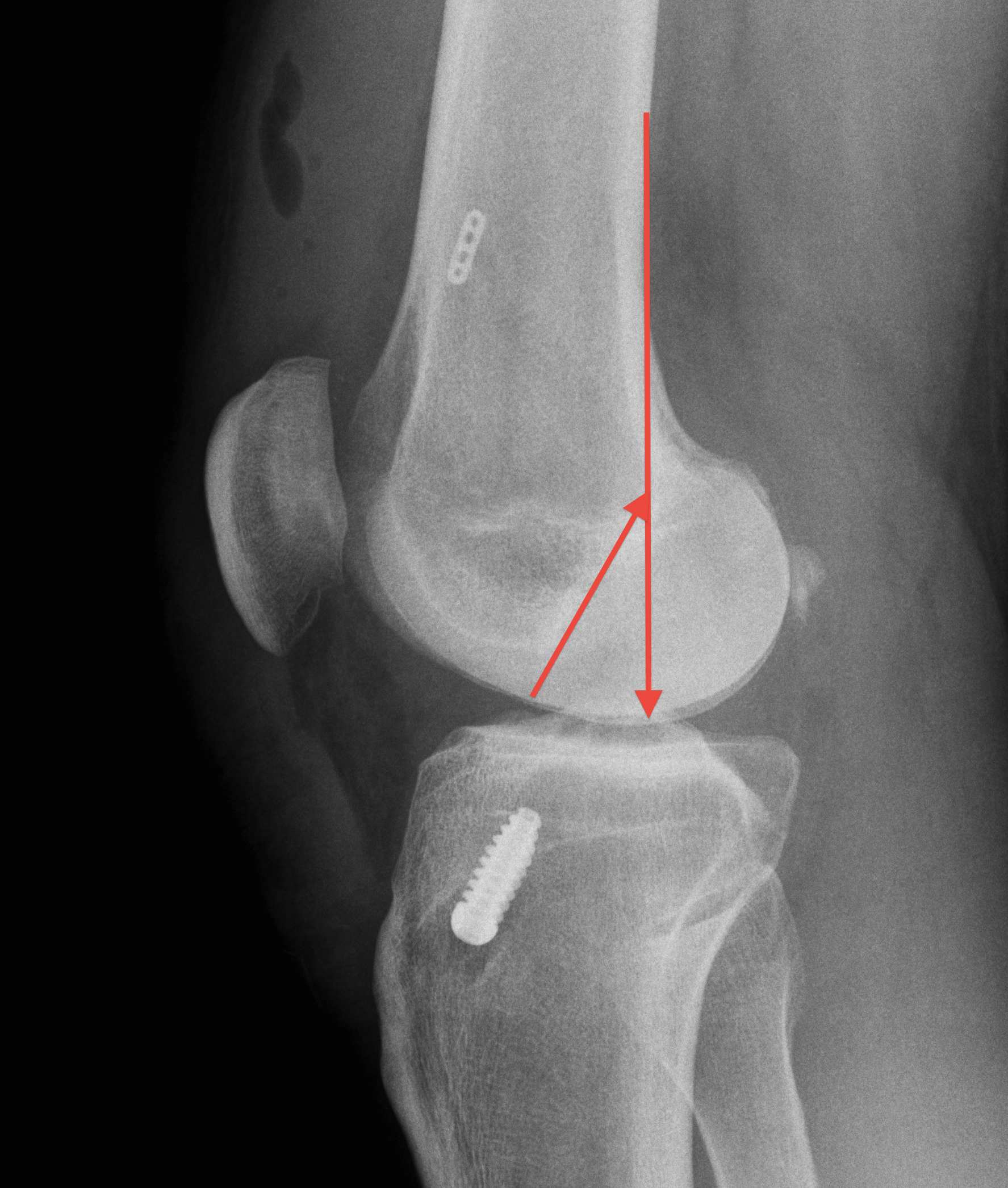

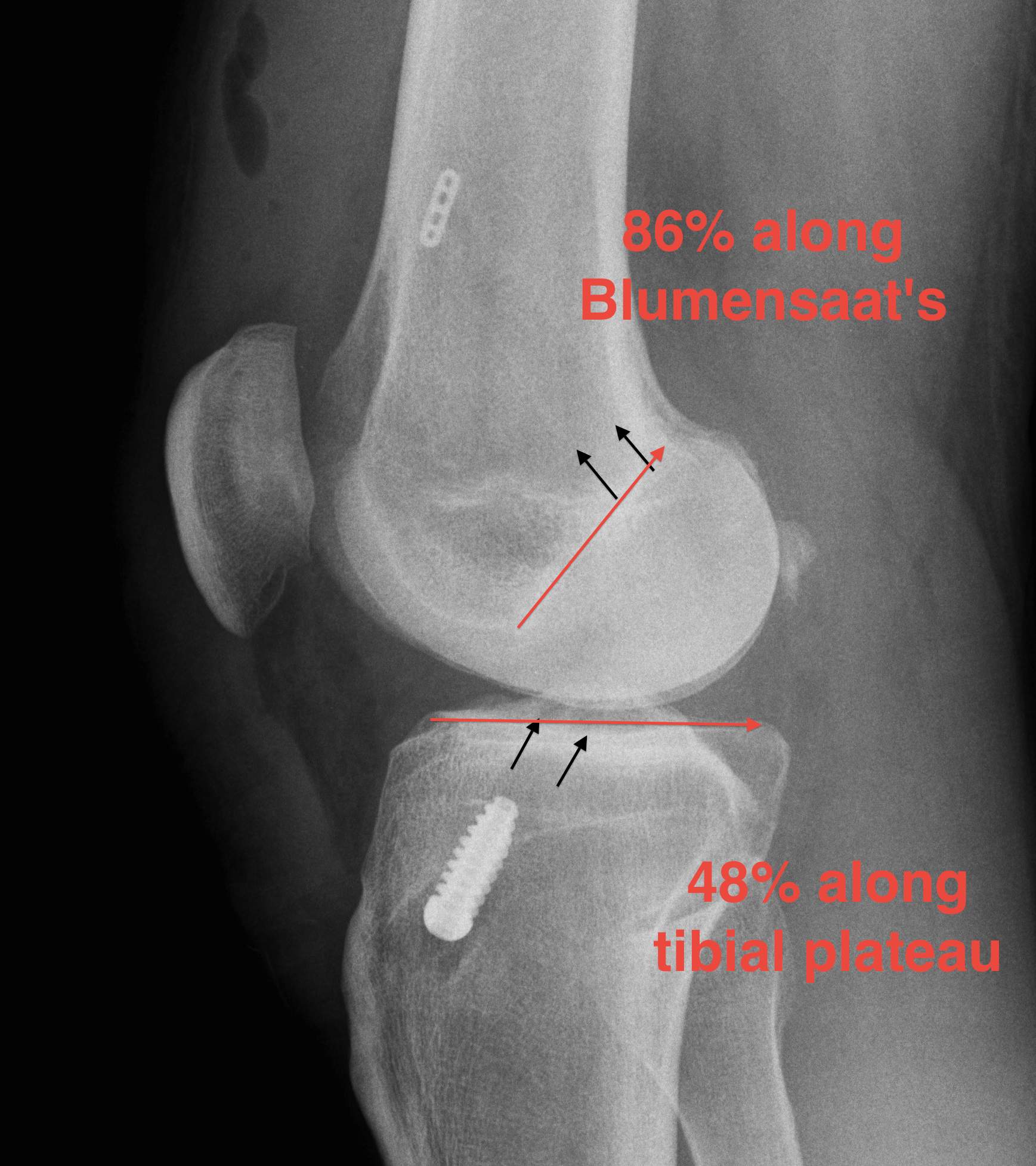
Pinczewski JBJS Br 2008
- 200 patients followed up over 7 years
1. Posterior femoral tunnel placement
- 86% along Blumensaat's line
2. Anterior tibia tunnel placement
- 48% along tibial plateau
- parallel to Blumensaat's
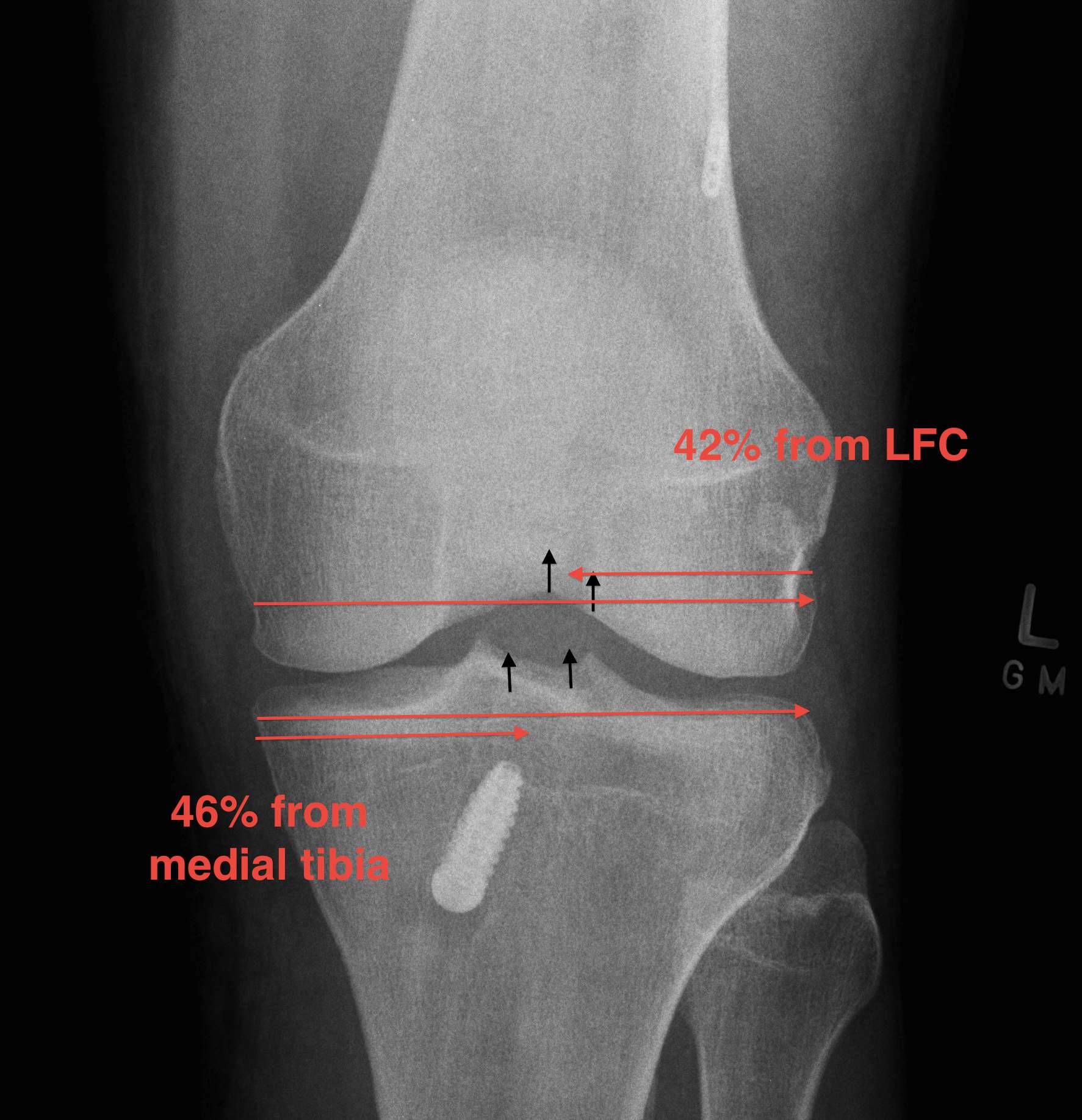
AP Xray
1. Medial tibial tunnel placement
- 46% (towards medial)
2. Lateral femoral tunnel placement
- 42% from lateral LFC
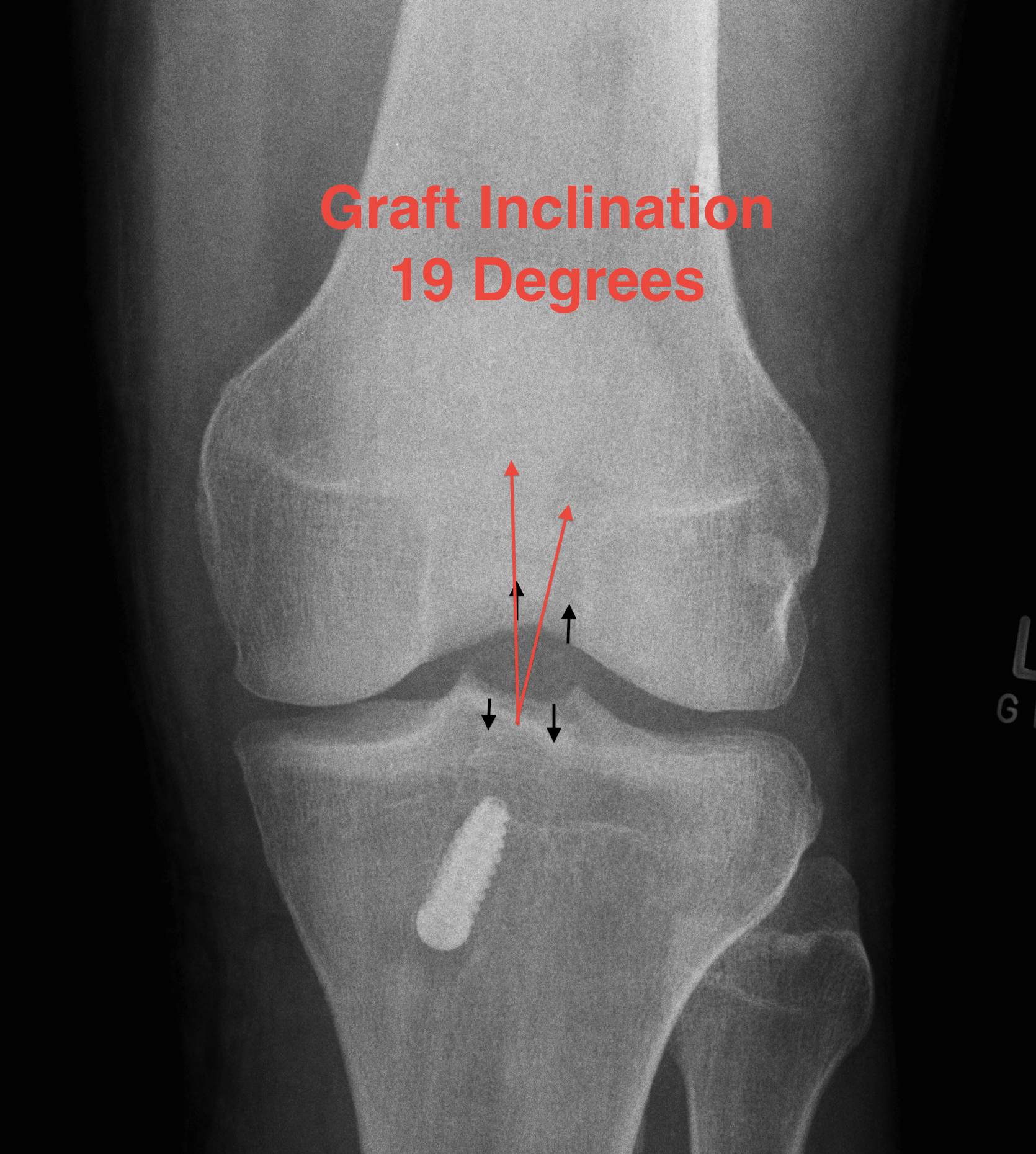
3. Graft inclination
- 19o
11% rupture rate over 7 years
- associated with posterior tibial tunnel placement
Good rotational stability
- 19o inclination in coronal plane
- avoid too vertical orientation
3. Incorrect tunnel positions
Tibial Tunnel
A. Anterior tibial tunnel
- impingement / limits extension / cyclops lesion
B. Posterior tibial tunnel
- impinge on PCL
- extension strain in extension
C. Lateral tibial tunnel
- impinges on lateral wall femoral condyle
Femoral Tunnel
A. Anterior Femoral Tunnel
- limits flexion
- increased strain in flexion / stretches graft
- increases risk of failure
B. Posterior Femoral Tunnel
- excessive strain in extension
C. Vertical Graft
Fu etal Arthroscopy 2003
- cadaver study of graft in 10 v 11 o'clock position
- demonstrated increased rotational instability in 11 o'clock
Options for drilling femur
1. Trans - tibial
Traditional techique
- drill tibial tunnel first
- place guide up tibial tunnel onto femur
Advantage
- cannot damage MFC
Potential disadvantage
- tibial tunnel sets position of femoral tunnel
- tends to make the graft more vertical
Technique
- drill femur with knee at 90o
2. Anteromedial portal
Advantage
- allows separation of femoral from tibial tunnel
- can place femoral tunnel lower on femoral wall
Disadvantage
- places drills and reamers close to MFC
- must be careful not to damage cartilage
Technique
- must hyperflex knee
- or femoral tunnel may exit in PFJ
Femoral Tunnel Back wall blow-out
Problem
Cannot use RCI screw to secure femoral side
Avoid by
1. Using posterior offset femoral guide
- divide tunnel size required in half and add 2
- 6mm for 7.5 mm hamstring tunnel
- 7mm for 10 mm BPTB tunnel
2. Appropriate knee flexion when drilling femoral tunnel
- hyperflexing knee if using AM portal
- 90o of flexion if using transtibial technique
Options
1. Endo-button
- don't need back wall for fixation
2. Redrill tunnel
- change angle by flexing knee +++
- get in good bone stock
3. Fix in over the top position
- pass graft around back of femoral condyle using curved hemostat
- may need medial parapatella approach
- lateral approach to femur
- fix to femur with screw / staple
- can pass around lateral intermuscular septum and LCL
Notchplasty
Issue
- smaller notch increases risk of re-rupture / stretching by causing graft impingement
- more necessary with larger grafts i.e. BPTB
- required if presence of notch osteophytes
Disadvantage
- notchplasty can lateralise
- important to only debride anterior portion of notch
- do not debride lateral wall or will lateralise the femoral graft
Techique
- trial with guide wire / reamer / chondrotome / graft
- check for lateral wall impingement
- check for roof impingement
- notchplasty as required
Graft Fixation
Graft fixation is weakest link first 6-12 weeks
- BPTB 6-10 weeks to incorporate
- HS 12 weeks (bone grows into tendon resembling Sharpey's fibres)
After 12 weeks the weak link is the graft
Options
Aperture Fixation
Interference screw
- metal / bioabsorbable
Suspensory Fixation
Endobutton
Transfix

Fauno et al Arthroscopy 2005
- compared transfix and endobutton
- demonstrated increased tunnel widening with fixation away from joint i.e endobutton
Screws
Diameter
- biomechanical studies in tibia with hamstring
- line to line screw size less strong than tunnel diameter + 1
Length
- probably more important than diameter in hamstring
- has been demonstrated than increasing length increases fixation
- increase number of threads available for fixation
Divergence
- important with bone block
- must keep divergence below 200
Central / eccentric placement
- no significant difference
Metal v bioabsorbable
Mascarenhas Arthroscopy 2015
- meta-analysis
- no difference in outcome
- increased knee effusion, femoral tunnel widening, and screw breakage with bioabsorbable