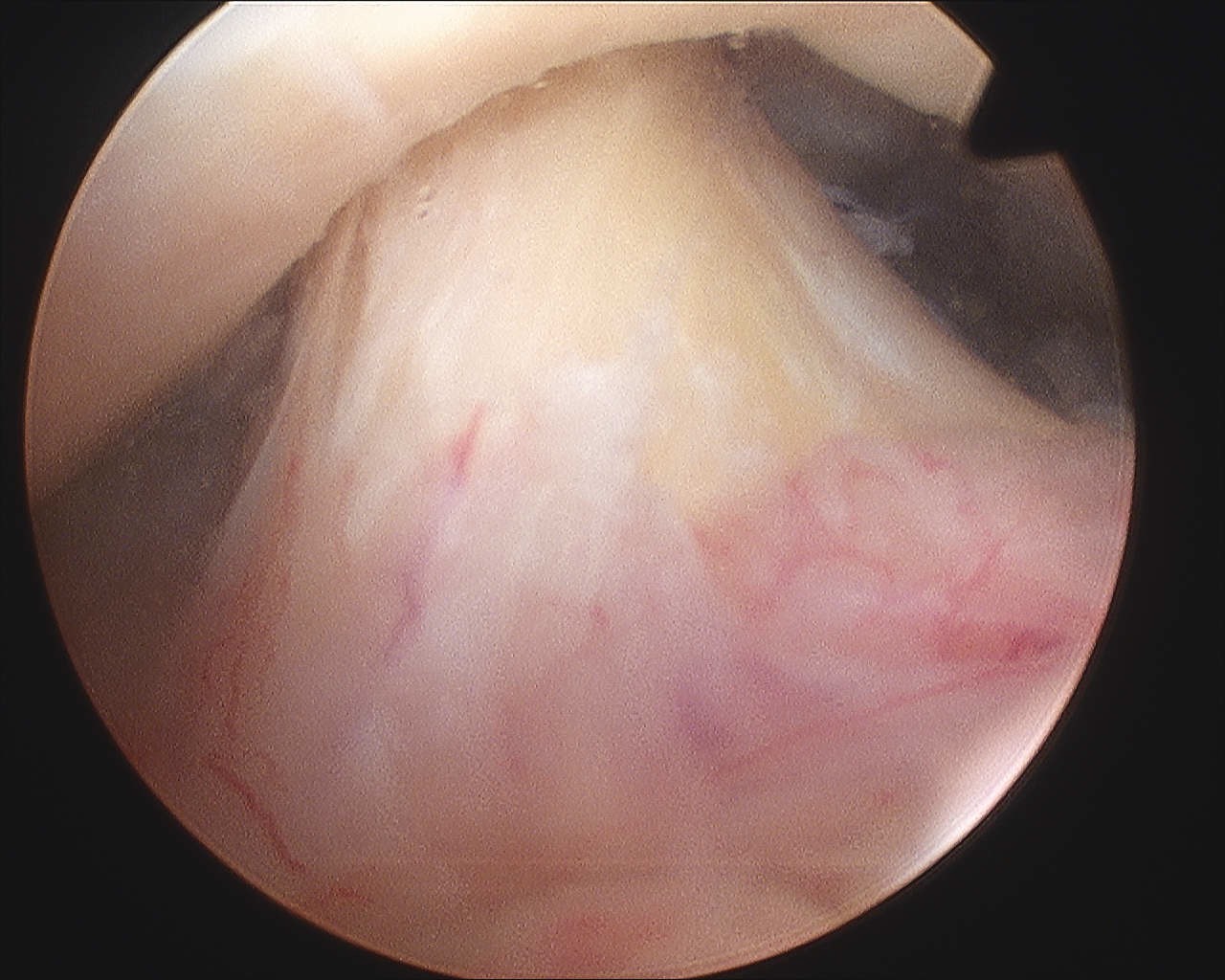
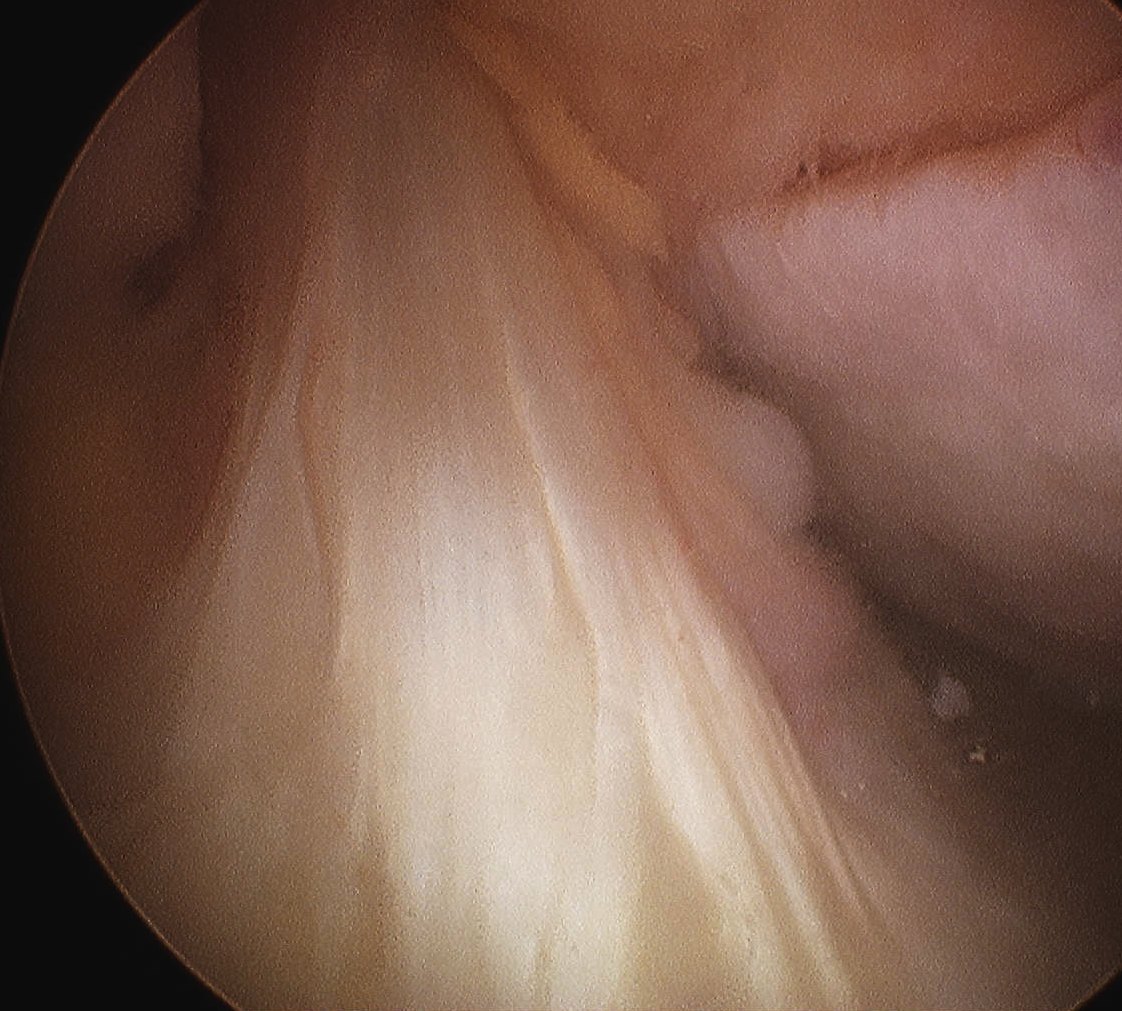
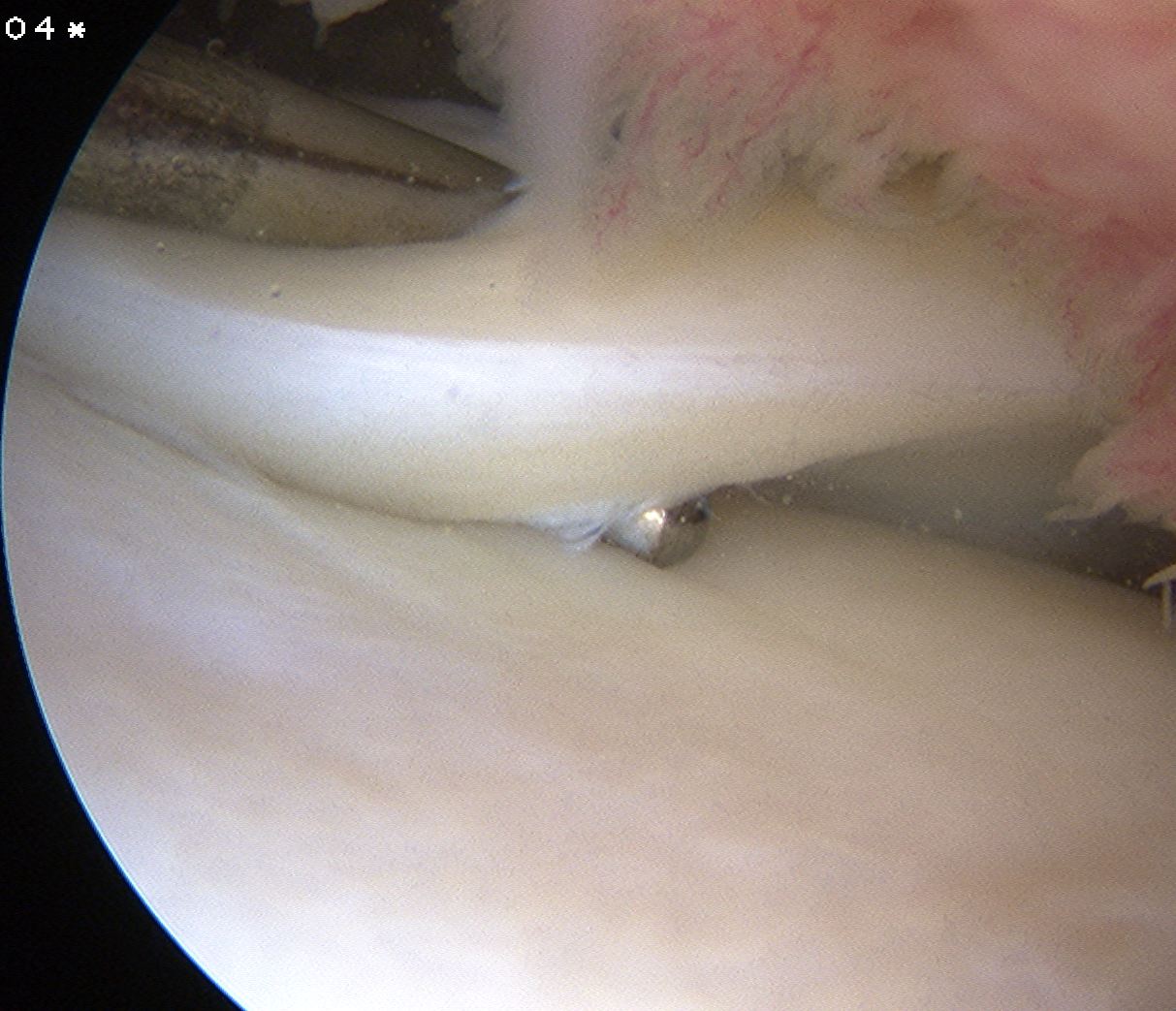
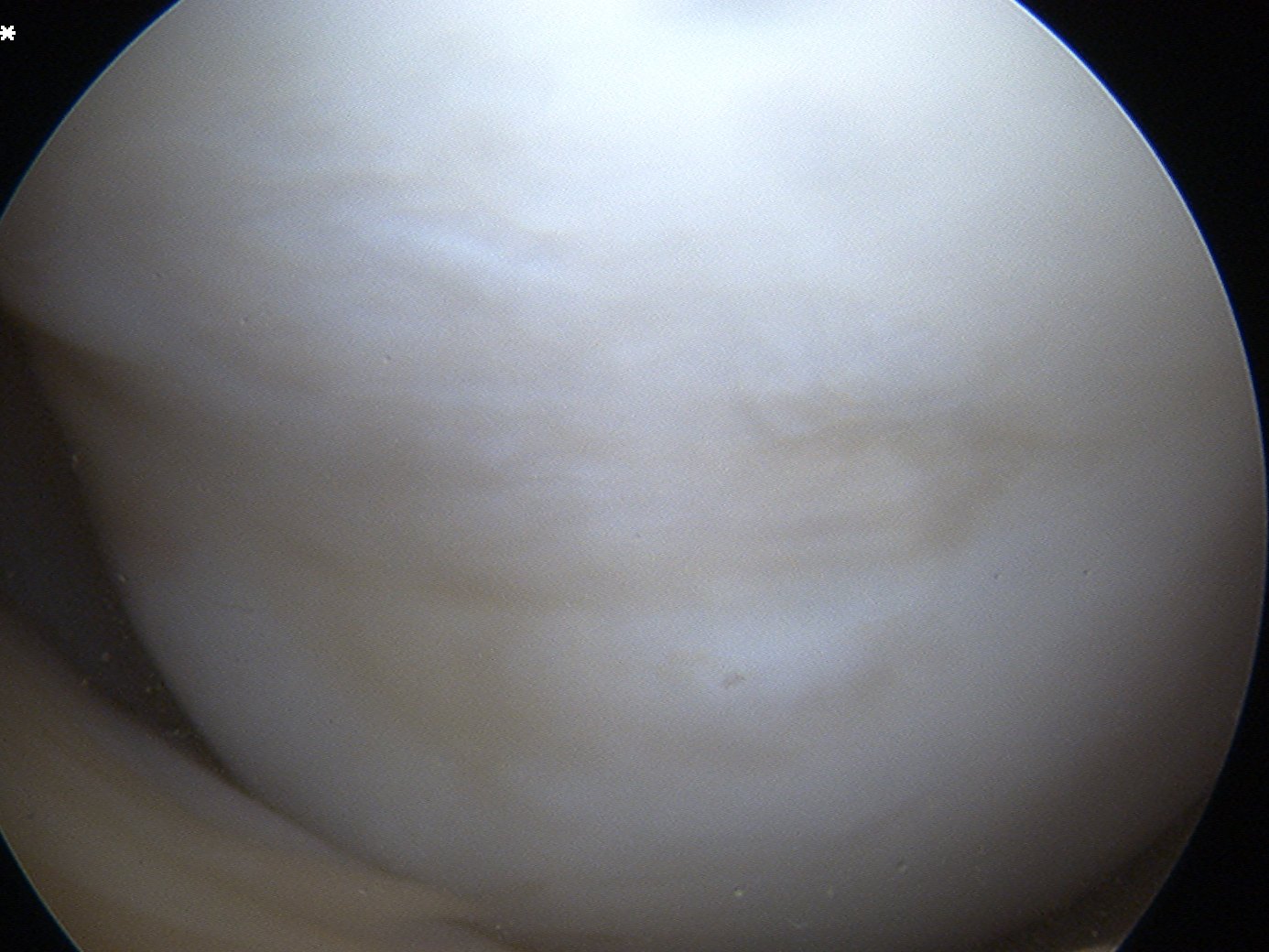
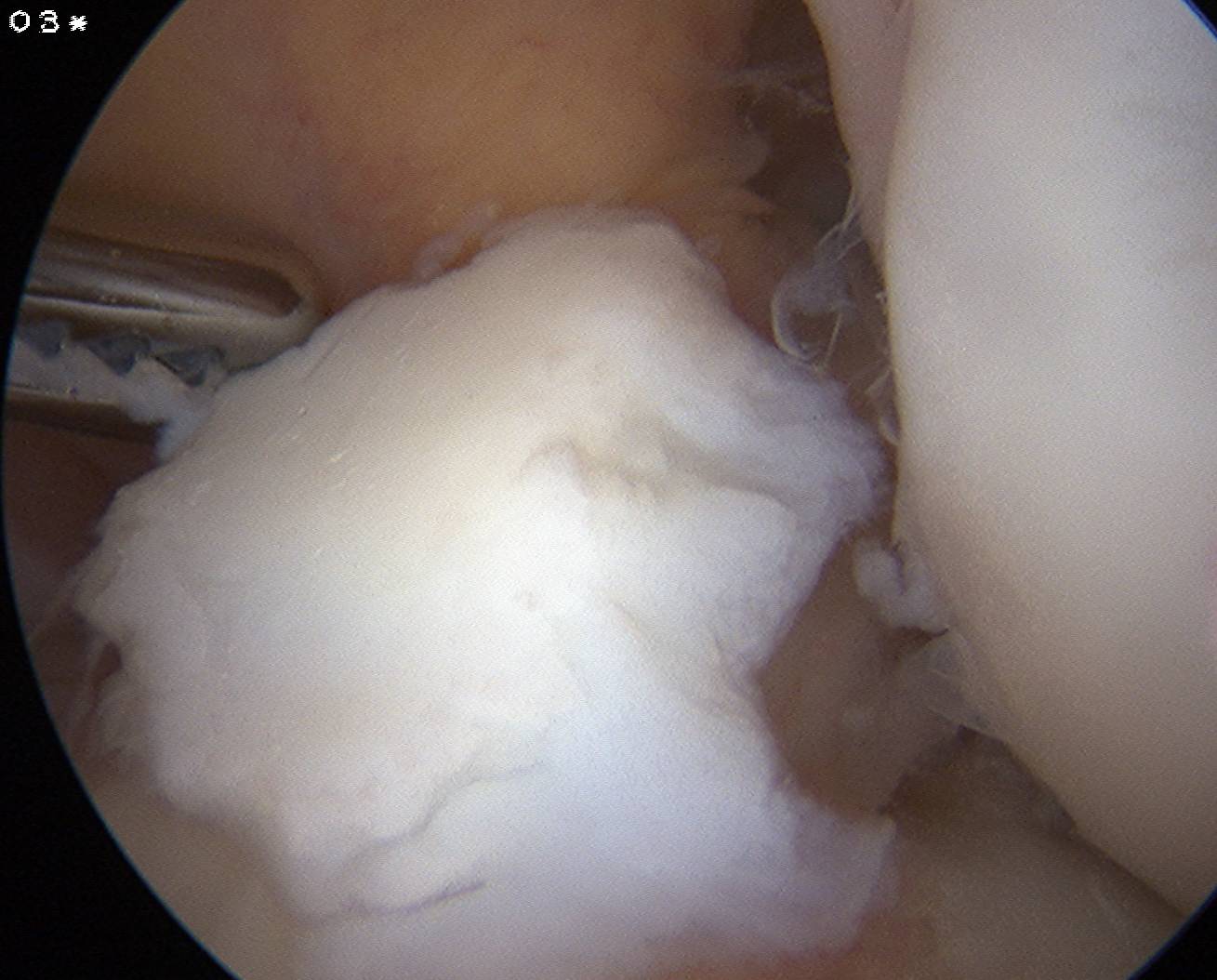
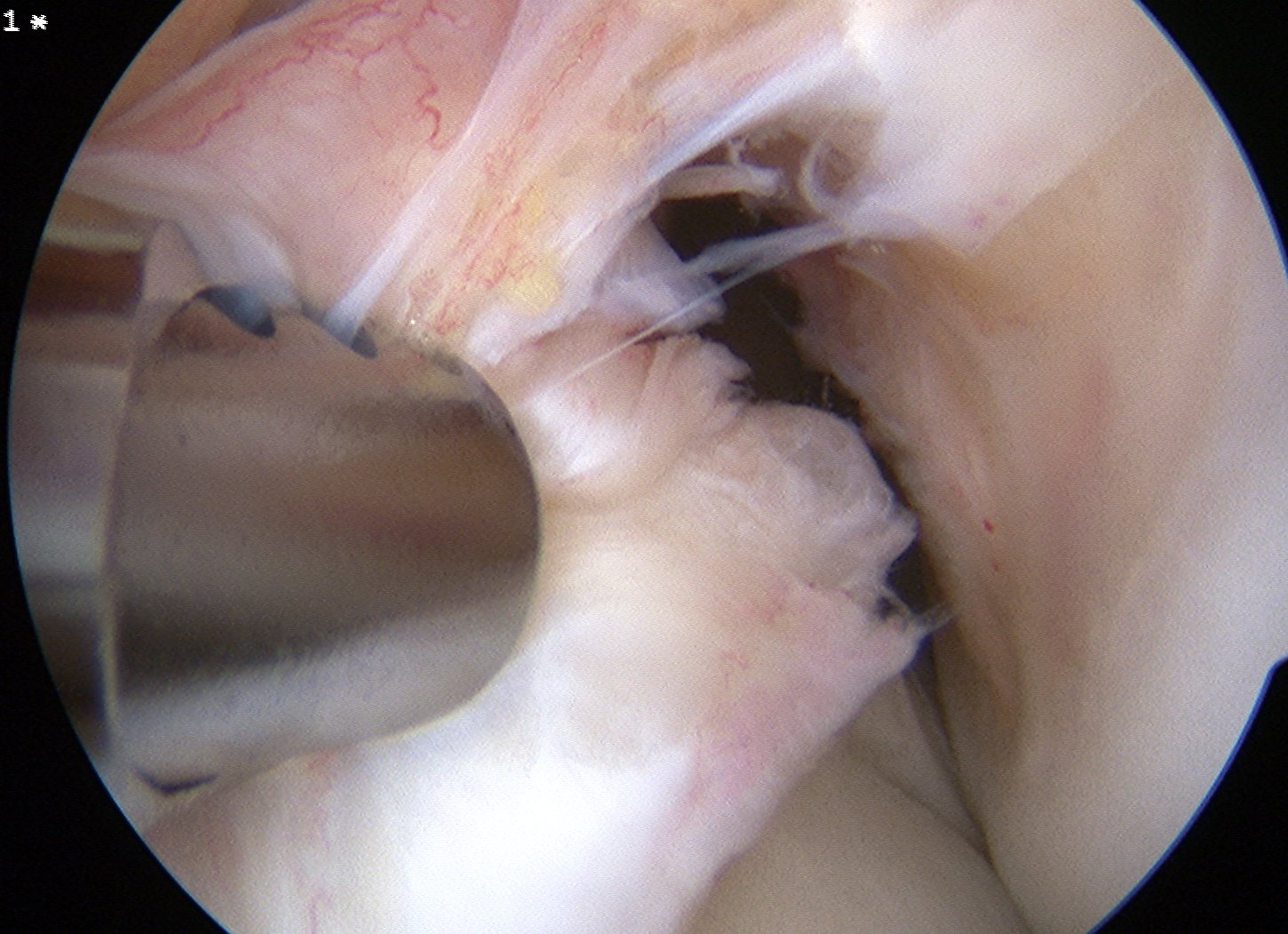
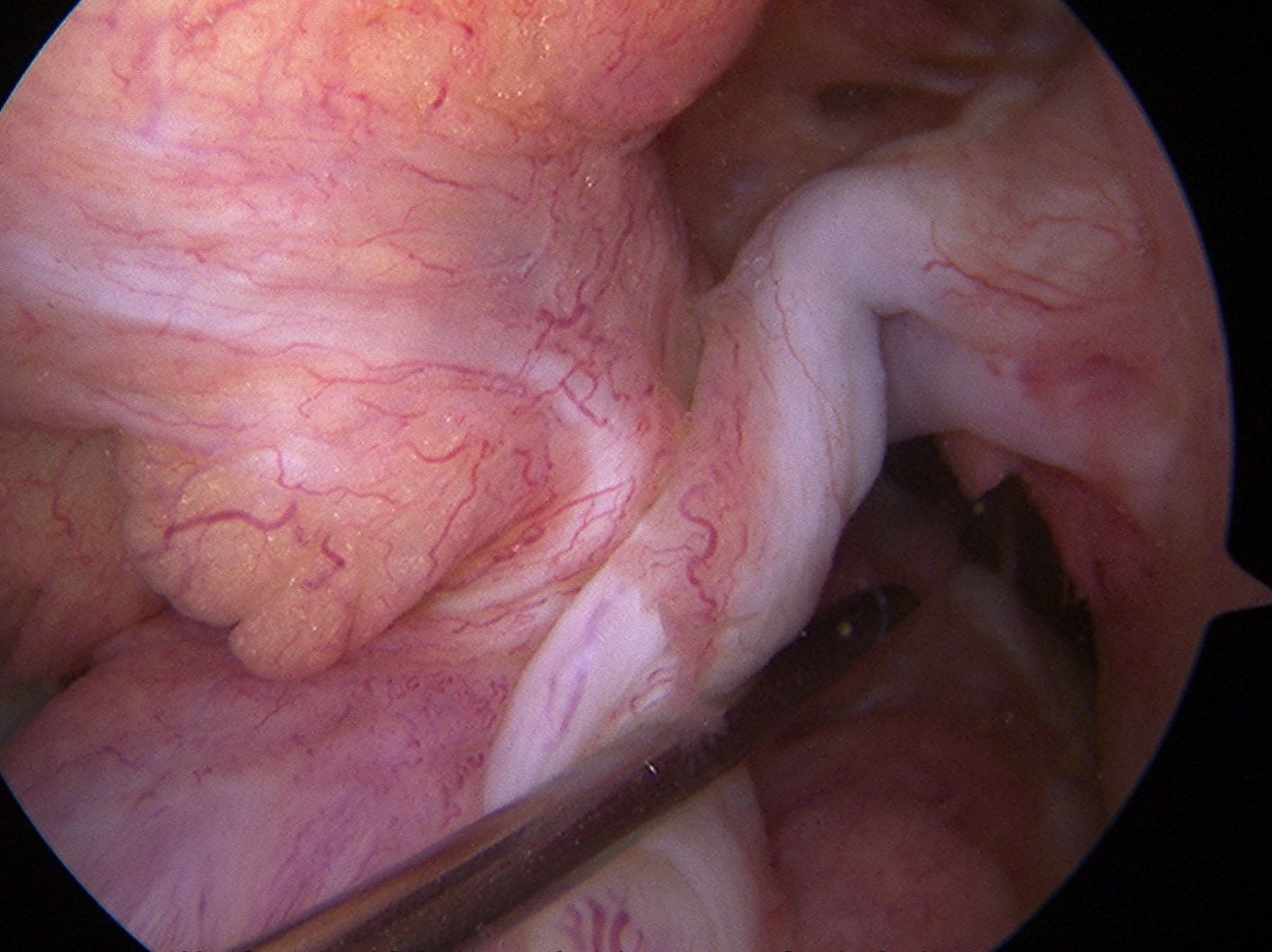
Arthroscopy images of right knee demonstrating normal ACL
Anatomy
ACL is intracapsular and extra-synovial
Direction
In full extension
- subtends 45o angle in sagittal plane
- 25o angle in coronal plane
Dimensions
- 25-40 mm long
- 7-10 mm wide
Two bundles
Anteromedial and posterolateral bundles
- described regarding point of tibial insertion
Anteromedial
- smaller
- tight in flexion
- test with anterior draw
Posterolateral
- larger
- tight in extension
- test with Lachman / Pivot Shift
Nerve
- posterior articular nerve / branch tibial
Arterial supply
- middle geniculate
Origin
- posterior on the medial wall lateral femoral condyle
- semicircular
Insertion
- passes anteriorly, distally and medially
- oval shaped fossa anterior and between the tibial spines
- majority of ligament passes deep to transverse meniscal ligament
- a few fascicles blend with anterior horn of lateral meniscus
- wider and stronger than femoral insertion
Histology
Collagen and elastin arranged in less parallel configuration than tendons
- allows increase in length without large increase in internal stress
Ligaments attach to bone directly or indirectly
Cruciates attach directly / 4 histological zones
- ligament
- nonmineralised fibrocartilage
- mineralised fibrocartilage
- cortical bone
Indirect attachments via periosteum and fascia
- i.e. tibial insertion of MCL
Function
1° Stabilizer
- prevents anterior translation
2° Stabilizer
- lateral & medial stability
Incidence
1:1500 - 1:3500
Mechanism
Non contact deceleration producing valgus twisting injury
Deceleration / ER / Valgus
Associated Injury
Meniscal Injury
60% lateral meniscus
- associated with acute ACL rupture
- classically posterior horn
- many will heal

40% medial meniscus
- associated with chronic ACL rupture
Fractures
- 10-20%
- associated with characteristic bone bruise patterns on MRI
- see femoral chondral impressions from hyper-extension injury

Chondral Injuries
MCL
- 10-20%
History
1. 50% describe a "Pop"
2. 75% haemarthrosis
- intra-articular swelling or effusion within the first 2 hours after trauma suggests hemarthrosis
- swelling that occurs overnight usually is an indication of acute traumatic synovitis / meniscal tear
3. Immediate inability to weight bear
DDx hemarthrosis
Rupture of a cruciate ligament
Osteochondral fracture
Peripheral tear in the vascular portion of a meniscus
Tear in the deep portion of the joint capsule
Intra-articular fracture of tibial plateau / distal femur / patella
Examination
Laxity Grading Lachmans / Anterior Draw
1+: mild instability < 5mm
2+: moderate instability 5-10mm
3+: severe instability >10mm
Lachman's
20 - 30° Flexion
- removes effects of bony contour / menisci i.e. 2° constraints
- stabilise femur with one hand, other hand behind tibia with anterior force
- sublux the tibia forward
85% sensitivie when awake
100% under anaesthetic


Anterior Draw
Knee at 90° Flexion with hamstring relaxed
- foot in neutral
- sit on foot to stabilise
- hands behind tibia and pull forward
- has to > 3mm different to contralateral knee


Foot in 15° of External Rotation
- medial structures tightened in this position
- reassess anterior draw
- if have positive anterior draw in this position suggests associated posteromedial injury
- ACL + MCL / Med Capsule / OPL
Foot in 30° of Internal Rotation
- lateral structures tight in this position
- reassess anteior draw
- if have positive anterior draw in this position suggests associated posterorlateral injury
- ACL / LCL / PLC Complex
Pivot Shift
Concept
- ACL torn
- lateral tibia subluxed anteriorly in extension
- reduced in flexion
Technique
- knee moves from extension to flexion
- valgus force applied to knee
- apply axial load
- mimicking weight bearing
Findings
- in extension the LTC is subluxed anteriorly
- in extension ITB is in front of flexion axis and is extender of knee
- as the knee is flexed
- ITB moves behind the flexion axis and becomes flexor of knee (20-40°)
- this reduces the LTC
“The relocation of the subluxed lateral tibial condyle as the extended knee is flexed”
“This occurs as the ITB line of function changes so as to become a flexor rather than an extensor of the knee”


Need 4 things for a pivot shift
1. MCL to pivot about
2. ITB to reduce on flexion
3. Ability to glide ie no meniscal tear
4. °FFD
Grading
Jakob et al JBJS Br 1987
- 3 grades with foot in varying degrees of rotation
Grade 1: Pivot shift with foot IR
Grade 2: Pivot shift with foot neutral
Grade 3: Pivot shift with foot ER
X-ray
Usually normal
Segond Fracture
- small avulsion fracture of lateral proxima tibia
- is sign of lateral capsular avulsion
- pathognomonic of ACL tear
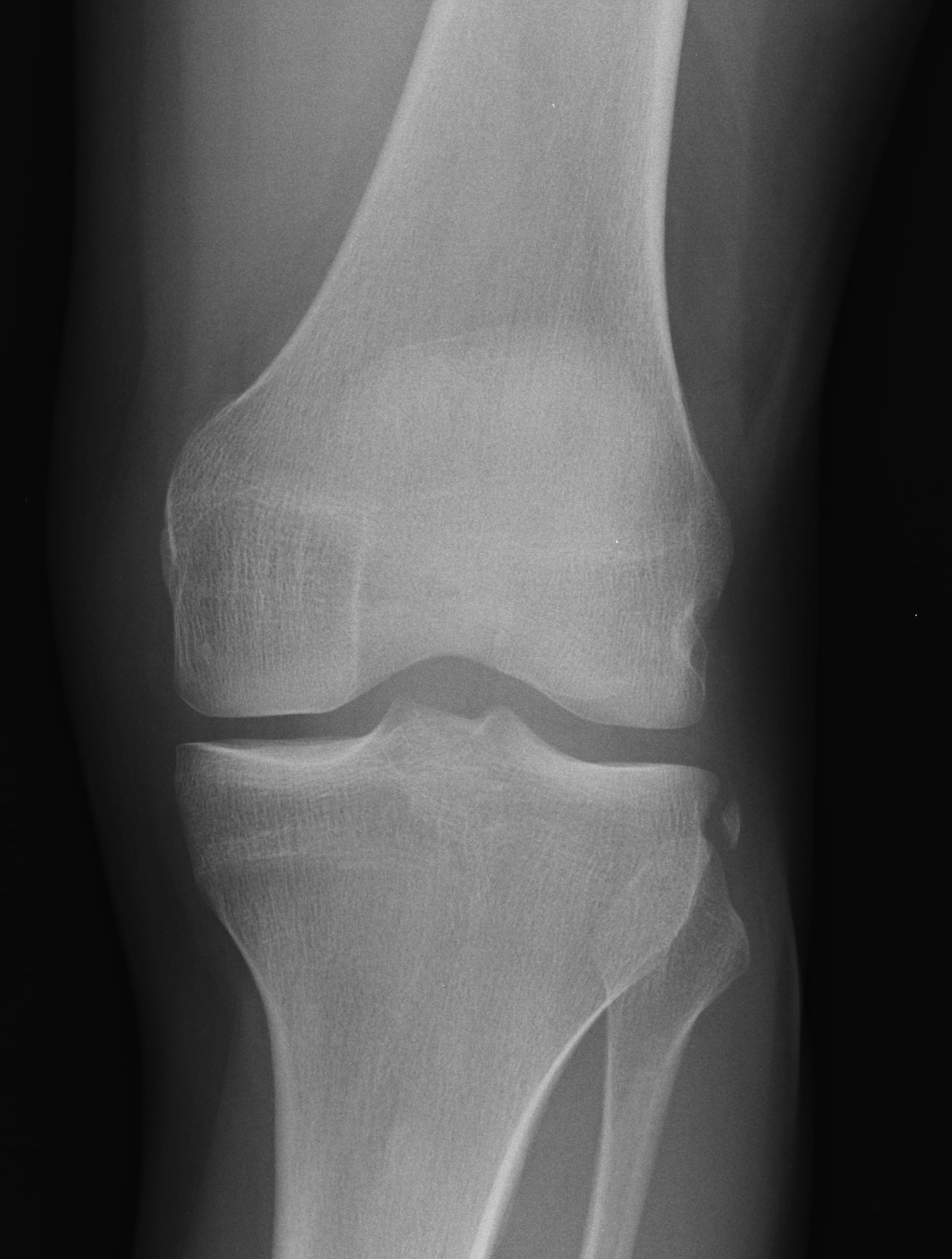

Tibial avulsion
- more common in children
- can be seen in adults




MRI
Accuracy
Smith et al Am J Roentgenology 2016
- meta-analysis of 3T MRI accuracy in diagnosing ACL tears in comparison to arthroscopy
- 92% sensitive and 99% specific for ACL tears
https://www.ajronline.org/doi/10.2214/AJR.15.15795
Normal ACL on MRI


Characteristics
- straight structure
- able to see continuity of fibres from tibial to femur
- parallel to intercondylar notch
- no anterior subluxation of the tibia
- normal to have some increased signal due to adipose and synovial tissue
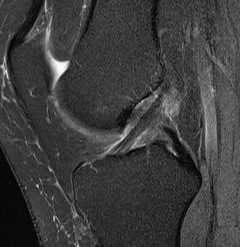
Torn ACL on MRI
Findings
- high signal intensity / oedema in ACL, especially acutely
- unable to identify continuous fibres from tibia to femur
- loss of taut, straight line of fibres

Sagittal TI MRI with no femoral attachment

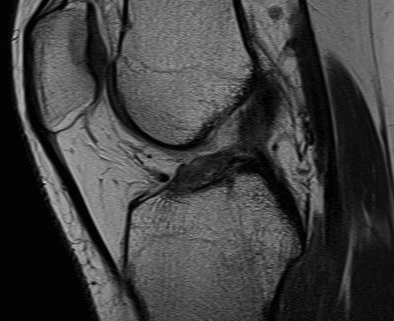
Sagittal T2 MRI with midsubstance ACL tear Sagittal T1 MRI with midsubtance ACL tear
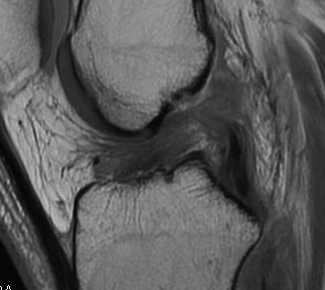
Sagittal MRI with complete ACL rupture
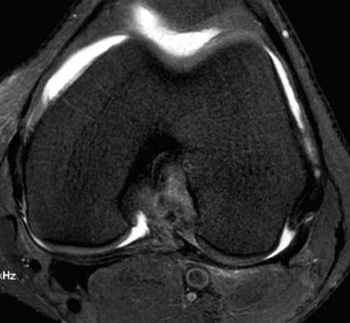
Axial MRI demonstrating no ACL attachment to lateral femoral condyle
ACL Partial Tear

Bone bruising patterns
- pathognomonic
- caused by the knee pivot shifting
- terminal sulcus of LFC
- posterolateral tibial plateau

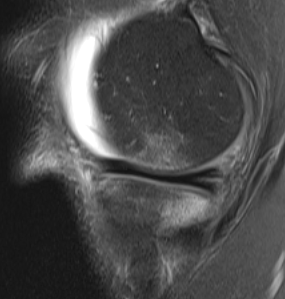

Coronal MRI with LFC bone bruising Sagittal MRI with terminal sulcus LFC Sagittal MRI with bone bruise posterolateral tibial plateau
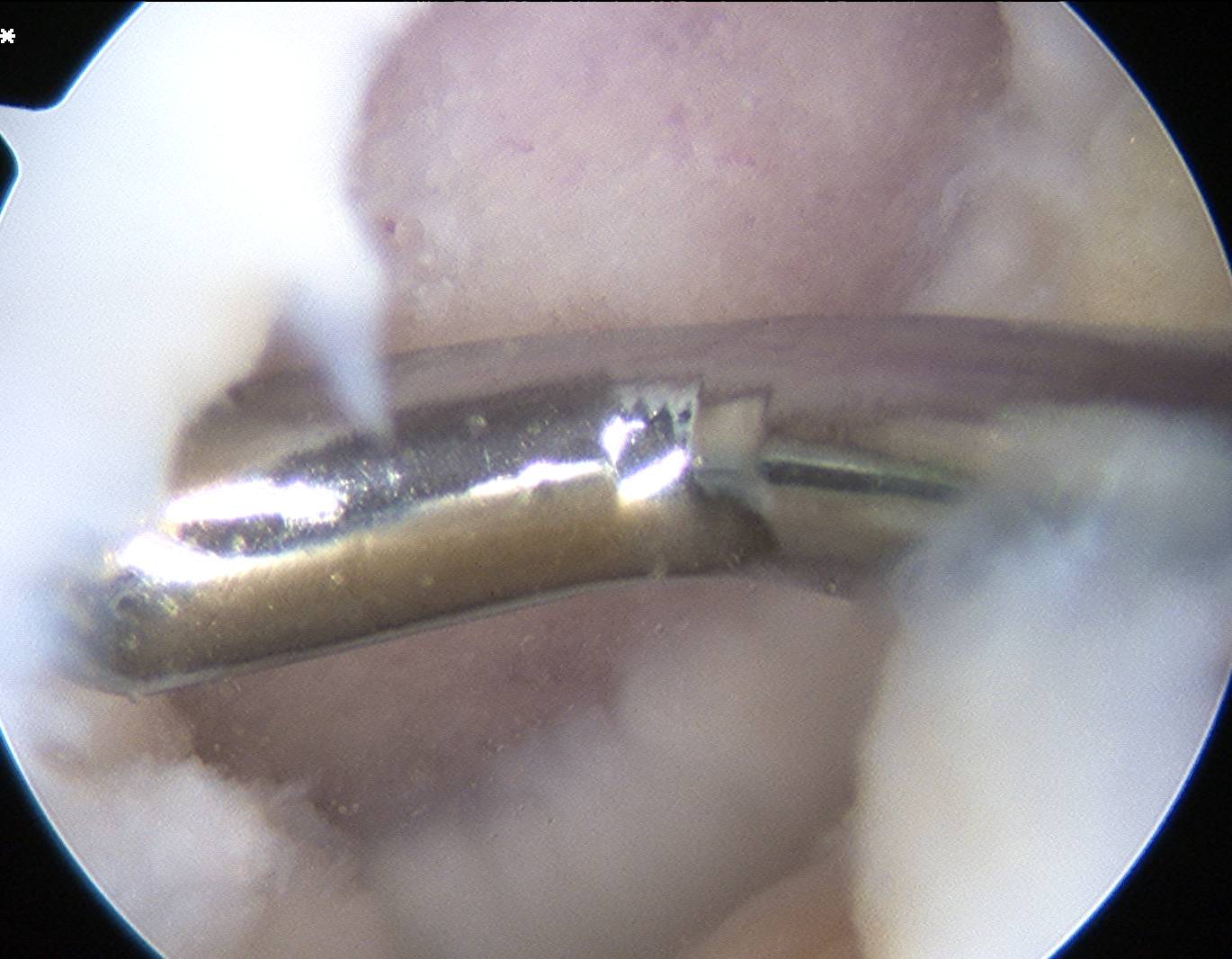
Arthroscopy
Findings
- empty lateral wall
- ACL healed onto PCL
Arthroscopy of left knee showing no ACL attachment to lateral femoral condyle

Arthroscopy of right knee showing no ACL attachment to lateral femoral condyle
Arthroscopy of left knee demonstrating only a few minor fibres attached to lateral femoral condyle