Indications
Rheumatoid arthritis
Osteoarthritis / post-traumatic arthritis
Acute unreconstructable fracture > 60
Haemophilia
- elbow joint commonly involved
- 90% of haemophiliacs
Contra-indications
Sepsis
Poor soft tissue cover skin triceps
Under 60 years
Charcot Joint
Design
1. Unlinked
Depend on integrity of MCL / LCL
Risk postoperative instability
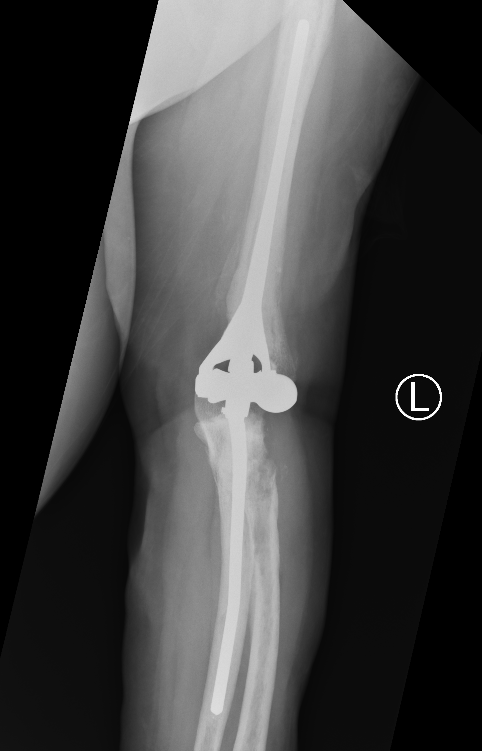
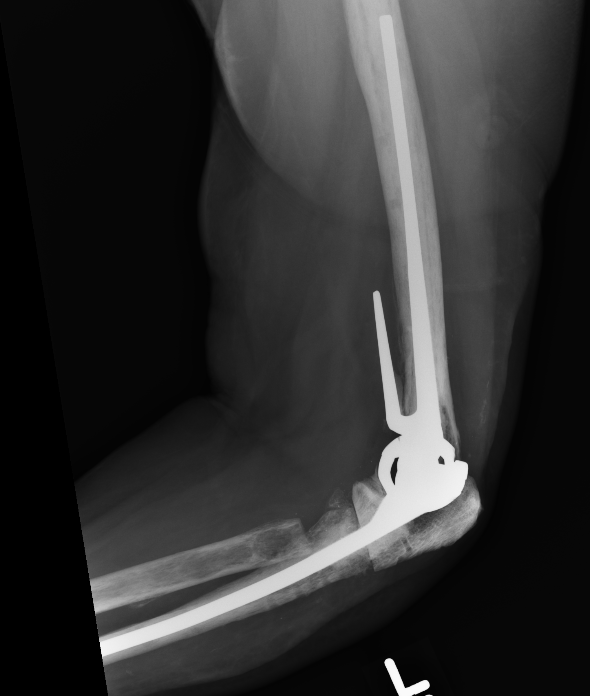
2. Linked
Normal elbow has degree of varus / valgus laxity during flexion / extension
Sloppy hinge / semiconstrained
- metal on poly linked bearing
- some varus / valgus and rotational laxity
- anterior flange on humerus with bone graft to resist rotational force



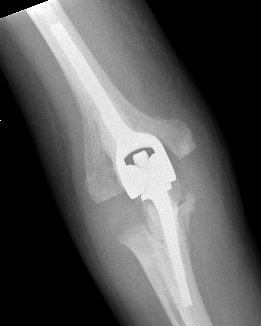
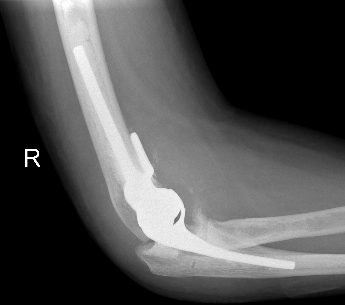
Coonrad-Morrey Discovery Elbow Latitude
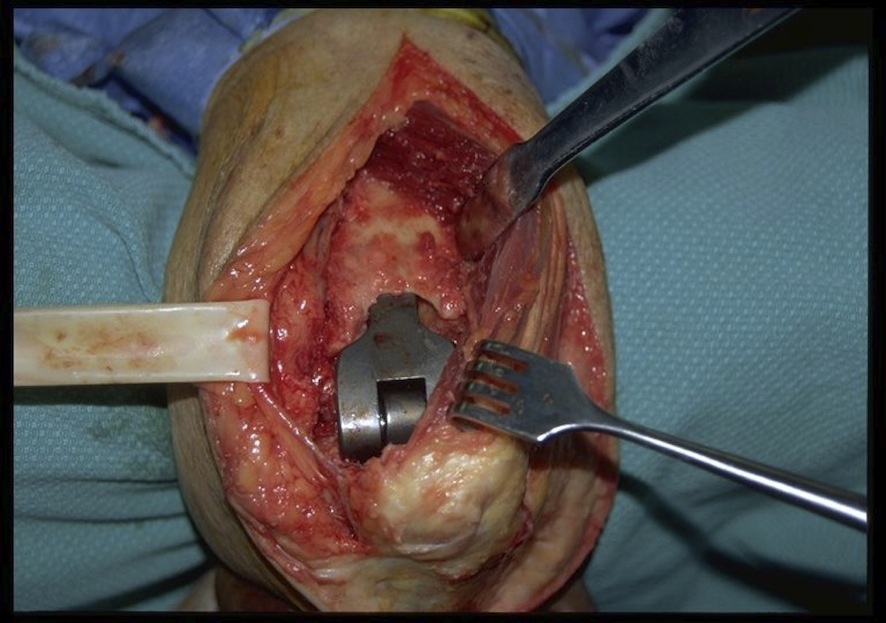
Exposure / Approach / Triceps management
Triceps Options
|
Triceps off (some interruption of the triceps mechanism) |
Triceps on |
|---|---|
|
Advantage: Excellent exposure Disadvantage: Risk triceps insufficiency |
Advantage: Little risk triceps failure Disadvantage: More difficult exposure especially to ulna |
|
Options: Triceps splitting Triceps reflecting Triceps turn down |
Options: Lateral para-olecranon Para-tricipital |
Triceps split
AO surgery triceps split approach
Technique
- midline split of triceps tendon
- tendon feathered off the olecranon medially with FCU
- tendon feathered off the olecranon laterally with anconeus
Triceps reflecting / Bryan Morrey
AO surgery triceps reflecting approach
Technique
- release and protect ulna nerve
- mobilize medial border of the triceps including tendon from olecranon
- anconeus dissected off the ulna
- reflect triceps and anconeus from medial to lateral
- entire extensor mass is subluxated over lateral epicondyle
- leave
Triceps turndown
Inverted V in triceps fascia
Triceps sparing
Vumedi video triceps sparing TEA
AO surgery lateral para-olecranon approach
Para-triceps / lateral para-olecranon approach
- lateral and/or medial windows
- both humerus and ulna are typically instrumented through a lateral window to protect the ulna nerve
Results
- compared 46 triceps off to 37 triceps on approach
- no triceps ruptures in triceps on approach
- 7/46 (15%) incidence of triceps rupture in triceps off approach
- 3 patients who underwent triceps repair developed deep infections
Technique Total Elbow Arthroplasty
Vumedi video triceps sparing TEA
Vumedi video Coonrad-Morrey approach and prosthesis
JBJS Essential Surgical Technique


Approach
Lateral decubitus
- can limit hyperflexion of elbow for instrumentation humerus / ulna
Supine with arm over patient
- requires arm holding by assistant
Posterior Approach
- full thickness skin flaps
- identify and protect ulna nerve
Triceps on / triceps off approach
Distal Humerus
- release LCL / MCL from humerus and tag for later repair
- elevate anterior capsule off humerus
Dislocate Elbow
Arthroplasty
1. Size capitellum and trochlea with spool
- insert into olecranon and over radial head
2. Prepare ulna
- resect olecranon fossa
- can remove tip olecranon
- find entry to IM canal & pass IM guide
- prepare canal
- insert trial ulna stem
3. Prepare humerus
- rough cut trochlea
- find entry to IM canal & pass IM guide
- ensure correct rotation (5 degrees internal rotation)
- use IM rod to attach jig for distal humeral preparation
- release anterior capsule from humerus for anterior flange
- prepare humeral canal
- insert trial humeral stem
4. Trial reduction
5. Insert cement restrictors / implant ulna and humeral prosthesis
6. Insert bone graft under anterior flange
7. Link components
8. Repair collaterals if needed
Post op
Splint 2 weeks till wound healed
Then active ROM
Results
- systematic review of TEA with 10 years follow up
- 1429 elbows
- overall revision rate at 10 years 15%
- loosening at 10 years 13%
- infection 3%
- dislocation 4%
- nerve injury 2%
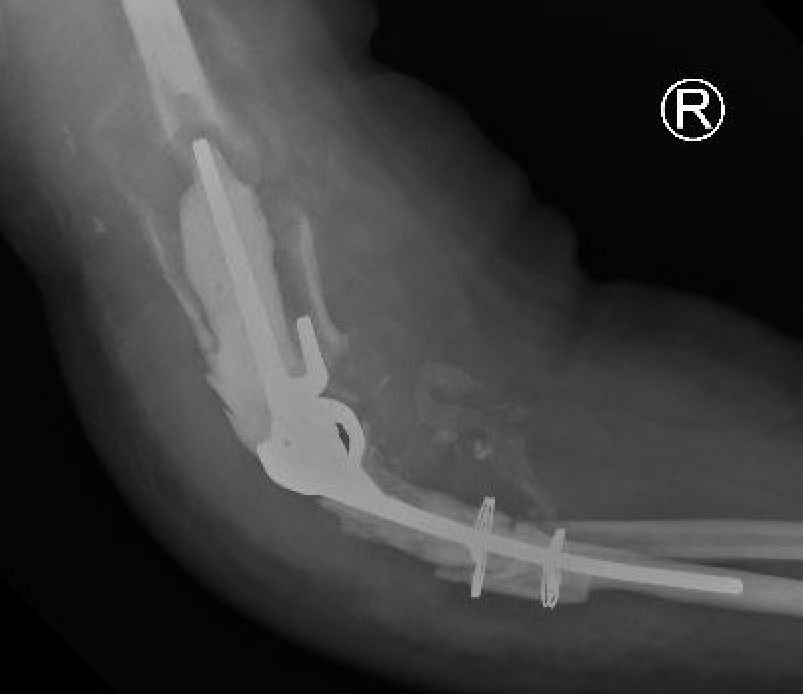
Complications
Intraoperative fracture
Humeral condyles
Ulna at risk
- slight bend / small diameter / relatively thin cortical bone
- perforations can allow cement extrusion
Infection
Diagnosis
Progressive lucency on xray
ESR / CRP - not always helpful, especially in patients with inflammatory arthritis
Aspiration
Open biopsy and culture



Risk factors for infection
- previous surgery
- younger patients
- previous infection
- rheumatoid arthritis
- obesity / diabetes
- drainage post-op / delayed wound healing
Management
- systematic review of 309 TEA infections
- Staph aureus most common (42%) followed by coag neg Staph 33%
- irrigation and debridement 56%
- resection arthroplasty 71%
- one stage revision 67%
- two stage revision 81%
Technique
JBJS surgical technique elbow resection deep infection




Triceps failure
Incidence
- systematic review of 4825 TEAs
- triceps insufficiency 4.5%
- 22% in revision TEA
- 10% in TEA for post-traumatic OA
- highest with triceps reflecting approach
Management
Direct repair
Anconeus rotational flaps
Achilles tendon allograft
Results
- 16 cases triceps insufficiency
- combination repair / anconeus flap / achilles allograft
- 14/16 good or excellent
- 14 cases of achilles allograft reconstruction
- bone plug inserted into olecranon
- 11/14 good or excellent results
Aseptic Loosening
- systematic review of 3000 TEA
- loosening rates 10% for unlinked and 14% for linked prosthesis
Results
- revision with allograft - prosthesis composite
- 25 patients
- one nonunion / one malunion
- 84% TEA survival
Ulna allograft - prosthetic revision TEA
Instability
- systematic review of 3000 TEA
- instability - dislocation / subluxation
- 5% for unlinked and 1% for linked prosthesis
- occurs in linked prosthesis by failure of constraint mechanism
Periprosthetic Fracture


Ulna nerve injury
Partial / Radio-capitellar arthroplasty

Watkins et al Bone Joint J 2018
- 30 elbow undergoing lateral resurfacing
- 100% survival at 8 years
- improved outcome scores and ROM