Definition
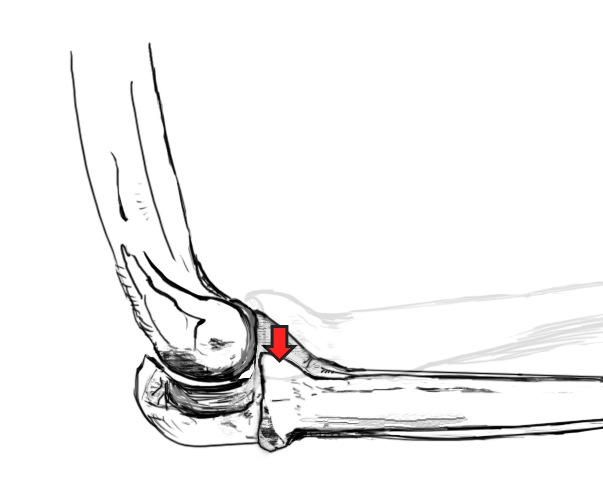
Dynamic posterior instability of the radial head relative to the capitellum in flexion
Secondary to injury to the Lateral Collateral Ligament (LCL) complex
Anatomy LCL complex
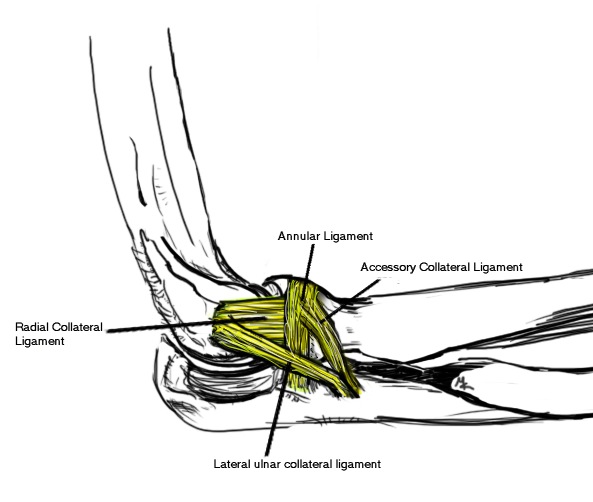
Four components
Need injury to lateral UCL and radial collateral ligament for instability to occur
| Lateral Ulna Collateral Ligament | Radial Collateral Ligament | Accessory Collateral Ligament | Annular ligament |
|---|---|---|---|
|
Lateral epicondyle to supinator crest |
Lateral epicondyle to annular ligament | Lateral epicondyle to annular ligament and supinator crest | Anterior and posterior sigmoid notch |
| Most important |
|
Etiology
Trauma
- elbow dislocation
- LCL complex fails to heal
Iatrogenic - tennis elbow release / Kocher approach
Ligamentous laxity
Cubitus varus
History
Lateral elbow pain
Clicking
Instability
Examination
Combine external rotation / supination with valgus and axial loading
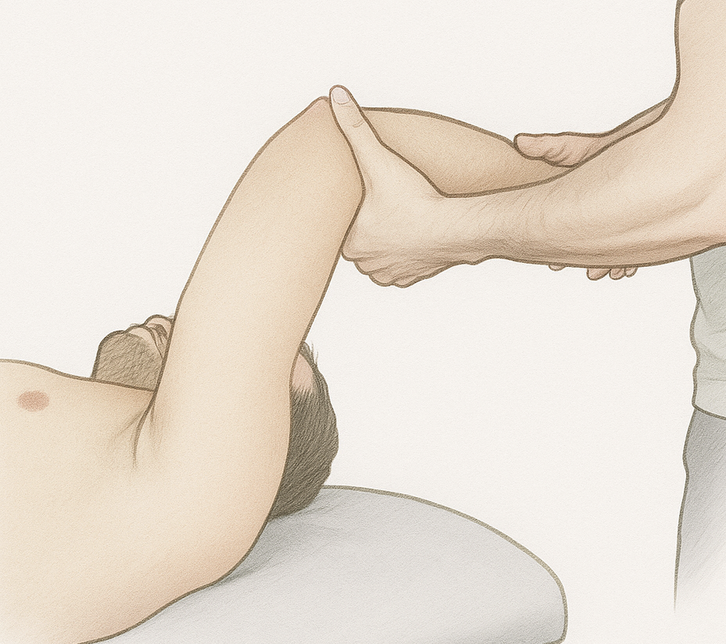
| Pivot Shift Test | |
|---|---|
|
Patient supine with hand over head - examiner at head of bed - elbow fully extended and forearm supinated - elbow resembles knee in this position
Valgus stress with axial load & slowly flex elbow - at 30 - 45o the radial head subluxes posterolaterally - patient feels apprehension / pain - reduces as the elbow flexes more
|
|
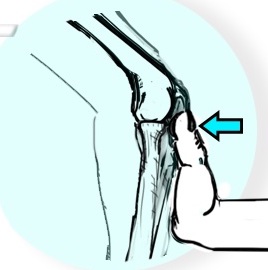
| Table top test | |
|---|---|
|
Push up on table with forearms in supination - in flexion the radial head subluxes - patient has apprehension and pain
|
Pain and apprehension relieved by anterior pressure on radial head |
 |
  |
MRI
Normal


PRLI
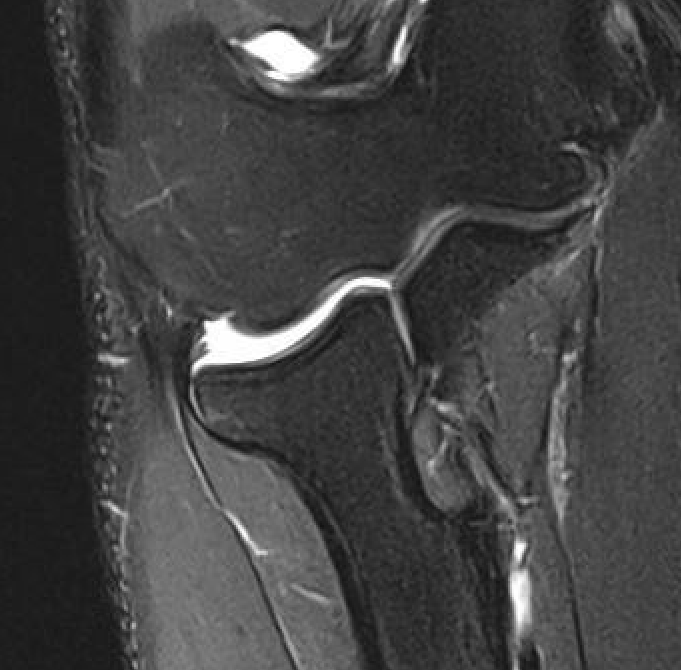
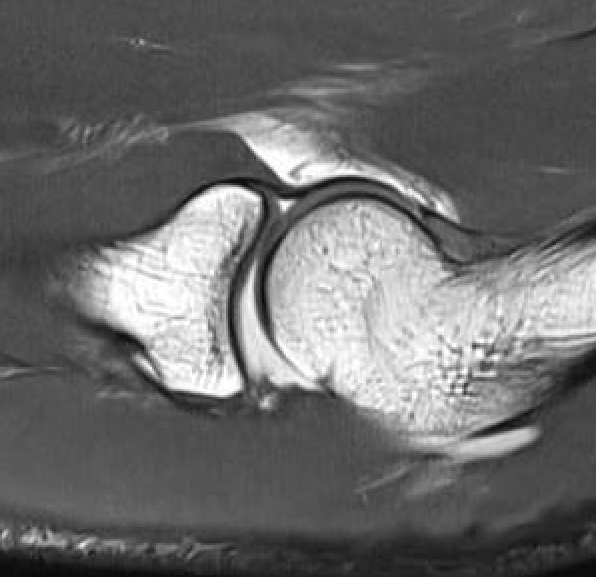
Subtle instability of the radiocapitellar joint
Nonoperative management
Ineffective
Operative management
Options
1. Repair +/- internal brace
2. Reconstruction with graft - open versus arthroscopic
Graft reconstruction
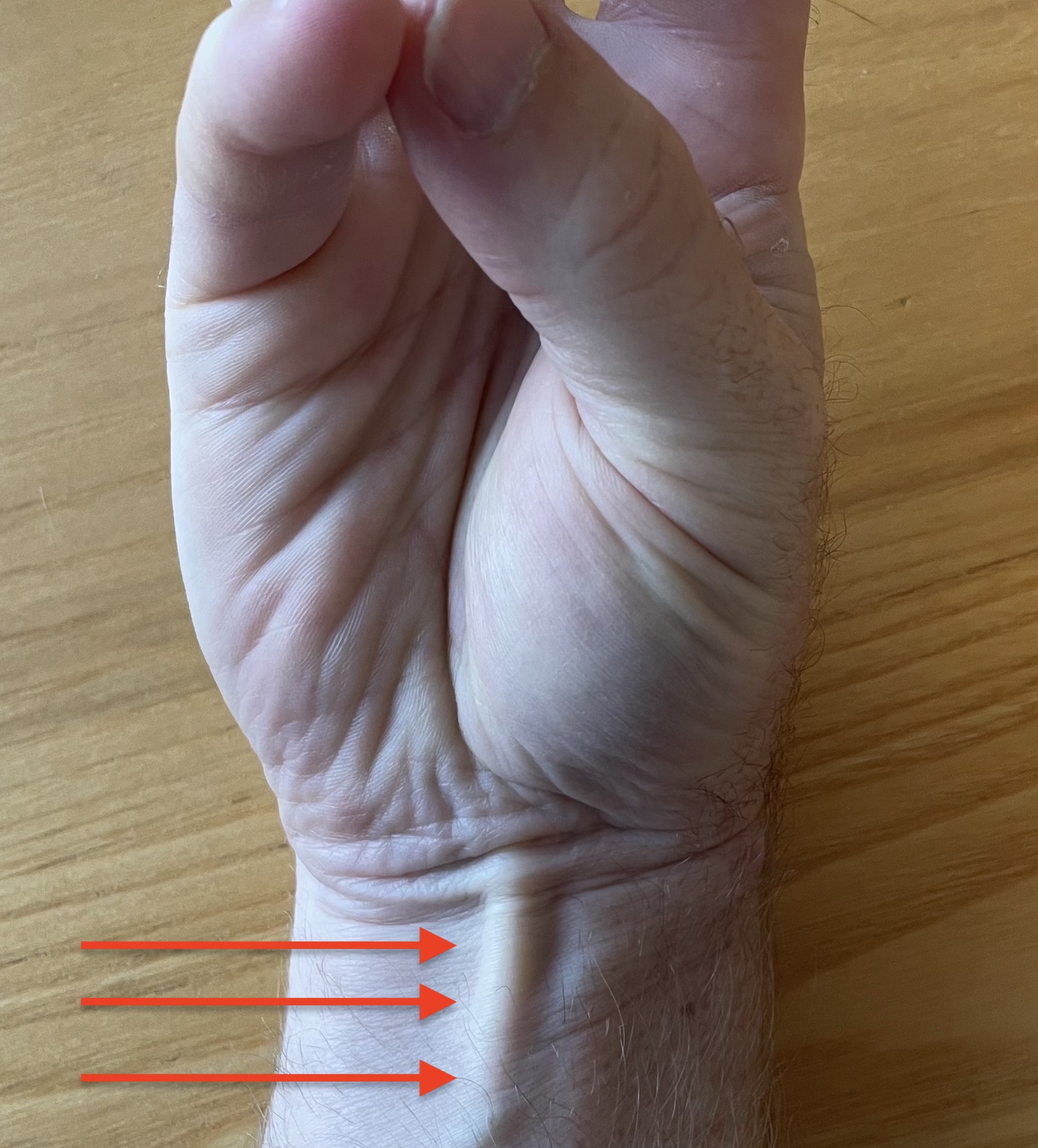
Graft choices
Palmaris longus - present 85% / press thumb and finger together
Gracilis / semitendinosis - autograft or allograft
Triceps tendon autograft
Vumedi 2 incision palmaris longus harvest technique video

Approach
Kocher approach - between anconeus and ECU
Open Techniques

Vumedi LCL reconstruction docking technique epicondyle with transverse tunnel ulna video
Arthrex LCL reconstruction with docking technique ulna and epicondyle video
Arthroscopy techniques LCL reconstruction PDF
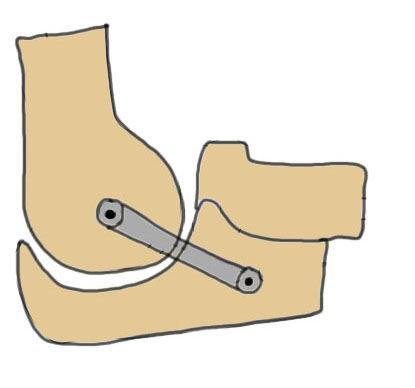
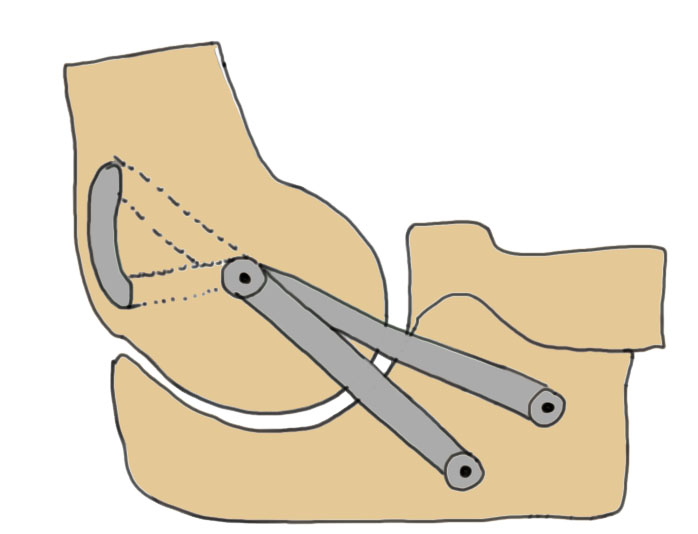
Distal tunnel
- supinator crest ulna - level of annular ligament
- docking technique with suture anchor
- transverse tunnel
Proximal tunnel
- lateral epicondyle at isometric point - can use flouroscopy
- typically docking as insufficient bone for transverse tunnel
Tension with elbow at 30 - 40o of flexion
Arthroscopic technique
Arthroscopy techniques arthroscopic LCL reconstruction PDF
Results
Repair versus reconstruction
- systematic review of repair v reconstruction for chronic PRLI
- 20 studies and 600 patients
- superior return to activity with reconstruction
- complication reconstruction: 8%
- complication repair: 15%
Outcomes reconstruction
Badhrinarayanan et al AJSM 2021
- systematic review of 17 studies and 168 patients with chronic PRLI
- 86% treated with docking technique
- recurrent instability 15%
- 93% functional ROM