

Issues
Pain and weakness
Humpback deformity / flexion deformity - alters wrist kinematics
Avascular necrosis
SNAC wrist (scaphoid nonunion advanced collapse)


Risk factors
Displaced fractures
- systematic review of scaphoid fractures displaced > 1 mm
- operative versus non operative management
- nonunion rate of displaced fractures 4X nondisplaced fractures
- nonunion rate of displaced fractures treated with cast: 18%
- nonunion rate of displaced fractures treated with surgery: 1%
Proximal pole fractures


Chong et al J Plastic Surg Hand 2022
- meta-analyis of proximal third fractures
- nonunion rates 2 - 3X higher than waist fractures
- nonoperative nonunion: 18%
- operative nonunion: 6%
Grewal et al J Hand Surg Am 2016
- 53 proximal pole scaphoid fractures
- union rate 90%
- increased risk with comminuted / cysts / translation
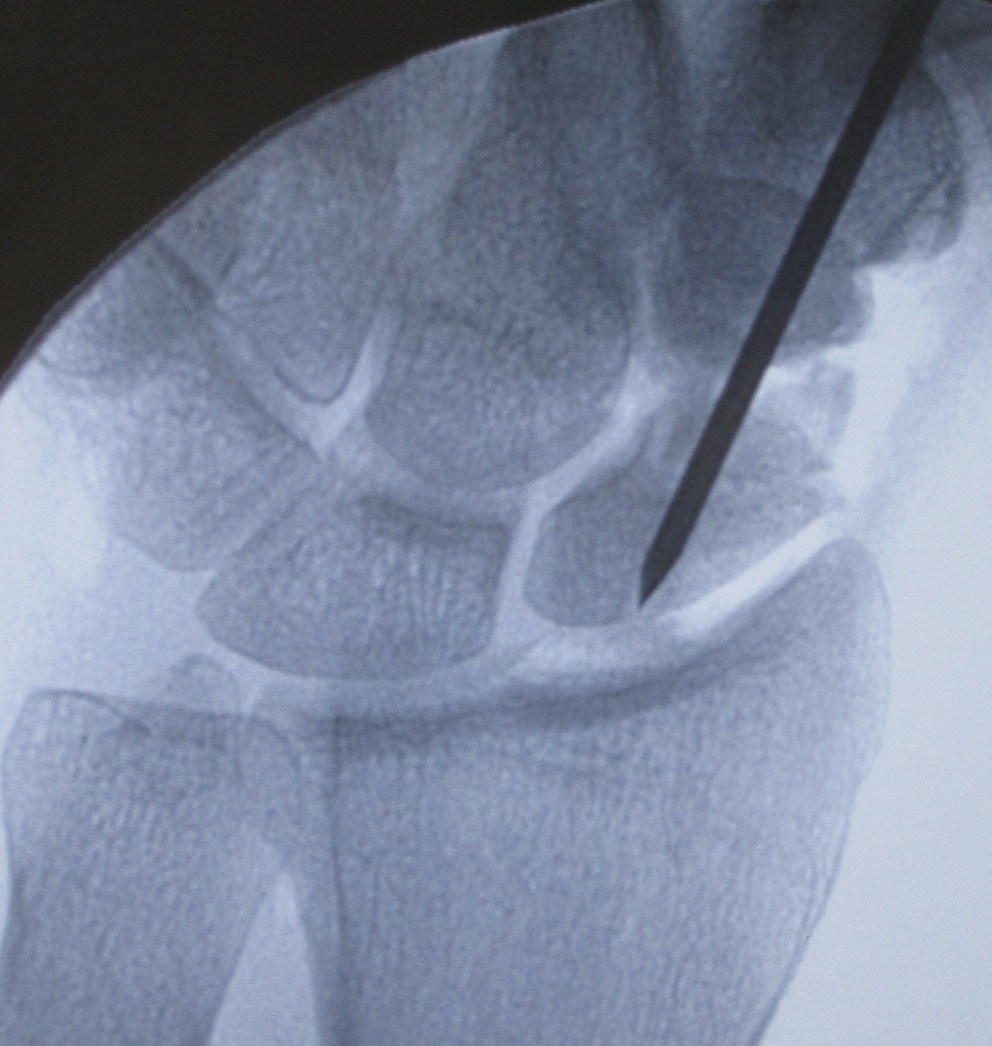
Post scaphoid ORIF

Xray



Nonunion with minimal displacement and minimal resorption

Nonunion with significant displacement and bone resorption
Proximal pole fracture with displacement and absorption
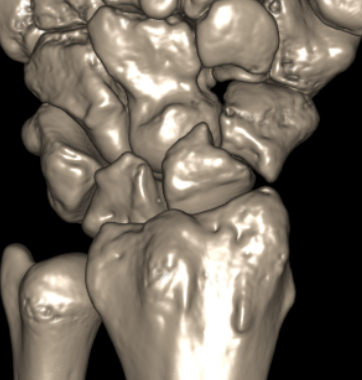
CT
Indication
- diagnose nonuion
- identify humpback deformity
- plan size and shape of bone graft

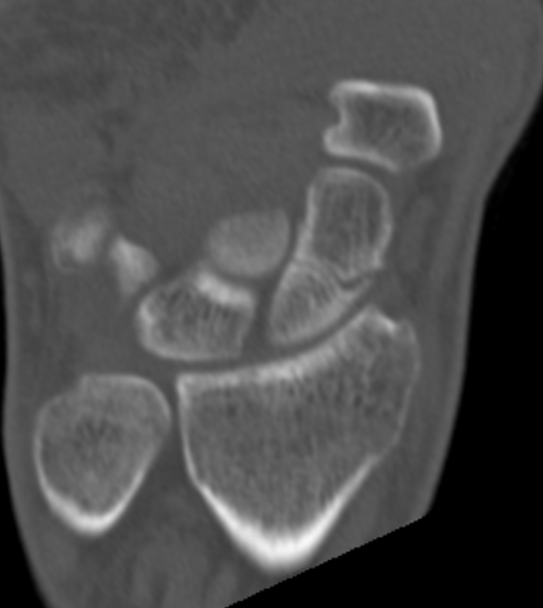
Failure of fracture to unite at 3 months on CT scan



Nonunion with flexion deformity
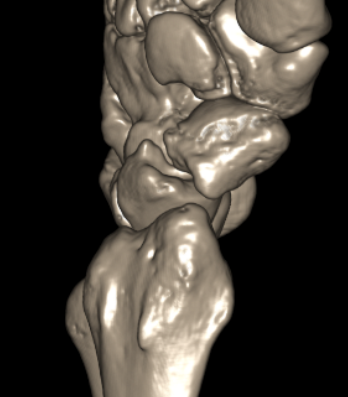
Nonunion with flexion deformity
MRI
Indication
- look for signs of AVN
- may need vascularized bone graft
Operative management
Bone graft options
Cancellous bone graft - minimal deformity
Cortico-cancellous bone graft (distal radius / iliac crest)
- correct deformity
- Russe-type inlay corticocancellous strut grafts
- Fisk wedge graft - triangular iliac crest grafts
Hamate
Vascularized bone graft




Wedge shaped corticocancellous iliac crest bone graft for deformity correction
Waist nonunion
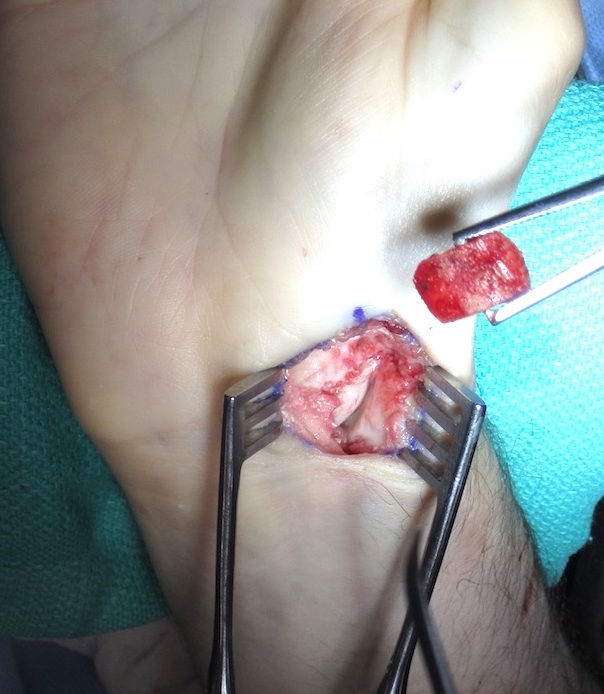

Technique
Volar approach
- clean fracture site of fibrous tissue with burrs if needed
- reduce deformity
- do not disrupt dorsal cortex
- place bone graft
- insert screws +/- plate
Results
Proximal pole nonunion



Technique
Dorsal approach

