High energy Lisfranc fracture dislocations Read more about High energy Lisfranc fracture dislocations
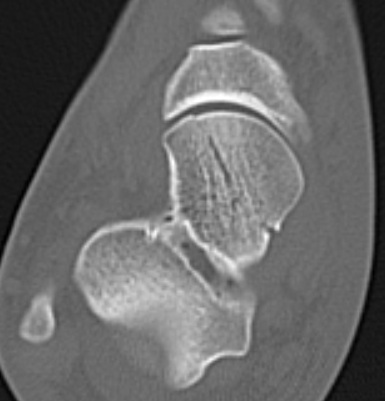
Talar head fractures Epidemiology < 10% of all talus fractures Rare and often missed Types Read more about Talar head fractures