Anatomy
Acromioclavicular Ligaments
ACJ capsule
- strongest superiorly
- provides sigificant horizontal and AP stability
- injury allows some superior migration of clavicle in Type II injury
Coracoclavicular Ligaments / CCL
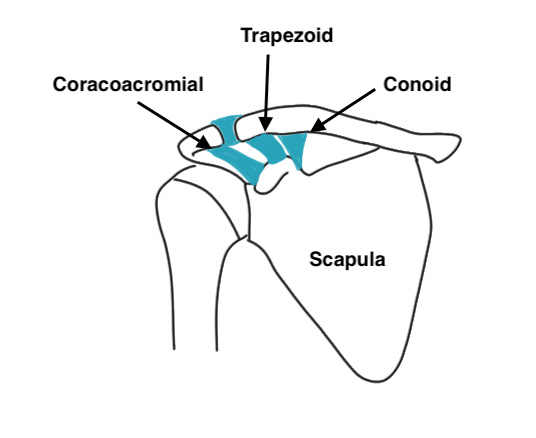
Primary restraint to superior translation
- primary suspensory ligament of upper limb
Trapezoid Ligament (anterolateral)
- anterolateral on coracoid
- almost horizontal in sagittal plane
- inserts trapezoid ridge
- primary restraint to axial compression
Conoid Ligament (posteromedial)
- postero-medial to trapezoid
- vertical inverted cone
- inserts conoid tubercle apex of posterior clavicular curve and junction lateral & medial 2/3
- primary restraint to superior and anterior translation
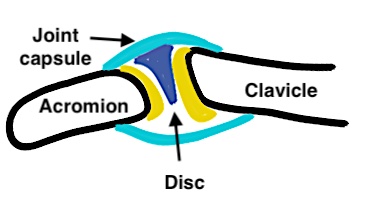
AC joint
Diarthrodial synovial joint with hyaline cartilage
- has fibrocartilage intra-articular disc
- complete or incomplete
- usually degeneration by 4th decade
Clavicle may lie superior to acromion in normal population
Motion
- rotates 5-8o with scapulo-thoracic joint motion
- rotates 40o with shoulder abduction and elevation
- motion is at rather than ACJ
Aetiology
Usually direct force onto adducted shoulder joint
- clavicle remains in normal position
- arm falls down
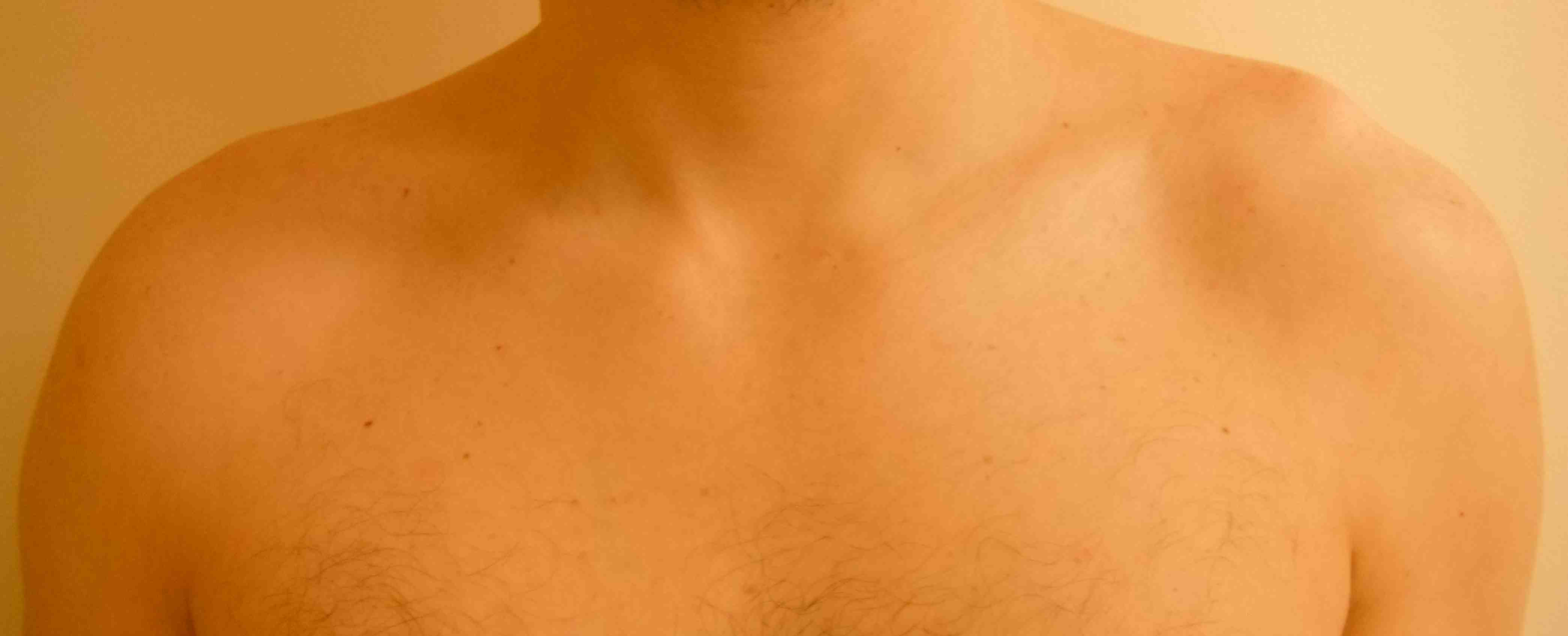
Examination
Significant injuries clinically obvious
Step at the AC joint compared with other side
Tender at AC joint




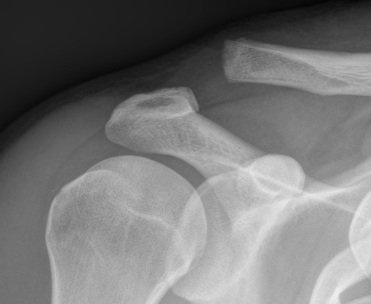
Allman grades I-III 1967 / Rockwood modified 1989 Classification
I AC ligament sprained, but CC ligaments intact (xray normal)
II AC ligament disrupted, CC ligaments sprained but intact (displaced < 100% CC distance)

III AC & CC ligaments ruptured (displaced up to 100% of CC distance)
IV AC and CC ligaments disrupted and clavicle displaced posteriorly into trapezius
- can be easily missed
- need axillary lateral



V High dislocation (100 - 300% CC distance) - disrupted trapezius & deltoid and end of clavicle subcutaneous

VI Subcoracoid dislocation

Reliability Classfication
Xray
Ringenberg et al J Should Elbow 2018
- 50 xrays reviewed by 6 upper limb trained orthopaedic surgeons
- inter-observer reliability fair (0.28)
- intra-observer reliability moderate (0.47)
- 4/50 images classified the same by all 6 surgeons
CT
- 28 cases with xray and 3D CT and 10 surgeons
- inter-observer reliability slight (0.18)
- intra-observer reliability moderate (0.57)
- addition of 3D CT did not improve reliability
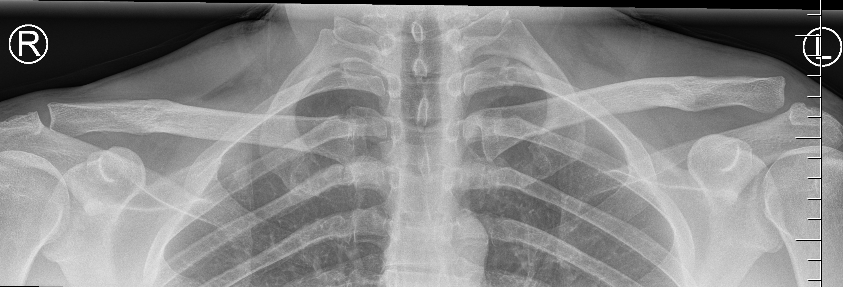
X-rays
Zanca view
- specific for AC joint
- 10o cephalad, 50% underpowered
Stress views
- hold weights in each arm
- bilateral xray
Normal
- 50% of population overriding clavicle
- 2% under riding
- 29% incongruent
- joint width 0.5-7 mm
MRI
Indications
A. Useful in professional athletes
- can distinguish between partial (type II) and complete (type III) CC ligament injuries
- allows prognosis
- can also distinguish type V
B. Incidence of concomitant GHJ injuries with ACJ dislocation
Shah et al Orthop J Sports Med 2020
- MRI of 62 patients with acute ACJ dislocation
- 77% had an intra-articular injury
- 72% SLAP tears, 24% anterior labral tears, 5% posterior labral tears, 3% supraspinatus tears
Management
Non operative
Type I and II
White et al Orthop J Sports Medicine 2020
- return to sport in 24 professional hockey players
- 3 weeks for grade 1/II
- 4 weeks for grade III
Type III / IV
Tamaoki et al Cochrane Database 2019
- acute type III dislocation
- 5 randomized and 1 quasi-randomized RCT with 357 patients
- no difference in outcomes with surgery
Canadian Orthopedic Trauma Society J Orthop Trauma 2015
- RCT of hook plate fixation for acute grade III, IV, V
- 83 patients
- no difference in outcome at 6, 12 or 24 months
- RCT suspensory fixation for acute grade III, IV versus non operative
- 60 patients
- no difference in outcome at 1 year
Operative
Indications
Type VI (subcoracoid)
Chronic debilitating Type III / IV failing non operative treatment
? Type V
Acute treatment
Options
Hook plate
Suspensory coracoclavicular fixation - open or arthroscopic


Concept
- in the acute setting, reduce and hold ACJ
- AC and CC ligaments can heal
- meta-analysis of tightrope v hook plate for acute ACJ dislocation
- 4 studies, 179 patients
- no difference in outcome
- less postoperative pain with tightrope
Issue
Should hook plate / tightrope be supplemented with reconstruction in acute setting?
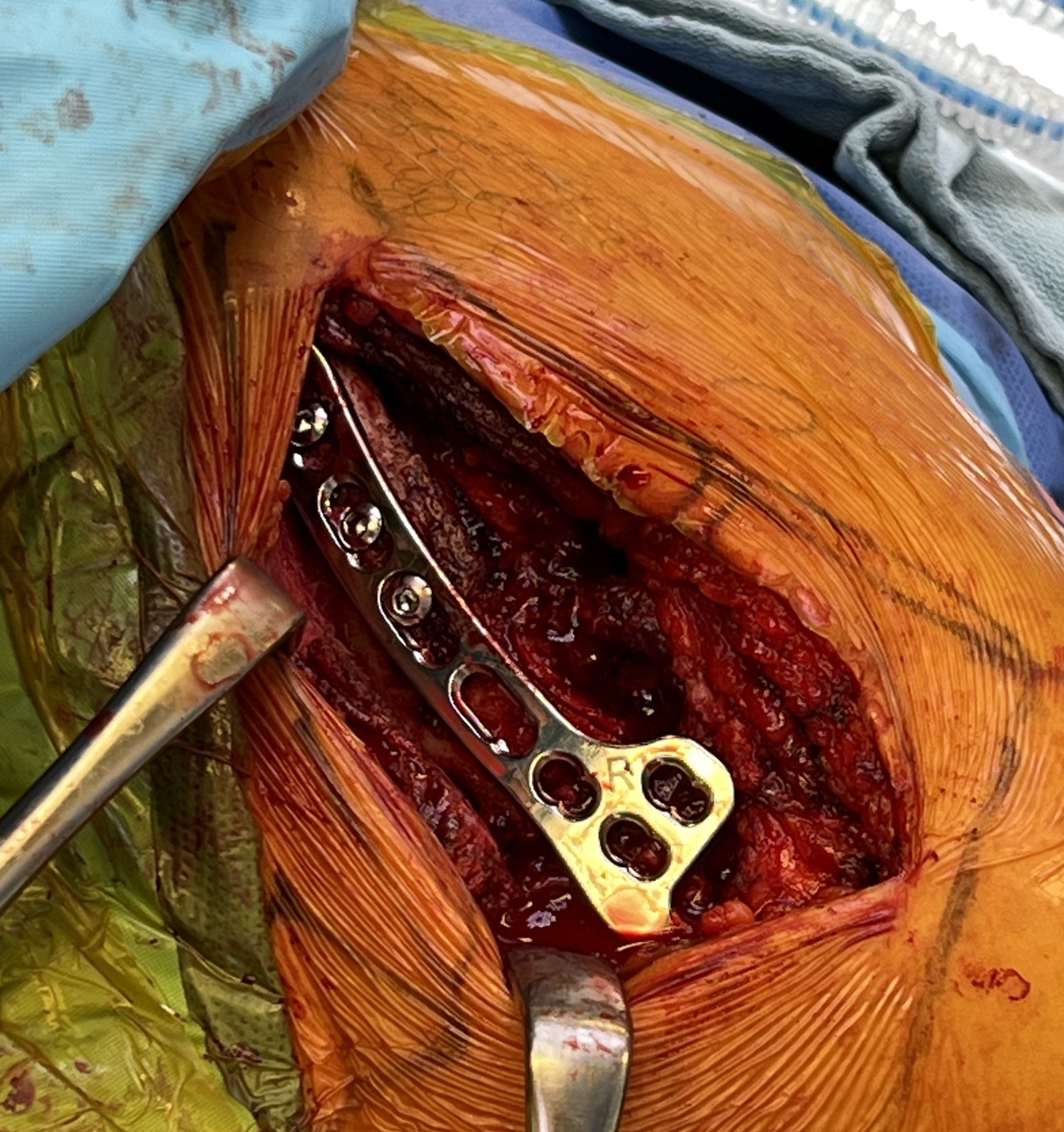
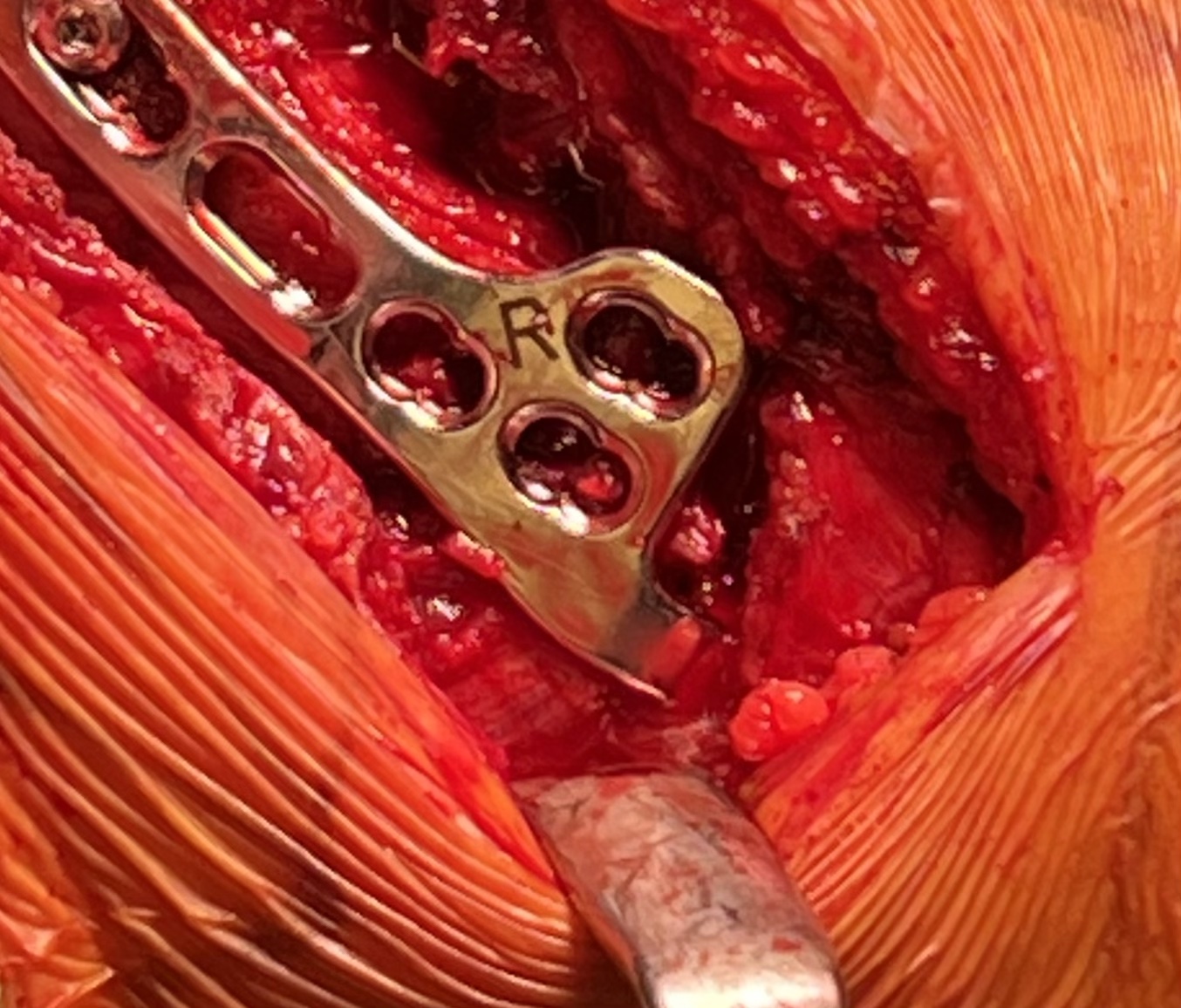
Hook plate
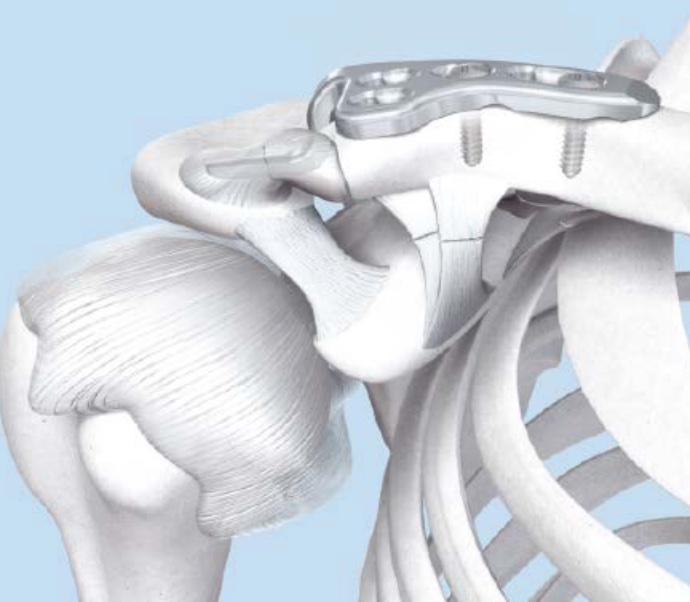
Technique
Reduction of ACJ
- hook under posterior acromion
- allows CC ligaments to heal
- need to remove plate at 4 - 6 months
Synthes technique hook plate pdf
Risks
Subacromial erosion - may be reduced by increasing the angle on the hook
Hook plate cut out through acromion - need to remove hook plate at 6 - 8 weeks
Clavicle fracture at end of plate

Results
Hemmann et al Arch Orthop Trauma Surg 2021
- 99 patients with acute ACJ dislocation treated with hook plate
- average loss of reduction of 4 mm after hook plate removal
- nearly all good to excellent outcome
- 68% full ROM post operatively
Kim et al J Orthop Trauma 2021
- 35 patients treated with hook plate
- CT showed average 5 mm of subacromial erosion (50% acromial thickness)
Issue
Do you need to reconstruction the CC ligaments in the acute setting?
- RCT of acute ACJ dislocation
- 26 hook plate and suture repair CCL
- 25 hook plate and ligament reconstruction CCL
- improved outcomes and satisfaction rates in hook plate + ligament reconstruction group
2. Suspensory fixation


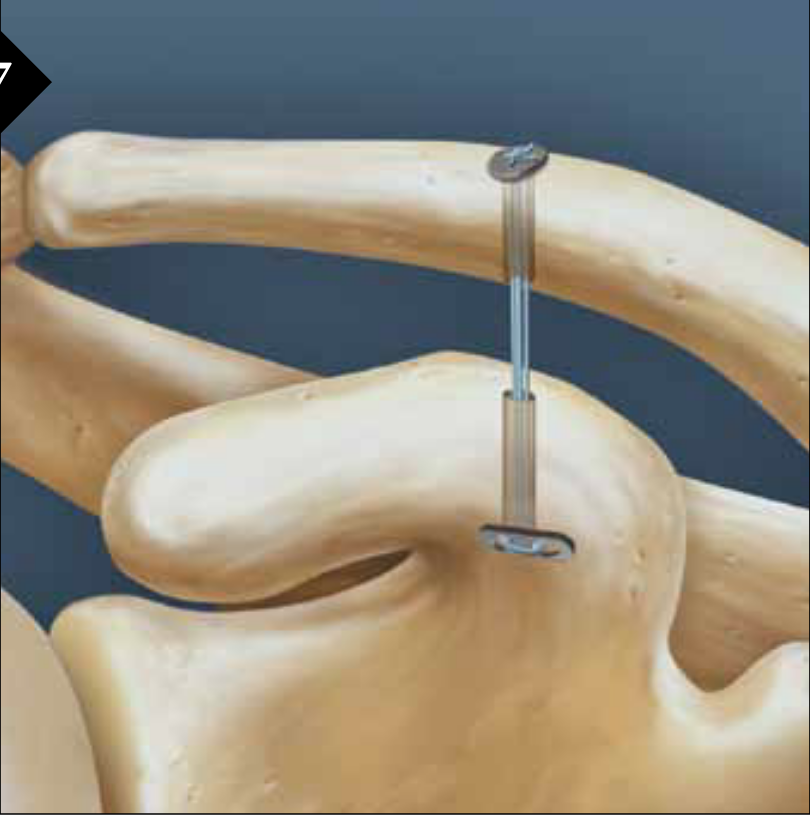
Technique
Open or arthroscopic
- drill hole in clavicle
- centred drill hole in coracoid (to avoid fracture)
- reduce AC joint
- tighten suspensory fixation
Arthrex tightrope arthroscopic technique video
Vumedi arthroscopic technique video
Risks
Coracoid fracture - must center the drill hole in the coracoid
Clavicle fracture
Failure tightrope construct
Overreduction

Failure tight rope


Over tightened tightrope
Results
- 18 patients with acute ACJ dislocation treated with Tightrope
- 1 case clavicle fracture
- 3 cases of clavicle or coracoid button failure
- 3 cases of clavicular bony erosion
Chronic ACJ Reconstruction
Options
1. Coracoclavicular ligament reconstruction
- anatomic or non anatomic
- autograft or allograft
- open or arthroscopic
- may be augmented with hook plate or suspensory fixation
2. Weaver Dunn
Historical options
Excision distal clavicle
- poor results
- convert long high riding clavicle to short high riding clavicle
Phimister technique
- K wires across AC joint
- suture repair AC and CC ligaments
- risk of K wire migration
Bosworth screw
- screw from clavicle to coracoid
- risk of pullout
- needs to be removed
1. CC ligament reconstruction
Anatomic technique
- pass allograft or autograft around coracoid
- pass through two clavicle drill holes
- secure with screws
- looking to improve AP and vertical stability
- risks clavicle fracture


Non anatomic technique
- pass allograft or autograft around coracoid
- around clavicle
Vumedi open anatomic technique video
Vumedi arthroscopic anatomic technique video
Supplement
- fixation such as hook plate or suspensory fixation
Results
Millett et al Arthroscopy 2015
- 31 shoulders anatomical reconstruction tendon graft
- 2/31 clavicle fractures
- 2/31 graft rupture attenuation
- 7/31 (22%) required secondary surgical procedure
2. Weaver Dunn Reconstruction
Concept
Reconstruction of CC ligament with coraco-acromial ligament (CAL)
Technique
- 45o beach chair
- sabre incision over ACJ
- split deltoid fascia transversely along the clavicle and onto acromion
- expose distal end of clavicle and resect small amount with microsagittal saw
- expose anterior aspect of acromion but identify and preserve CA ligament
- take off anterior 5mm of acromion with CA ligament attached
- carefully peel CAL off the underlying subscapularis
- CA ligament left attached to coracoid
- transferred from acromion to clavicle end
- intra-osseous suture repair through clavicle drill holes
- consider supplement fixation with hook plate / suspensory fixation
Type VI / Subcoracoid dislocation

Rare / can be missed
Risk of neurovascular injury / high velocity injury / associated with multi-traumas
Requires open reduction and fixation
- will have to release soft tissue off coracoid if not already avulsed
- i.e. pectoralis minor / coracoacromial ligament
- attempt to reduce with lateral traction of arm
- may need to release conjoint / perform coracoid osteotomy
- stabilize as needed
Subcoracoid dislocation case report