Dual mobility


Stryker dual mobility
Concept
Stryker dual mobility
Prevent contractures
Prevent dislocations
Improve walking
Provide stable and painless sitting
Allow perineal care
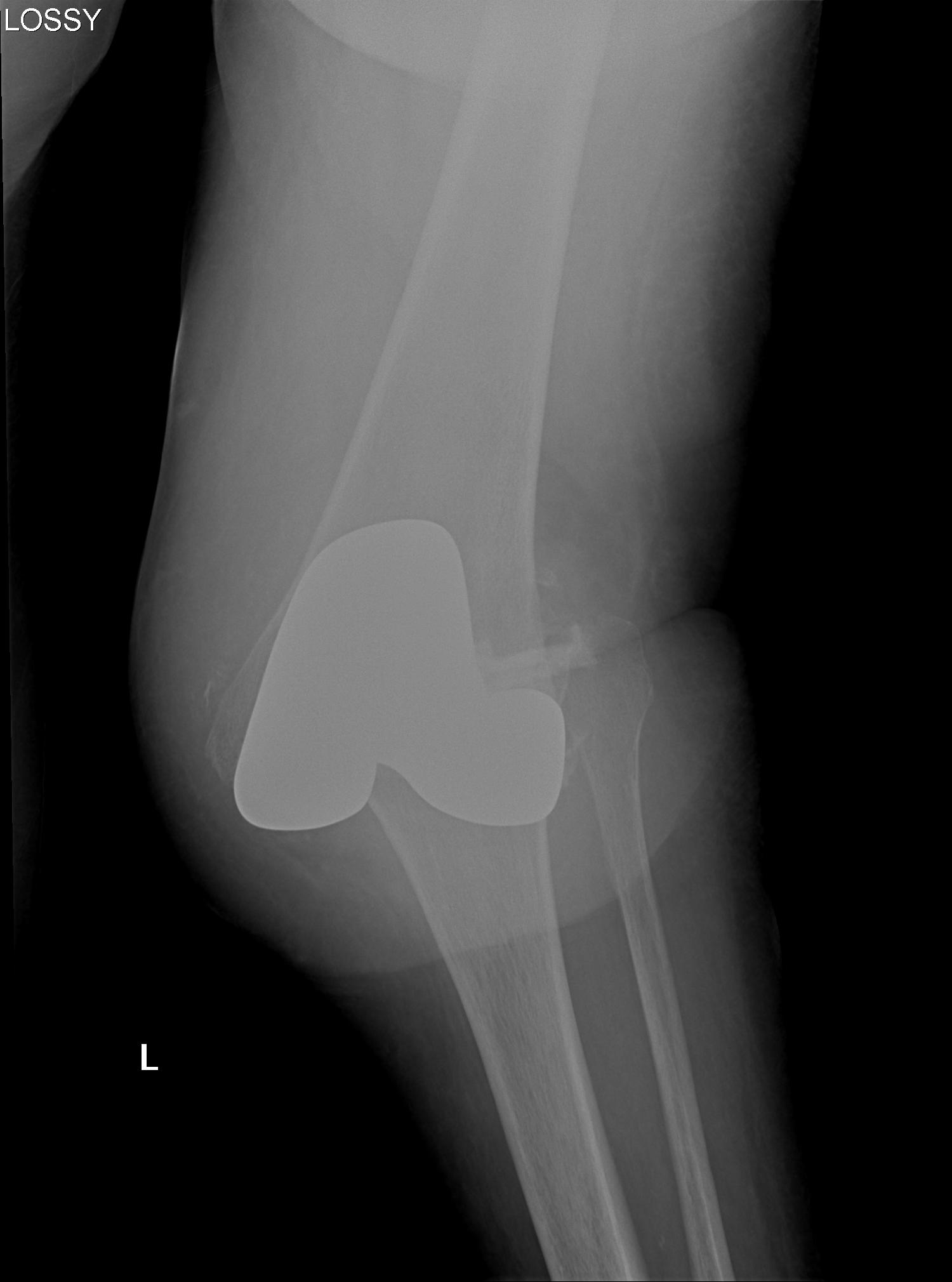
Hip Dislocation
Adductor contractures
Flexion contractures
In-toeing
Windswept hips
Accepted that a dislocated hip in CP is painful
Deadly & rare
- usually post mortem
More common in children due to
- immature joints
- larger head to body ratio
- relative ligamentous laxity
High velocity trauma
- MVA
Mechanism
- hyperextension, distraction & rotation
Pure ligament injury usually
Facet joint dislocations secondary flexion distraction injury
10%
1. Unifacet subluxation - interspinous process widening
2. Unifacet dislocation - 25% anterolisthesis
3. Bifacet dislocation - 50% anterolisthesis
4. Complete vertebral translation - 100% anterolisthesis
1. AP Instability
2. Varus Valgus Instability
3. Global Instability
4. Frank Dislocation


1. Direct lateral blow to patella
- usually with knee partly flexed and quadriceps relaxed
2. Indirect low energy injury
Repeated dislocation of patella with minimal trauma
- 15-20% of paediatric acute patella dislocations
- more common girls
- often bilateral
Dislocation occurs unexpectedly when quadriceps contracted with knee in flexion
Young men in 20's and 30's
High energy injuries
- fall from heights
- MVA
Injury progresses from radial to ulna
- usually disruption proximal row either side of lunate
1. Capitate usually displaces dorsally initially
- volar lunate dislocation is end stage
Avoid by
- careful reaming and drilling osteoporotic bone
Management
1. Rotate metaglene
- use locking screws to stabilise glenoid
2. PA screws
- cannulated 4.0 mm screws
- inserted percutaneously from posterior
Great deal of dead space is created
- always use a drain
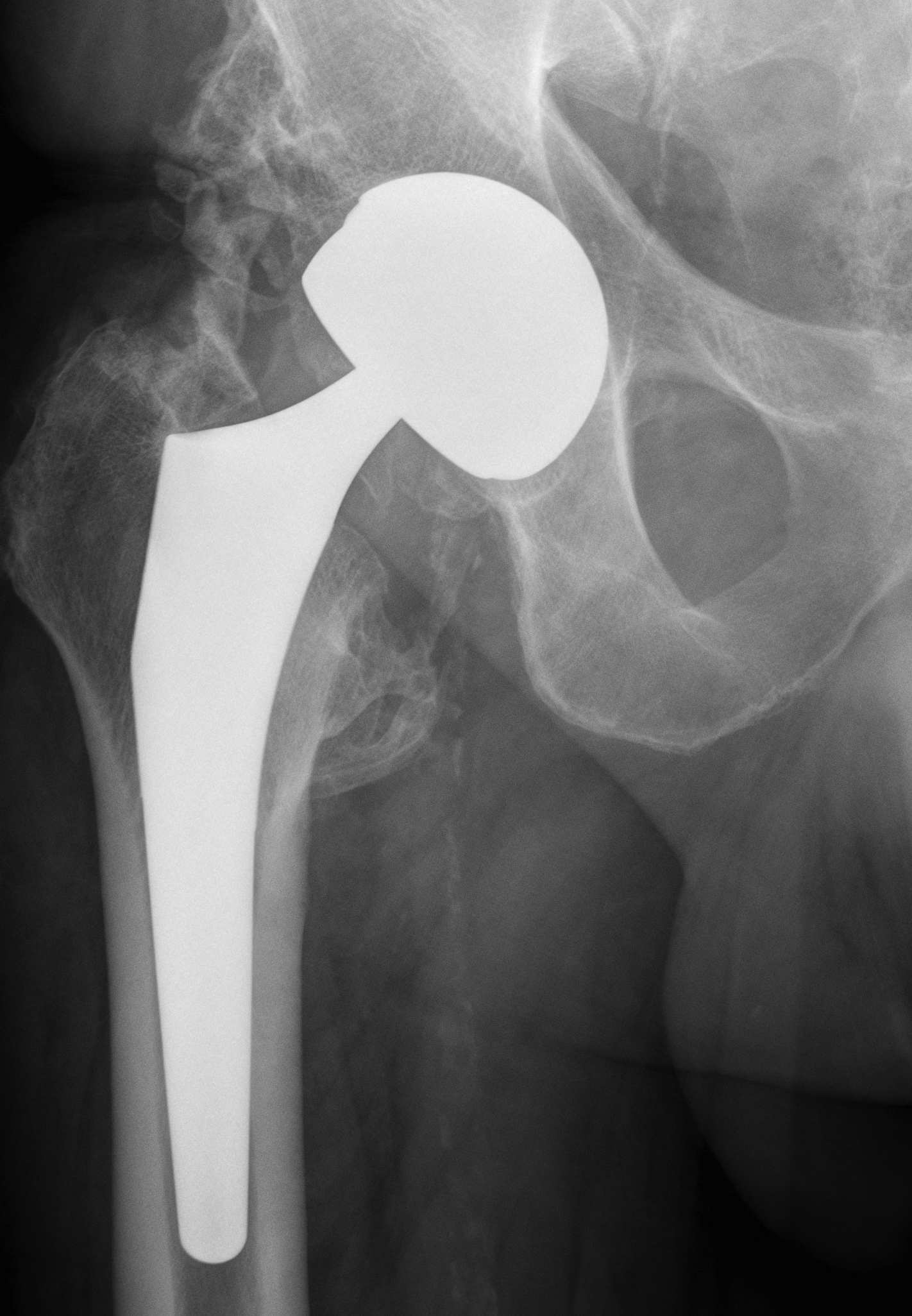
Wear
Stability
Normal feel of hip
Increased ROM
Large head
- increase volumetric wear
- less penetrative / linear wear
Small head
- increased linear wear
- decreased volumetric wear