classification
Fragility pelvic fractures

Definition
Fracture of the pelvis caused by a low energy fall
Usually secondary to osteoporosis
Bleeding
Incidence of bleeding low unless on anticoagulation
Fracture pattern
Lateral compression injury
- pubic rami fracture
Background
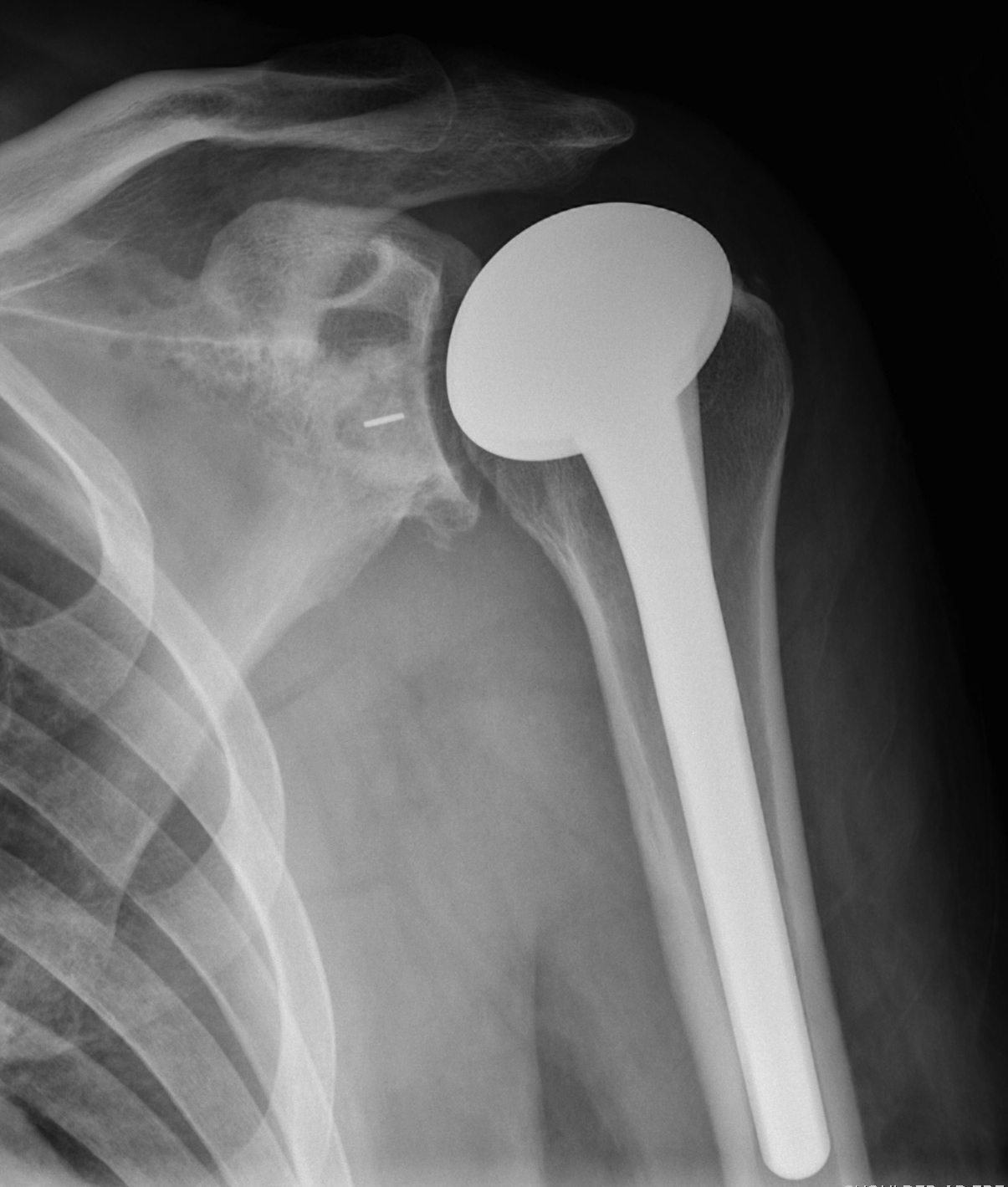
Indications
RA
OA
AVN
Contra-indications
Infection
Charcot
Paralysis of deltoid
Torn rotator cuff
Insufficient glenoid bone stock
Hangman's / C2 Fracture
Definition
Bilateral Pars Fracture C2
- traumatic axis spondylolisthesis
NHx
Neurological injury uncommon
- fragments separate and decompress
Different to judicial hanging where spinal cord is severed
Xray
Burst Fractures
Definition
Burst fractures
- injury to anterior and middle columns +/- posterior column
Mechanism
Vertical compression
Epidemiology
10% cervical fractures
Most commonly C5/6
Pathology
Anterior & middle columns fail
- if severe, posterior ligament complex fails
Injury
Classification Leffert "OCRO"
I Open
II Closed
A Supraclavicular
- Preganglionic / Avulsion of Roots
- Postganglionic / Rupture of Trunks
B Infraclavicular
- cords & branches
C. Post anaesthetic
III Radiation / Other
Tumour
Background
Aetiology
Intrinsic
- inflammatory
- degenerative
Extrinsic
- traumatic
- spur
Epidemiology
F > 40
Associations 60% of cases
- hypertension
- diabetes
- obese
- trauma
- prior surgery
- steroids
Background
Anatomy
3 facets
1. Posterior facet (STJ)
2. Middle facet (sustenaculum tali)
3. Anterior facet (on distal medial aspect)
Anterior process
- forms calcaneocuboid (CCJ) articulation
Thalamic portion
- under lateral process talus
Tuberosities
Posterior tuberosity
- posterior process / T Achilles attachment
Accessory Navicular
Incidence
1 - 2 %
Anatomy
Medial Aspect of foot
- proximal to navicular
- part of T posterior tendon
Usually will fuse with navicular (50%)
Issues
1. Probably not a cause of flat foot
- excising accessory navicular / rerouting / reattaching tibialis posterior
- will not help pes planus
2. Pain
- may fracture
Management Bone Defects
AORI / Andersen Orthopedic Research Institute
T Tibial F Femoral
1. Contained Metaphyseal Defect
2. Damaged Metaphyseal
A. One Condyle
B. Both Condyles
3. Deficient Metaphysis +/- collaterals +/- extensor mechanism
1. Contained Metaphyseal defect