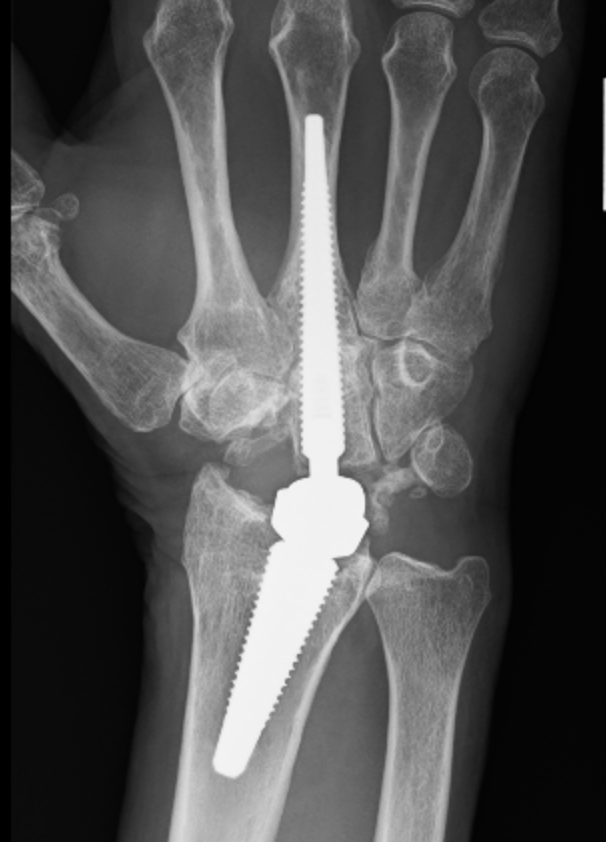
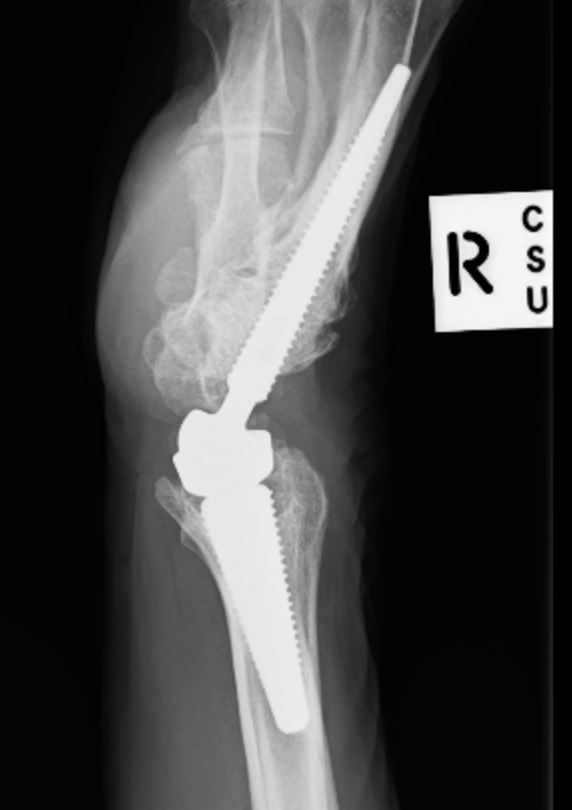
Wrist arthroplasty
Indications
Theory
- want to traverse one muscle / one compartment
- keep away from NV bundle
- as a rule perform open biopsy through compartment the tumour is in
- this is the compartment that will require surgical removal in wide excision
- direct approach without going through muscle if possible i.e. tibia, distal ulna
Thigh
Diaphyseal Aclasis / Multiple Osteochondromas
Heritable skeletal dysplasia
AD with variable penetrance (96%)
Incidence of malignant transformation much higher
- 10% overall
- 1 % / year
Chondrosarcoma (CS) > Osteosarcoma (OS)
Upper limb surgery is mainly in spastic hemiplegia
- many of the CP' s have sensory neglect for affected limbs
- won't use limb post surgery anyway
Surgical indications
- a reasonable level of IQ (>70)
- spastic not athetoid
- voluntary grasp and release
Scaphoid non union advanced collapse
Xray / CT
- non union of scaphoid
- radio-scaphoid OA


2 groups
1. Elderly
- low velocity injury
- osteoporotic
- need to start bisphosphonates
2. Young patients
- high velocity injury
Distal Radius Angles
- radial volar tilt 11°
- radial inclination 22°
- radius is 11 mm longer than ulna
- ulna variance 2mm positive on average

Extremely common
- 90% by 10 years have wrist problems
Landsmeer 1961
- treat wrist at same time as treat fingers or will recur
Frequently combine procedures
- synovectomy
- tendon transfer
- ulna procedure