Anatomy
Acromioclavicular Ligaments
ACJ capsule
- strongest superiorly
- provides sigificant horizontal and AP stability
- injury allows some superior migration of clavicle in Type II injury
Coracoclavicular Ligaments / CCL
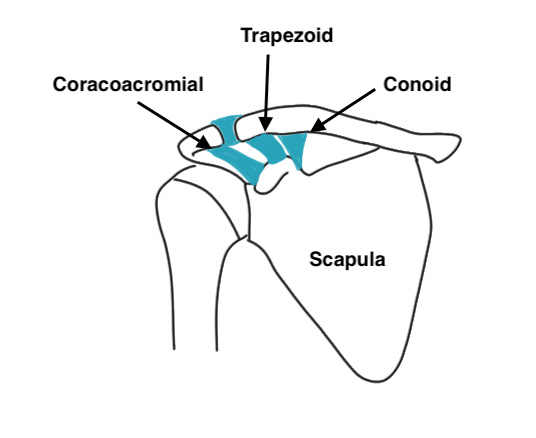
Primary restraint to superior translation
- primary suspensory ligament of upper limb
Trapezoid Ligament (anterolateral)
- anterolateral on coracoid
- almost horizontal in sagittal plane
- inserts trapezoid ridge
- primary restraint to axial compression
Conoid Ligament (posteromedial)
- postero-medial to trapezoid
- vertical inverted cone
- inserts conoid tubercle apex of posterior clavicular curve and junction lateral & medial 2/3
- primary restraint to superior and anterior translation
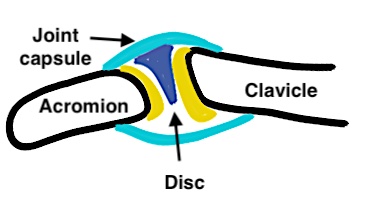
AC joint
Diarthrodial synovial joint with hyaline cartilage
- has fibrocartilage intra-articular disc
- complete or incomplete
- usually degeneration by 4th decade
Clavicle may lie superior to acromion in normal population
Motion
- rotates 5-8o with scapulo-thoracic joint motion
- rotates 40o with shoulder abduction and elevation
- motion is at rather than ACJ
Aetiology
Usually direct force onto adducted shoulder joint
- clavicle remains in normal position
- arm falls down
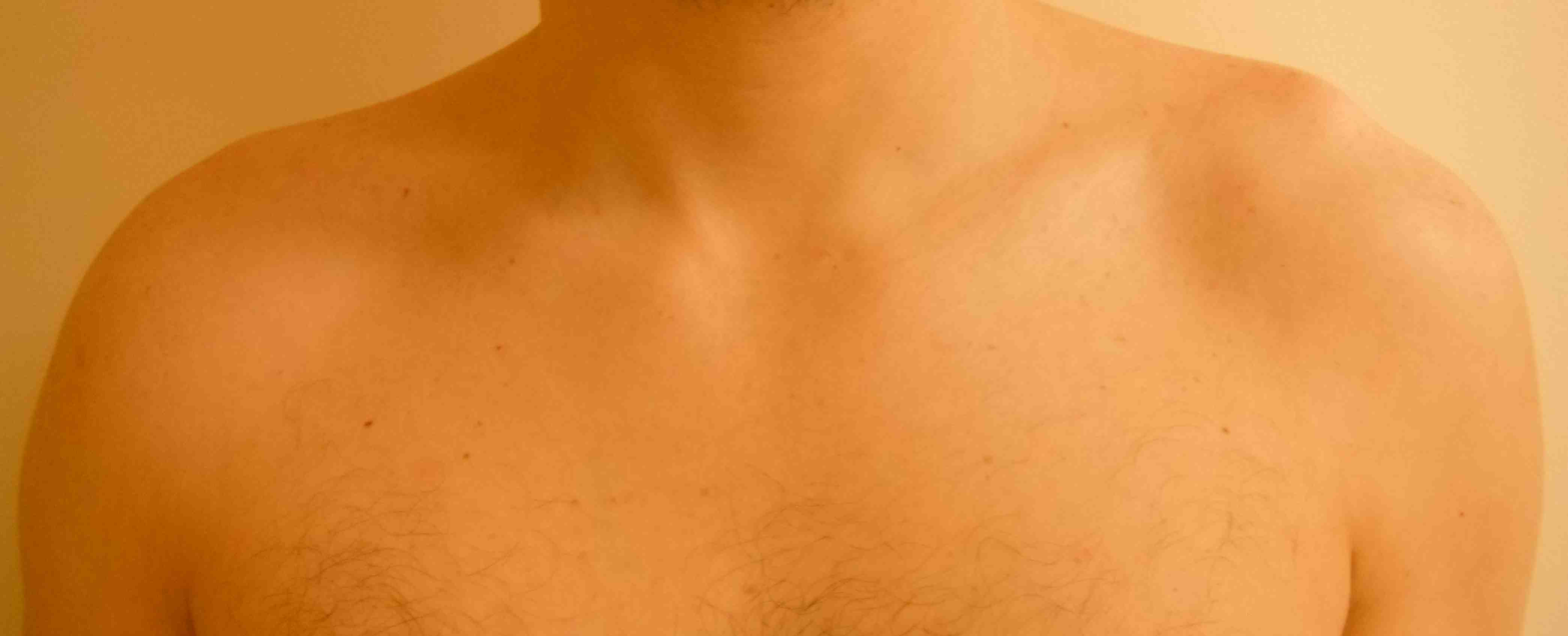
Examination
Significant injuries clinically obvious
Step at the AC joint compared with other side
Tender at AC joint




Allman grades I-III 1967 / Rockwood modified 1989 Classification
I AC ligament sprained, but CC ligaments intact (xray normal)
II AC ligament disrupted, CC ligaments sprained but intact (displaced < 100% CC distance)

III AC & CC ligaments ruptured (displaced up to 100% of CC distance)
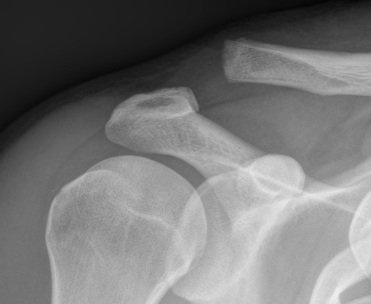
IV AC and CC ligaments disrupted and clavicle displaced posteriorly into trapezius
- can be easily missed
- need axillary lateral



V High dislocation (100 - 300% CC distance) - disrupted trapezius & deltoid and end of clavicle subcutaneous

VI Subcoracoid dislocation

Reliability Classfication
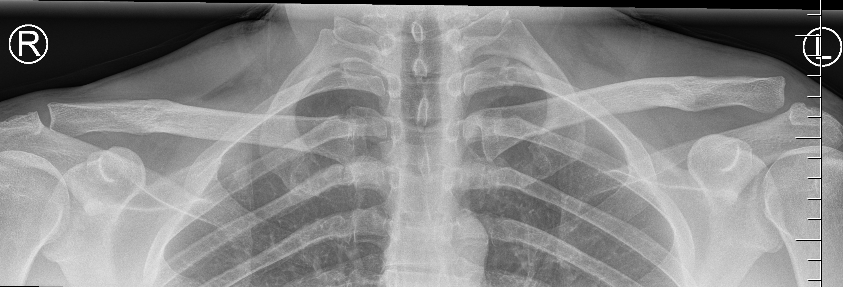
Xray
Ringenberg et al J Should Elbow 2018
- 50 xrays reviewed by 6 upper limb trained orthopaedic surgeons
- inter-observer reliability fair (0.28)
- intra-observer reliability moderate (0.47)
- 4/50 images classified the same by all 6 surgeons
CT
- 28 cases with xray and 3D CT and 10 surgeons
- inter-observer reliability slight (0.18)
- intra-observer reliability moderate (0.57)
- addition of 3D CT did not improve reliability
X-rays
Zanca view
- specific for AC joint
- 10o cephalad, 50% underpowered
Stress views
- hold weights in each arm
- bilateral xray
Normal
- 50% of population overriding clavicle
- 2% under riding
- 29% incongruent
- joint width 0.5-7 mm
MRI
Indications
A. Useful in professional athletes
- can distinguish between partial (type II) and complete (type III) CC ligament injuries
- allows prognosis
- can also distinguish type V
B. Incidence of concomitant GHJ injuries with ACJ dislocation
Shah et al Orthop J Sports Med 2020
- MRI of 62 patients with acute ACJ dislocation
- 77% had an intra-articular injury
- 72% SLAP tears, 24% anterior labral tears, 5% posterior labral tears, 3% supraspinatus tears
Management
Non operative
Type I and II
White et al Orthop J Sports Medicine 2020
- return to sport in 24 professional hockey players
- 3 weeks for grade 1/II
- 4 weeks for grade III
Type III / IV
Tamaoki et al Cochrane Database 2019
- acute type III dislocation
- 5 randomized and 1 quasi-randomized RCT with 357 patients
- no difference in outcomes with surgery
Canadian Orthopedic Trauma Society J Orthop Trauma 2015
- RCT of hook plate fixation for acute grade III, IV, V
- 83 patients
- no difference in outcome at 6, 12 or 24 months
- RCT suspensory fixation for acute grade III, IV versus non operative
- 60 patients
- no difference in outcome at 1 year
Operative
Indications
Type VI (subcoracoid)
Chronic debilitating Type III / IV failing non operative treatment
? Type V
Acute treatment
Options
Hook plate
Suspensory coracoclavicular fixation - open or arthroscopic


Concept
- in the acute setting, reduce and hold ACJ
- AC and CC ligaments can heal
- meta-analysis of tightrope v hook plate for acute ACJ dislocation
- 4 studies, 179 patients
- no difference in outcome
- less postoperative pain with tightrope
Issue
Should hook plate / tightrope be supplemented with reconstruction in acute setting?
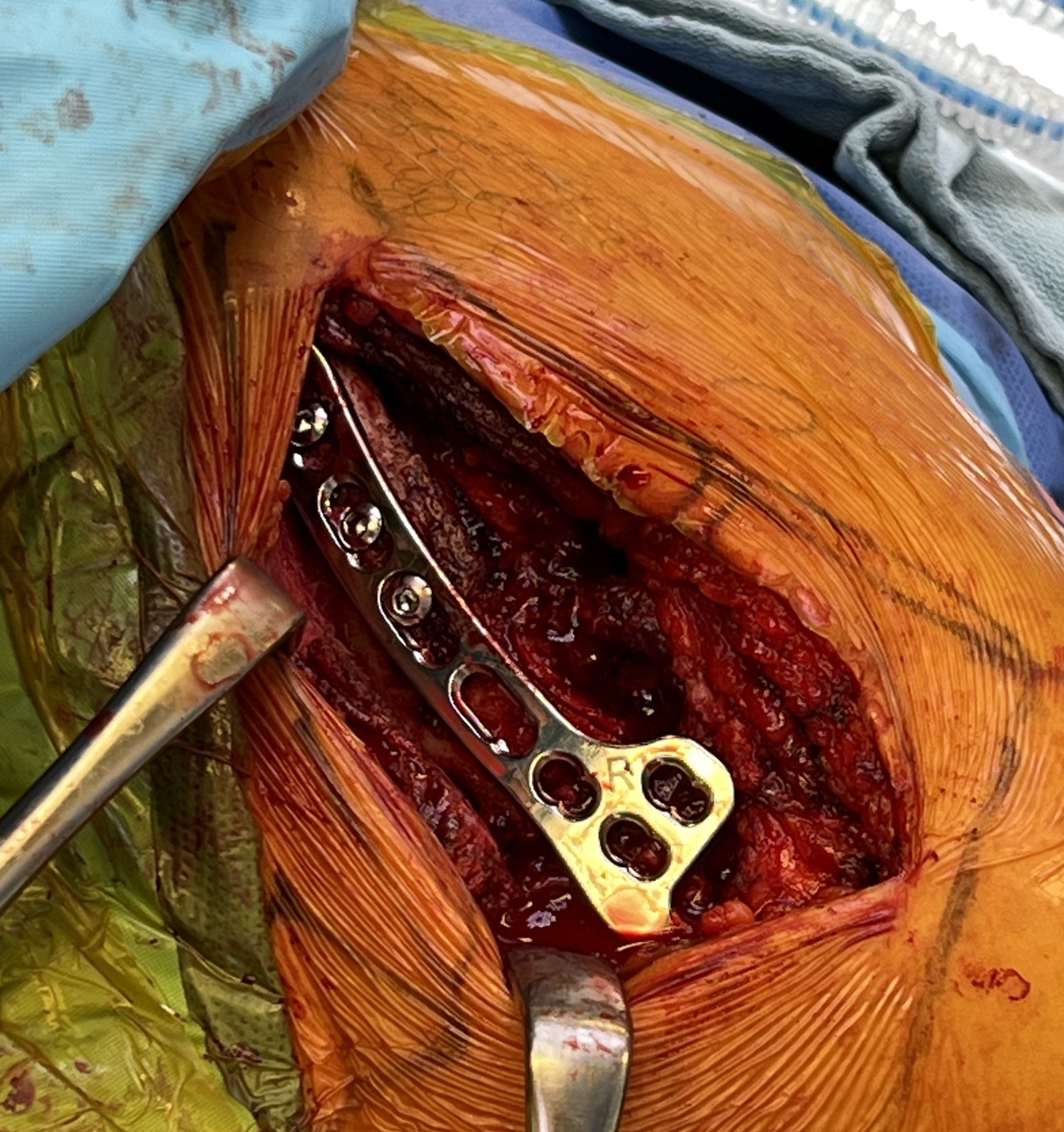
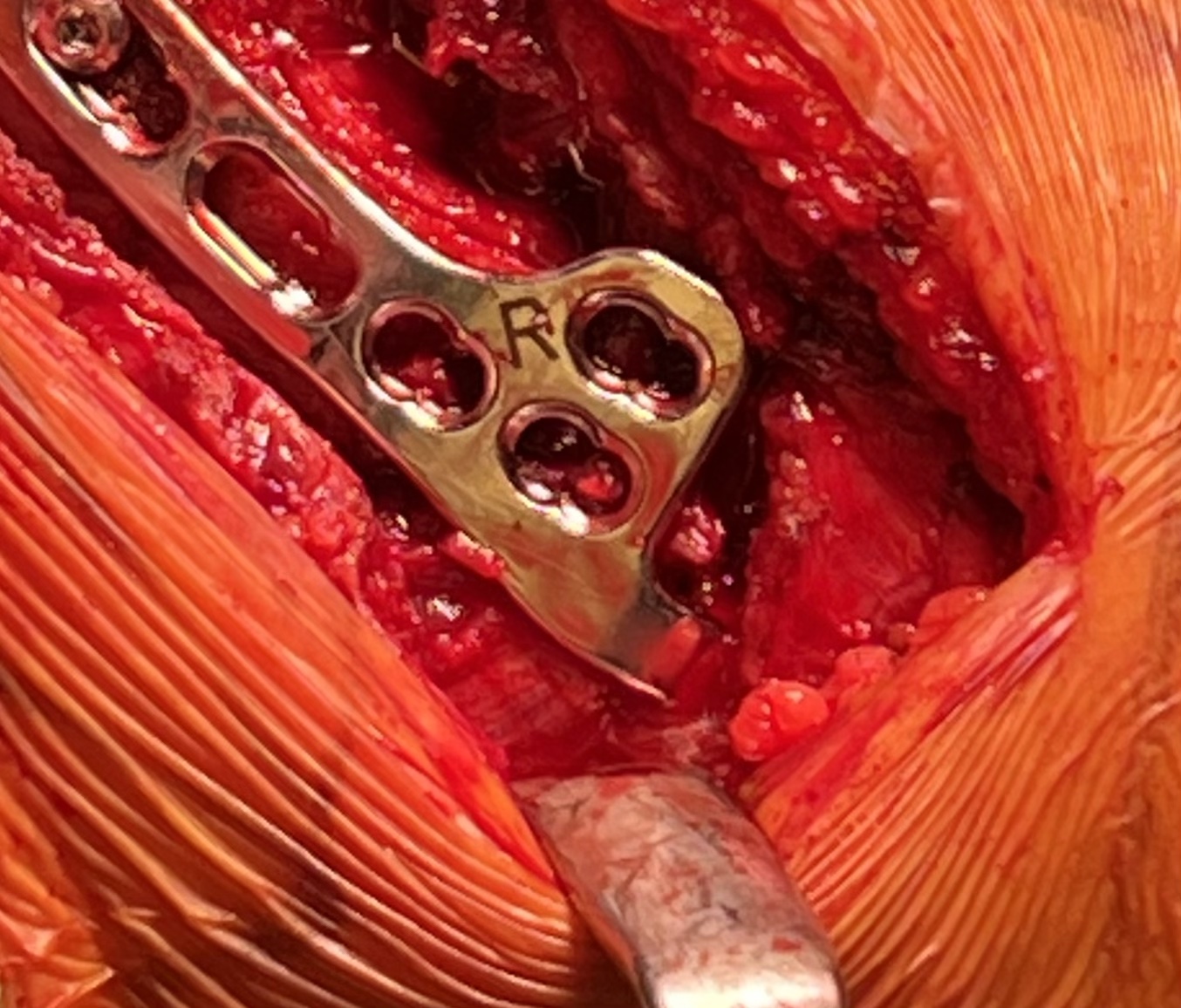
Hook plate
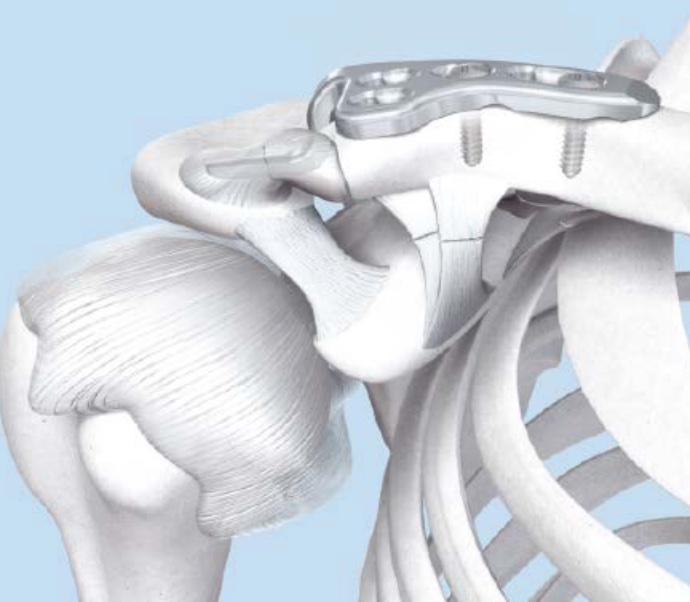
Technique
Reduction of ACJ
- hook under posterior acromion
- allows CC ligaments to heal
- need to remove plate at 4 - 6 months
Synthes technique hook plate pdf
Risks
Subacromial erosion - may be reduced by increasing the angle on the hook
Hook plate cut out through acromion - need to remove hook plate at 6 - 8 weeks
Clavicle fracture at end of plate

Results
Hemmann et al Arch Orthop Trauma Surg 2021
- 99 patients with acute ACJ dislocation treated with hook plate
- average loss of reduction of 4 mm after hook plate removal
- nearly all good to excellent outcome
- 68% full ROM post operatively
Kim et al J Orthop Trauma 2021
- 35 patients treated with hook plate
- CT showed average 5 mm of subacromial erosion (50% acromial thickness)
Issue
Do you need to reconstruction the CC ligaments in the acute setting?
- RCT of acute ACJ dislocation
- 26 hook plate and suture repair CCL
- 25 hook plate and ligament reconstruction CCL
- improved outcomes and satisfaction rates in hook plate + ligament reconstruction group
2. Suspensory fixation


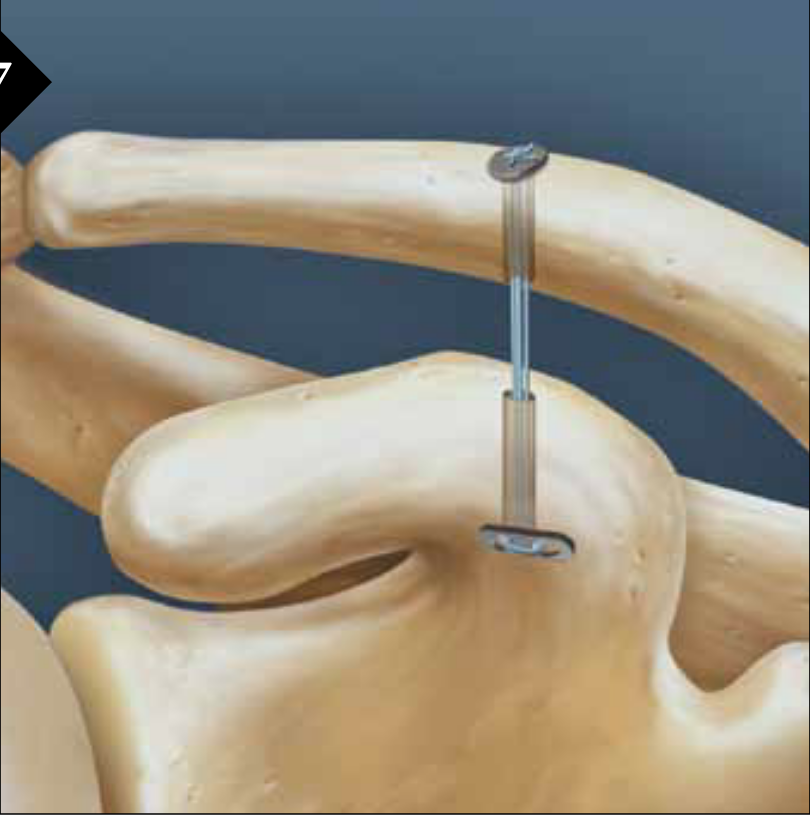
Technique
Open or arthroscopic
- drill hole in clavicle
- centred drill hole in coracoid (to avoid fracture)
- reduce AC joint
- tighten suspensory fixation
Vumedi open technique with CA ligament video
Arthrex tightrope arthroscopic technique video
Vumedi arthroscopic technique video
Risks
Coracoid fracture - must center the drill hole in the coracoid
Clavicle fracture
Failure tightrope construct
Overreduction

Failure tight rope


Over tightened tightrope
Results
- 18 patients with acute ACJ dislocation treated with Tightrope
- 1 case clavicle fracture
- 3 cases of clavicle or coracoid button failure
- 3 cases of clavicular bony erosion
Chronic ACJ Reconstruction
Options
1. Coracoclavicular ligament reconstruction
- anatomic or non anatomic
- autograft or allograft
- open or arthroscopic
- may be augmented with hook plate or suspensory fixation
2. Weaver Dunn
Historical options
Excision distal clavicle
- poor results
- convert long high riding clavicle to short high riding clavicle
Phimister technique
- K wires across AC joint
- suture repair AC and CC ligaments
- risk of K wire migration
Bosworth screw
- screw from clavicle to coracoid
- risk of pullout
- needs to be removed
CC ligament reconstruction anatomic technique
Anatomic technique
- pass allograft or autograft around coracoid
- pass through two clavicle drill holes
- secure with screws
- looking to improve AP and vertical stability
- risks clavicle fracture


Results
Millett et al Arthroscopy 2015
- 31 shoulders anatomical reconstruction tendon graft
- 2/31 clavicle fractures
- 2/31 graft rupture attenuation
- 7/31 (22%) required secondary surgical procedure
CC ligament reconstruction non anatomic technique
Pass allograft or autograft around coracoid and clavicle
- supplementary fixation
- hook plate / suspensory fixation
Vumedi open anatomic technique video
Vumedi arthroscopic anatomic technique video


ACJ reconstruction with Arthrex Dogbone followed by allograft
2. Weaver Dunn Reconstruction
Concept
Reconstruction of CC ligament with coraco-acromial ligament (CAL)
Technique
- 45o beach chair
- sabre incision over ACJ
- split deltoid fascia transversely along the clavicle and onto acromion
- expose distal end of clavicle and resect small amount with microsagittal saw
- expose anterior aspect of acromion but identify and preserve CA ligament
- take off anterior 5mm of acromion with CA ligament attached
- carefully peel CAL off the underlying subscapularis
- CA ligament left attached to coracoid
- transferred from acromion to clavicle end
- intra-osseous suture repair through clavicle drill holes
- consider supplement fixation with hook plate / suspensory fixation
Type VI / Subcoracoid dislocation

Rare / can be missed
Risk of neurovascular injury / high velocity injury / associated with multi-traumas
Requires open reduction and fixation
- will have to release soft tissue off coracoid if not already avulsed
- i.e. pectoralis minor / coracoacromial ligament
- attempt to reduce with lateral traction of arm
- may need to release conjoint / perform coracoid osteotomy
- stabilize as needed
Subcoracoid dislocation case report