


Incidence
Leg length discrepancy (LLD) < 1 cm seen in 90% of population
Etiology
Functional LLD
- LLD caused by contracture
- knee and hip fixed flexion deformity (sagittal plane)
- hip adduction / abduction contractures, knee varus / valgus (coronal plane)
Structural LLD
- true LLD
- short femur / tibia / hip
- multiple causes
| Hemihypertrophy / atrophy | Growth plate arrest | Hip | Congenital femoral deficiency | Leg |
|---|---|---|---|---|
|
Idiopathic Klippel-Trenaunay-Weber syndrome Proteus syndrome Beckwith-Weiderman syndrome Russel-Silver syndrome (atrophy) |
Trauma Infection Radiotherapy Tumour |
PFFD Coxa vara SUFE DDH Perthe's Infection |
Fibula hemimelia Tibial hemimelia Bowing |
Congenitally short femur Short femur from distal femur growth arrest
Issues
Short leg gait / increased energy expenditure
Khamis et al Gait Posture 2017
- systematic review of effect of LLD and gait
- LLD > 1 cm affected gait
Compensatory scoliosis
Hamada et al Strategies Trauma Limb Recon 2022
- 113 patients with LLD
- LLD 2 cm correlates with Cobb angle of 10 degrees
Low back / hip / knee pain
Gordon et al J Pediatr Orthop 2019
- systematic review
- some evidence of low back pain / hip / knee pathology with LLD > 2 cm

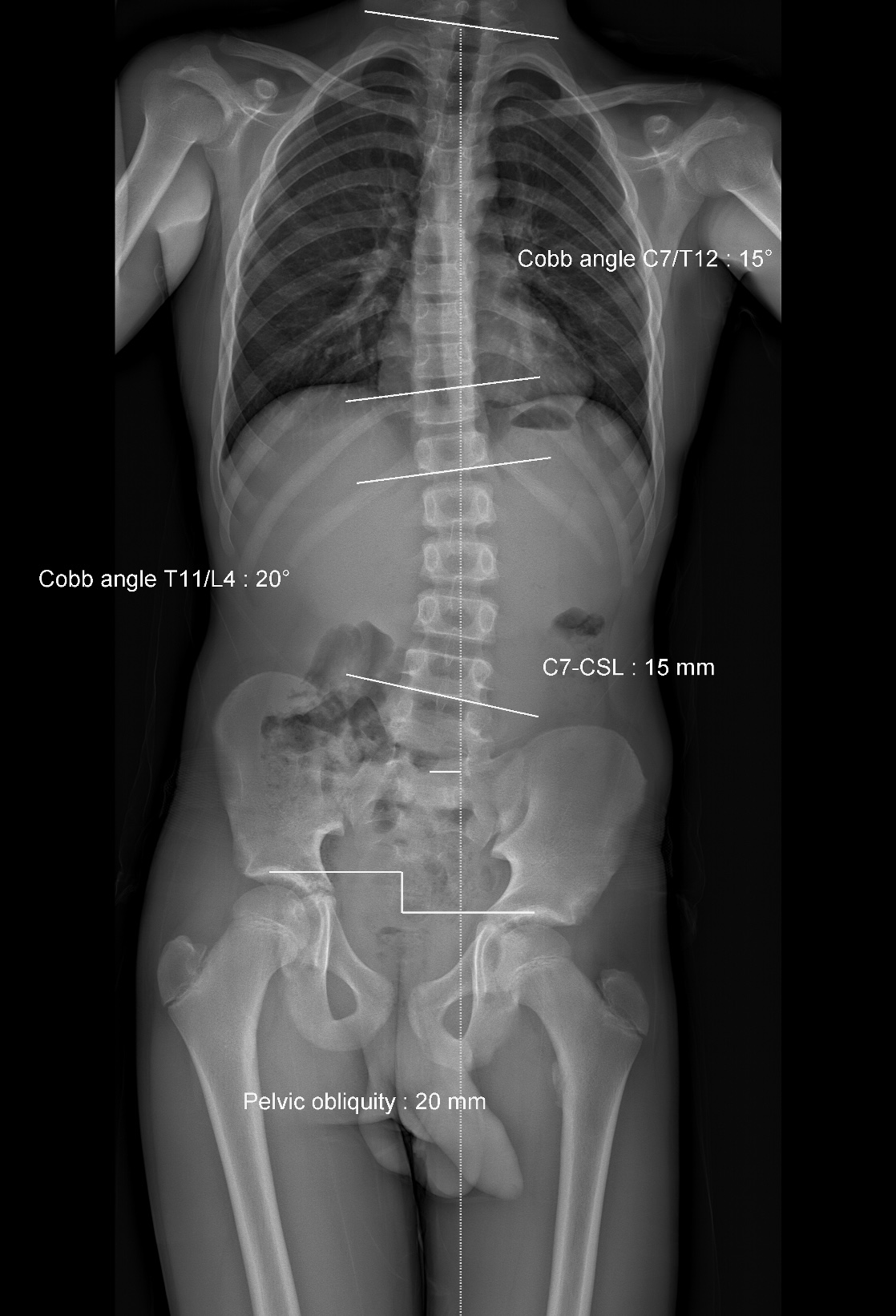
Pelvic obliquity and scoliosis secondary to LLD
Growth
| Proximal femur | Distal femur | Proximal tibia | Distal tibia | |
|---|---|---|---|---|
|
Growth
|
3 mm / year |
9 mm / year | 6 mm / year | 3 mm year |
| % total leg | 15% | 37% | 28% | 20% |
| % femur | 30% | 70% | ||
| % tibia | 60% | 40% |
Growth cessation
- girls: 14-15
- boys: 16-17
Examination
Look

Pelvic obliquity - corrects with blocks
Scoliosis - corrects with sitting
Long leg - knee held flexed
Short leg - foot in equinus
Gait
Options
- walk on toes with short leg - most common
- walk with flexed knee on long leg - high energy expenditure
Short leg gait - head moves up and down as walk from long leg to short leg
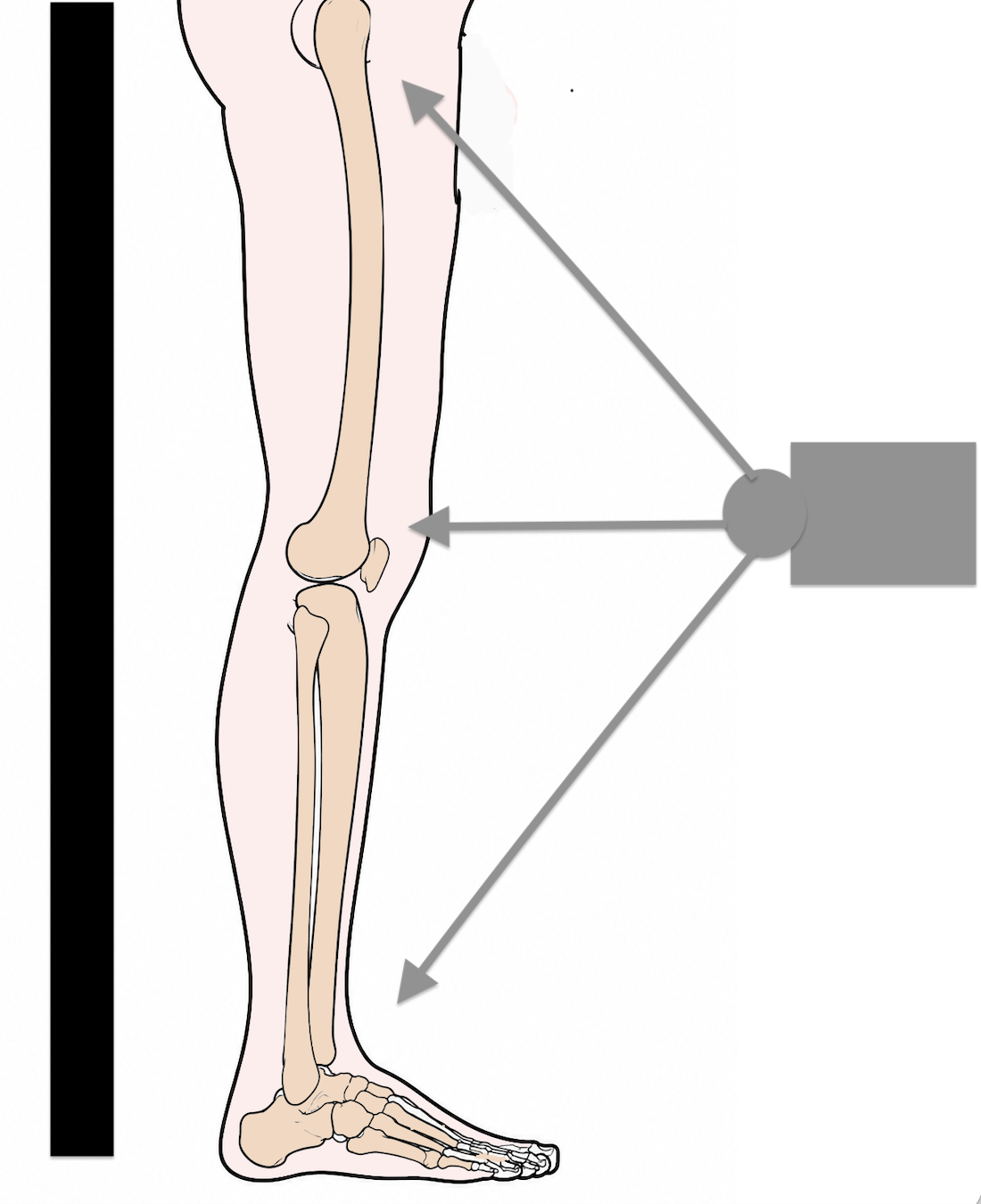
Measure LLD
| Functional LLD | Apparent LLD | True LLD |
|---|---|---|
|
Use blocks under short leg - correct pelvic tilt / scoliosis - correct knee flexion
|
Xiphisternum to medial malleolus
No correction for contractures - hip / knee / foot - coronal and sagittal plane |
ASIS to medial malleolus
Correct for contractures in coronal and sagittal plane - hip: exclude hip adduction or abduction contractures - hip: compensate for hip FFD with pillow under other hip - knee: compensate for knee FFD with pillow under other knee
|
| Measure desired correction |
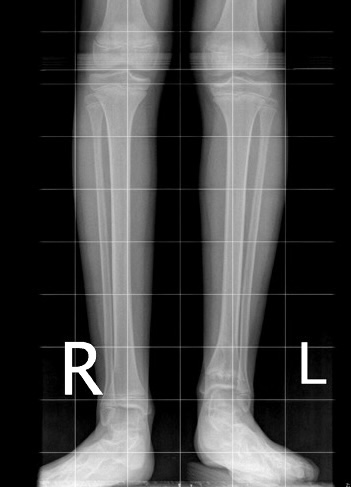
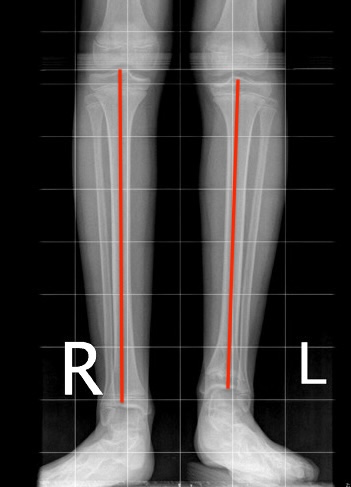
Identify site of shortening


Long right femur
Galeazzi
- hips and knees flexed side by side
- look for tibial / femoral shortening
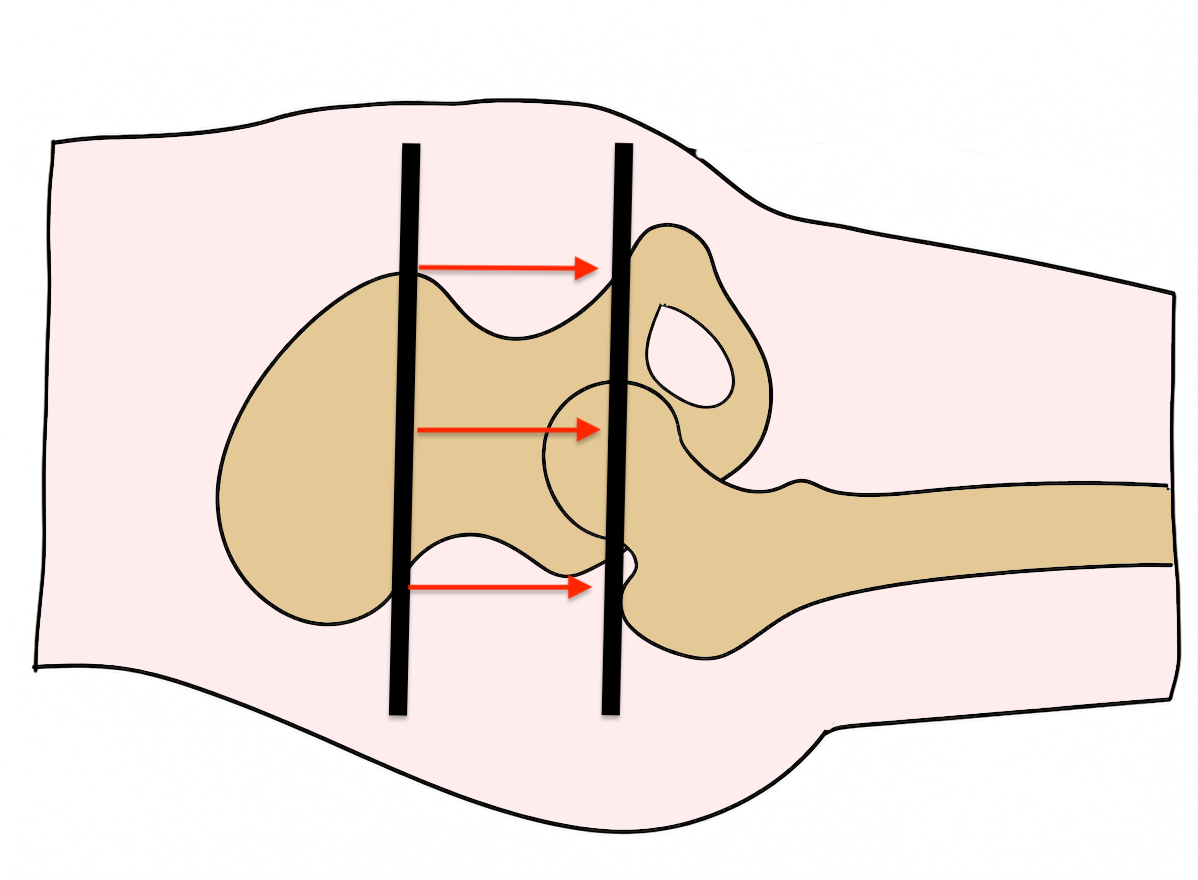
Bryant's triangle
- detects shortened femur above greater trochanter in hip
- distance between lines perpendicular to GT and ASIS
- compare each side
Examine knee
Conditions such as fibula hemimelia associated with ACL deficiency
Can cause issues with femoral lengthening procedures
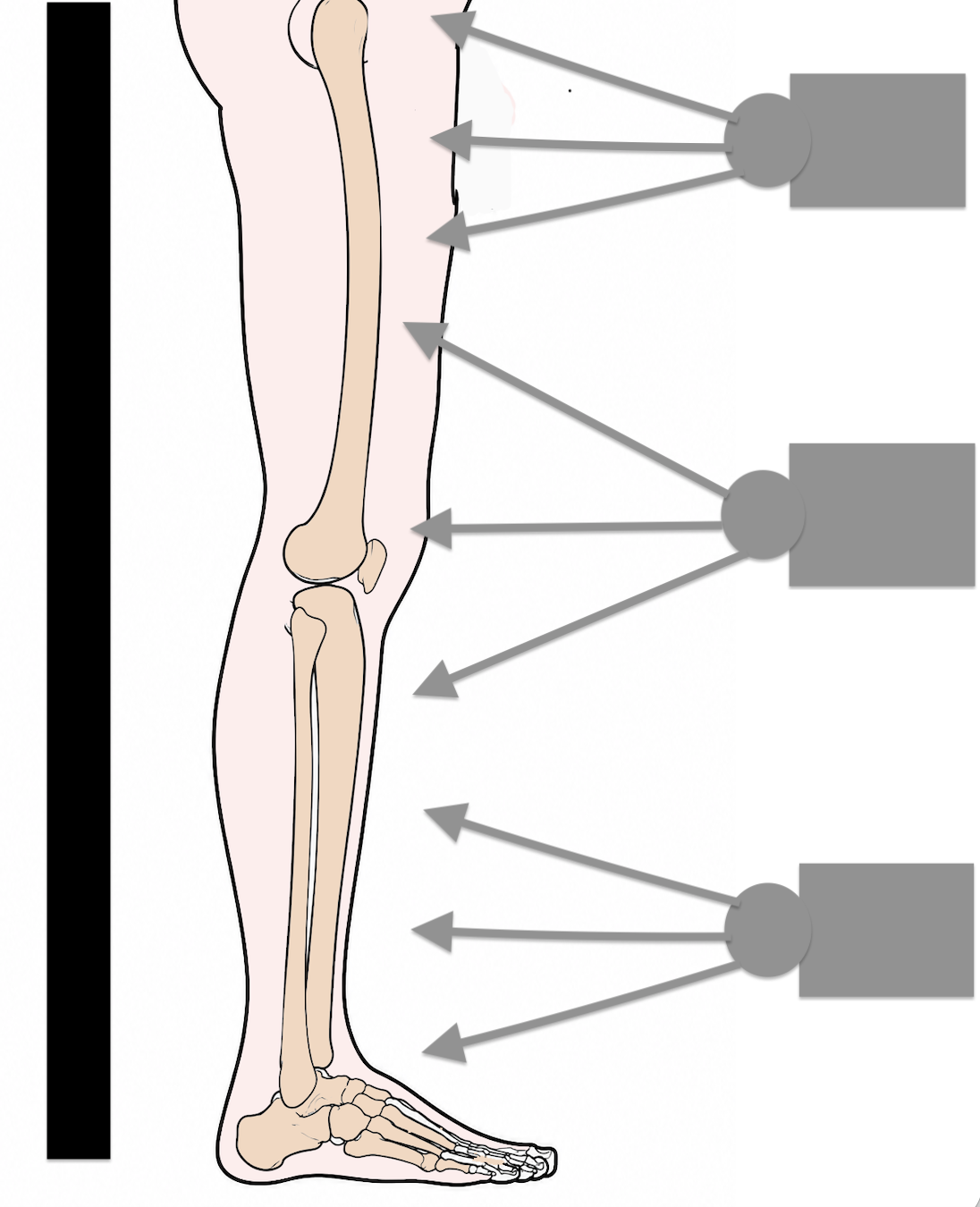
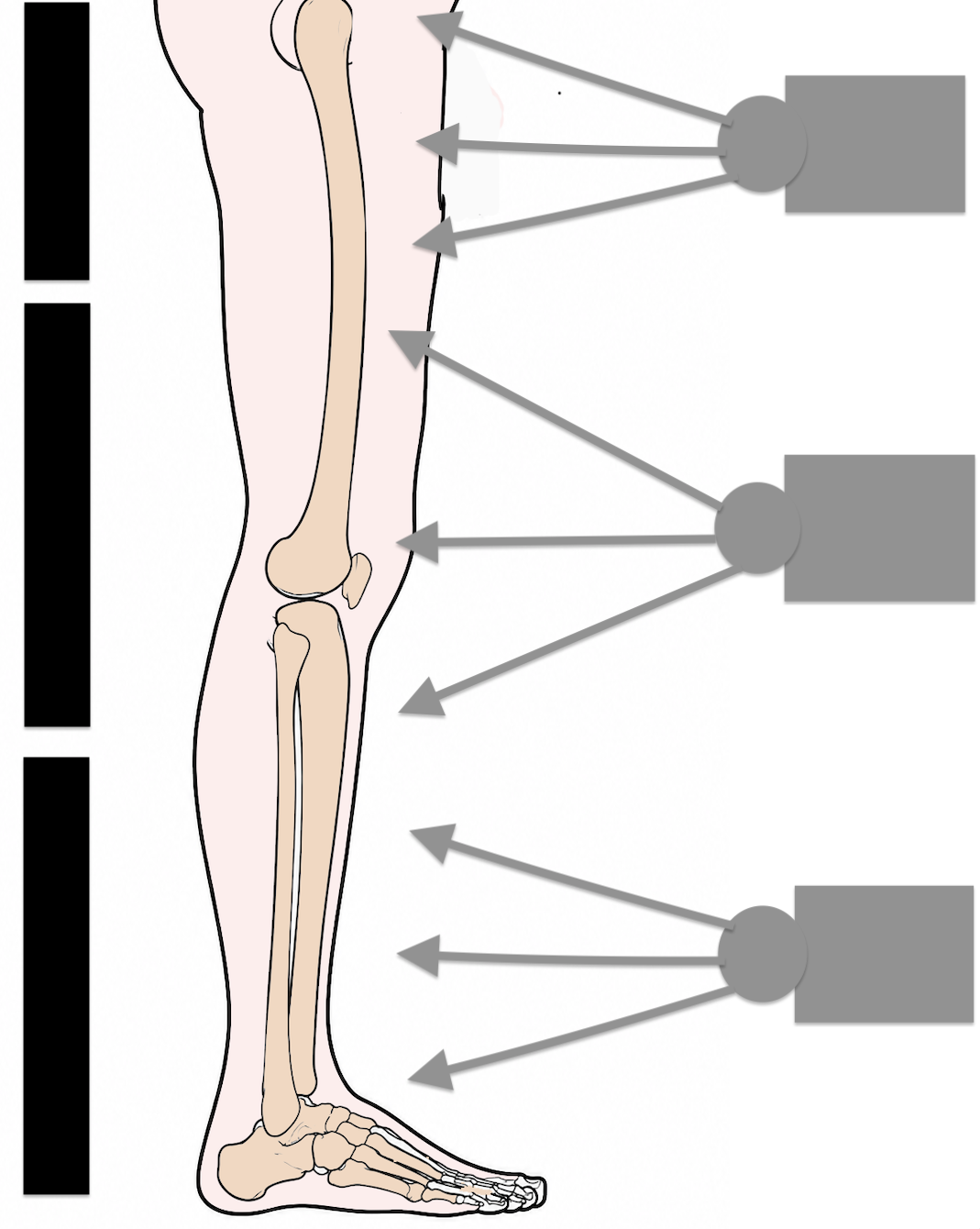
Four outcomes
|
Symmetrical Stance Level Pelvis |
Symmetrical Stance Oblique Pelvis |
Asymmetrical stance Level Pelvis |
Asymmetrical stance Oblique pelvis |
|---|---|---|---|
|
No LLD
Bilateral symmetrical deformity |
Uncompensated LLD
Hip / knee / ankle normal position |
Fully compensated LLD
Flexed hip Flexed knee Equinus ankle |
Partially compensated LLD
Partly flexed hip / knee / ankle |
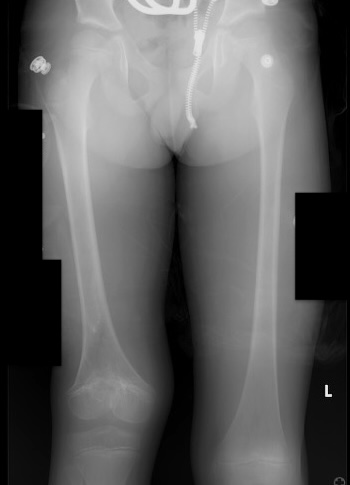
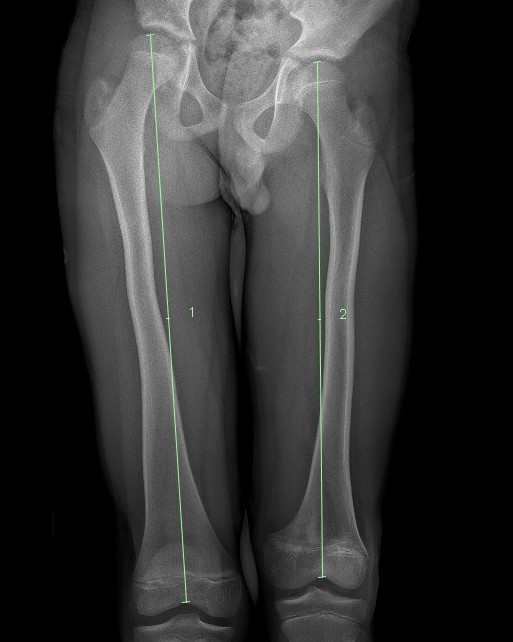
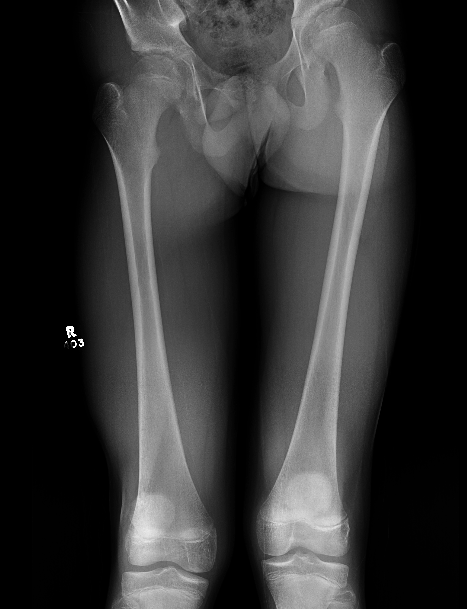
X-ray

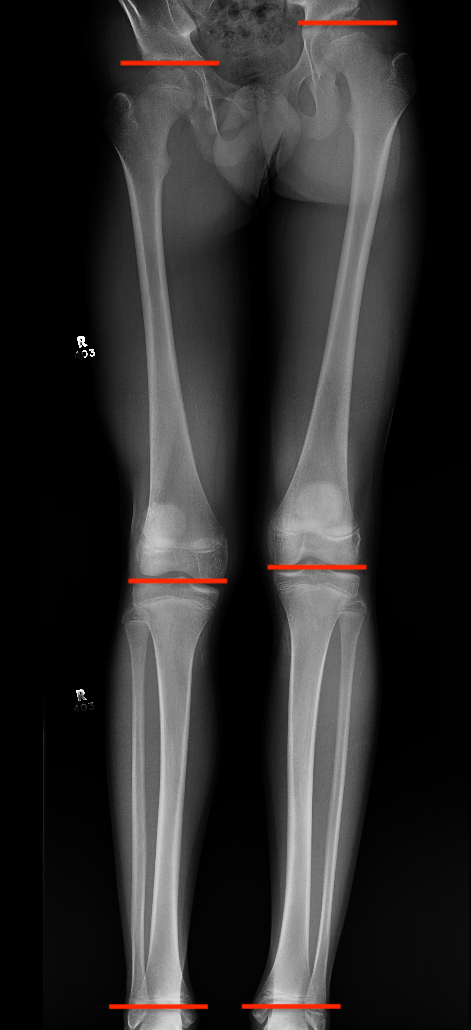
| Teleroentgenogram | Orthoroentgengram | Scanogram |
|---|---|---|
|
Single exposure Single film |
Multiple exposures hip / knee / ankle Single film |
Multiple exposures hip / knee / ankle Separate film hip / knee / ankle |
 |
 |
 |
| Parallex error | Parallex error |

Skeletal Age

Greulich-Pyle atlas using PA xray of the left hand
- estimate skeletal age
- peak growth boys skeletal age 14
- peak growth girls skeletal age 12
- 2 years of growth after distal phalanges have fused


12 year old versus 14 year old hand xray. Distal phalanges have fused in 14 year old.
Comprehensive guide to skeletal age: www.radiologykey/skeletal-age
Shapiro's development patterns of LLD
- longitudinal study of 800 patients with LLD
- age versus LLD with varying causes
- 5 main patterns of LLD over time
| Type I | Type II | Type III | Type IV | Type V |
|---|---|---|---|---|
 |
 |
 |
 |
 |
|
PFFD Growth arrest |
Polio Juvenile RA |
Femoral fracture overgrowth | Hip pathology | Juvenile RA |
Growth prediction
Concept
- predict LLD at maturity
- enables decision making on timing of eiphysiodesis
Menelaus Rule of Thumb
- girls stop growing at 14 / boys stop growing at 16
- distal femur 9 mm / year
- proximal femur 3 mm / year
- proximal tibia 6 mm / year
- distal tibia 3 mm / year
Green and Anderson growth remaining tables
- measured longitudinal growth in normal white children
- tibia and femur
- plotted average growth per year by skeletal age with standard deviations
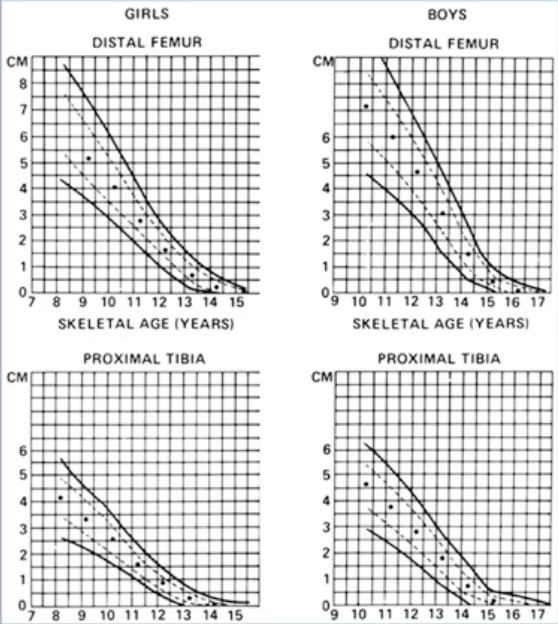
Green and Anderson growth remaining tables
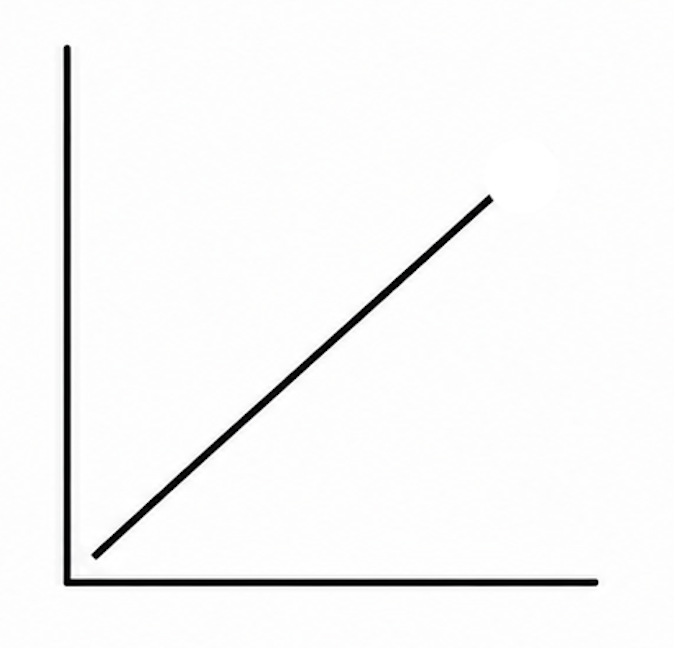
Moseley straight line graph
- converted Green and Anderson table to straight line
- three measures: length long leg, length short leg, skeletal age
- plot measures over three time periods
- estimate LLD at skeletal maturity
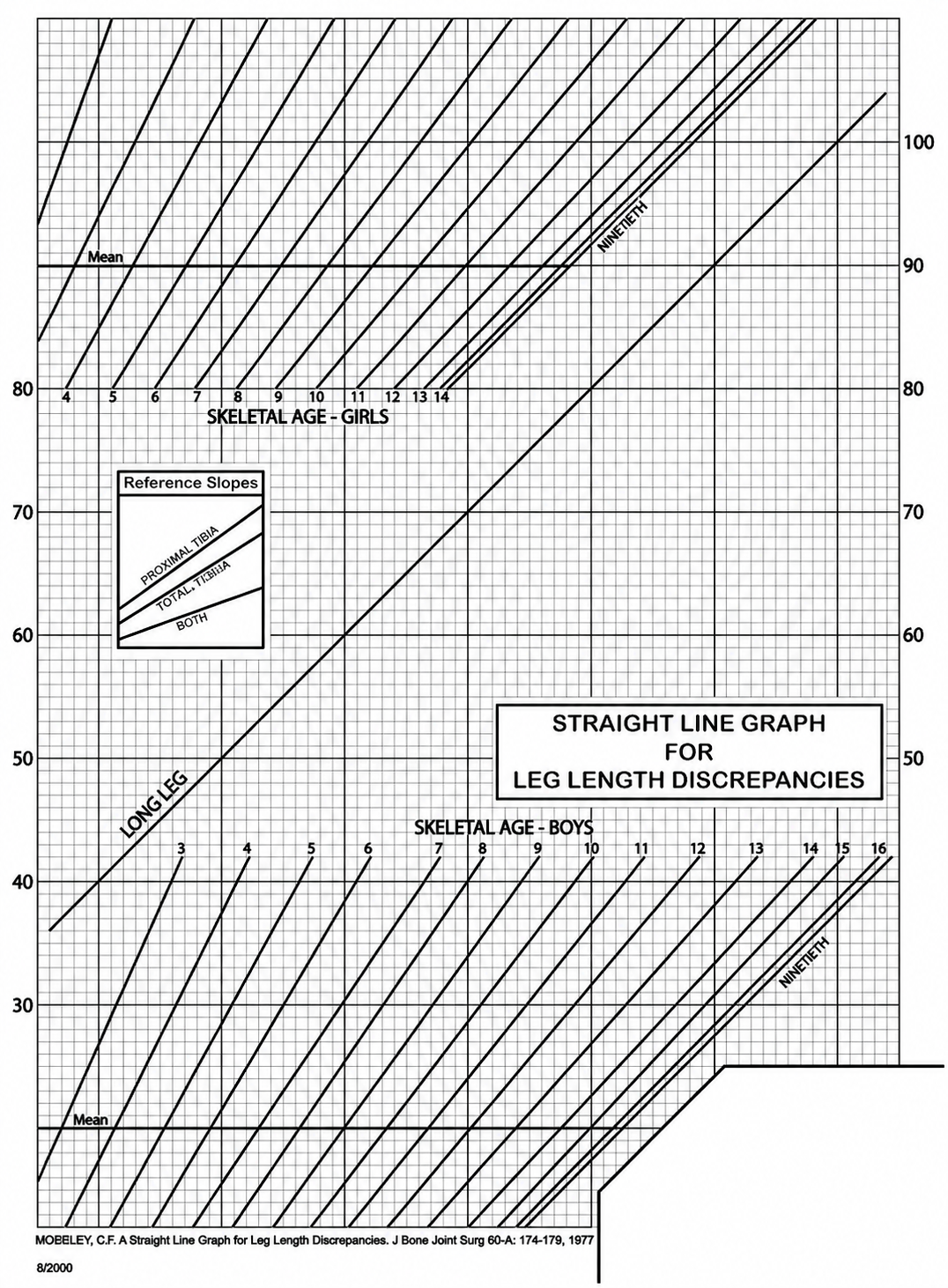
Moseley straight line graph
Paley multiplier method
- converted Green and Anderson table to a multiplier for tibia and femur over time
- use established multiplier for age and sex to determine LLD at maturity
- only works with Shapiro Type I LLD patterns
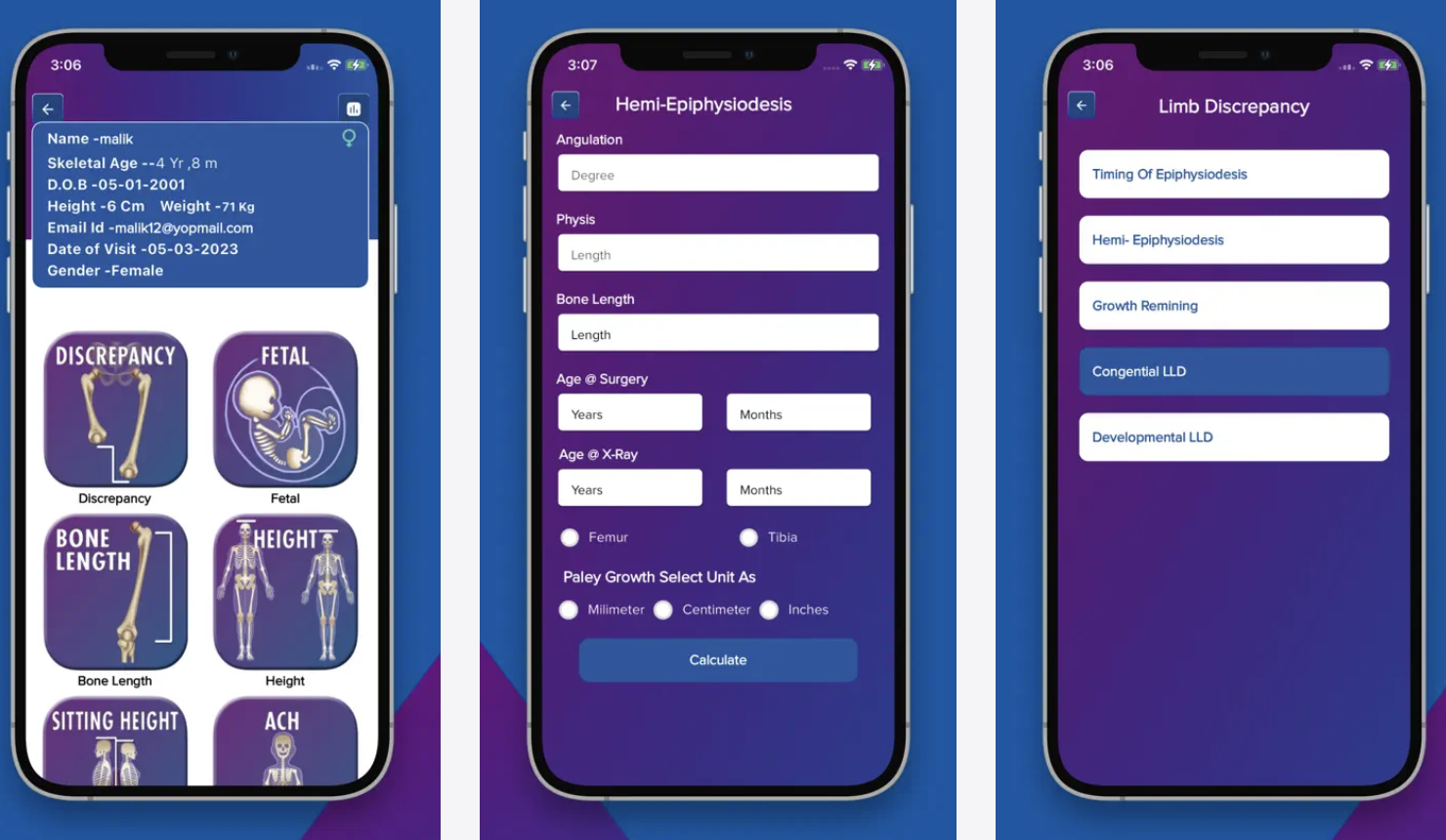
Paley growth multiplier app