fracture



Distal Tibial Fractures
Distal Tibial Fractures
Definition
Metaphyseal
Extra-articular

Intra-articular Extension
Patella sleeve fractures
Ossification
3 - 5 years old
Management
Undisplaced
- manage in plaster in extension
Displaced > 3 mm
- ORIF
Patella sleeve fracture
- usually small inferior fragment seen on xray
- patella high riding on xray / alta
- is actually large cartilaginous fragment avulsed with retinaculum
- can be osteochondral
Perthes
Issues
Femur
Multiplanar deformity
- worsend by previous surgery
- may require osteotomy
Acetabulum
Dysplasia often present
- not as severe as in DDH
LLD
Can be significant
Abductors
Have been short for long time
- difficult to restore length
Paget's Disease
Definition
Chronic, non metabolic bone disorder
Characterised by increased bone resorption, bone formation and remodelling
Epidemiology
Rare < 40
1 – 3 % population over 60
M > F
Aetiology
Unknown
Paramyxovirus implicated
- measles
- RSV
- canine distemper virus
Electron Microscope
Patella Fracture
Mechanism
Direct blow
- most common
Indirect
- forced knee flexion with foot fixed / maximally contracted quadriceps
Types
1. Vertical

2. Transverse
Medial Opening Wedge HTO

Position
- patient supine on radiolucent table
- place ECG lead and artery clip over centre of femoral head
- useful to put II ipsilateral to leg, and place knee on cassette
Tibial Stress Fractures
Epidemiology
Athletic / high impact exercises
Aetiology
First described in ballet dancers (Burrows 1956)
- tension side of bone / lateral side
- progression to complete fracture has been well documented in athletes
Signs
Point tenderness
- lateral aspect of tibia
Over time develop bony lump
Intertrochanteric Fractures
Definition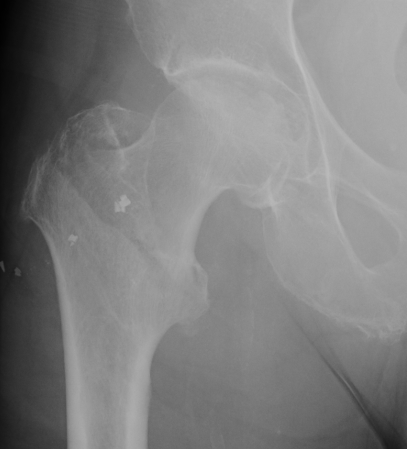
Fracture which extends between the trochanters of the proximal femur
- lower limit is inferior border of lesser tuberosity
Anatomy
Extra capsular / well vascularized
The key to stability is the posteromedial cortex
Perilunate dislocations
Epidemiology
Young men in 20's and 30's
Aetiology
High energy injuries
- fall from heights
- MVA
Mayfield Classification
Injury progresses from radial to ulna
- usually disruption proximal row either side of lunate
1. Capitate usually displaces dorsally initially
- volar lunate dislocation is end stage