Definition
Dorsal Intercalated Segmental Instability / CID
Anatomy
Scapholunate joint
- C shaped
- 2-3 mm thick dorsally with transverse fibres
- thin palmar
Dorsal extrinsic ligaments
- V shaped, onto trapezium
1. Dorsal RC ligament / DRC
- radius to triquetrum
2. Dorsal Intercarpal Ligament / DIC
- trapezius to scaphoid
Between these two ligaments is access to SL joint
Volar extrinsic ligaments
Radioscapholunate
- ligament of Testut
Epidemiology
Most common form of carpal instability
Classification
CID
Static
- SL diastasis
Dynamic
- positive Kirk Watson test
- nil SL diastasis without dynamic / stress imaging
CIND DISI
- secondary to radial malunion
- adaptive posture of proximal row
- lunate extends
- capitate translates dorsally and get OA
- treat with radial osteotomy if symptomatic
Aetiology
FOOSH
Scapholunate dissociation
- Mayfield Stage 1
Wrist extended / ulna deviated / supinated
- capitate driven into interval between scaphoid and lunate
Pathomechanics
CID (Complex Instability Dissociative)
- disassociation between scaphoid and lunate
- Palmarflexion of scaphoid
- dorsiflexion of lunate
The scaphoid will move into flexion
- due to its ligamentous attachments to the distal carpal row
Lunate extends
- due to ligamentous attachment to triquetrum
History
History of injury
Pain on radial side of wrist
Weakness of wrist
Certain movements may cause clicking or snapping
DDx
DR / scaphoid fracture
Dequervain's
Neuroma
Ganglion
STT, wrist, RC OA
Examination
Swelling and tenderness over SLJ
- most specific
Pain with dorsiflexion and radial deviation
Kirk-Watson test


1. Passive wrist ulnar deviation
- thumb on dorsum wrist / index finger on scaphoid tuberosity
- in wrists with instability, the scaphoid is displaced dorsally over the lip of the radius
2. Passive wrist radial deviation
- the scaphoid's proximal pole returns to its position in the scaphoid fossa of the radius
- as the scaphoid reduces, a clunking sensation and wrist pain are noted
1000 randomly examined wrists
- 11% had unilateral, asymptomatic increased scaphoid mobility on KW test
Patients with dynamic instability are distinguished by
- symptoms of instability and pain with KW test
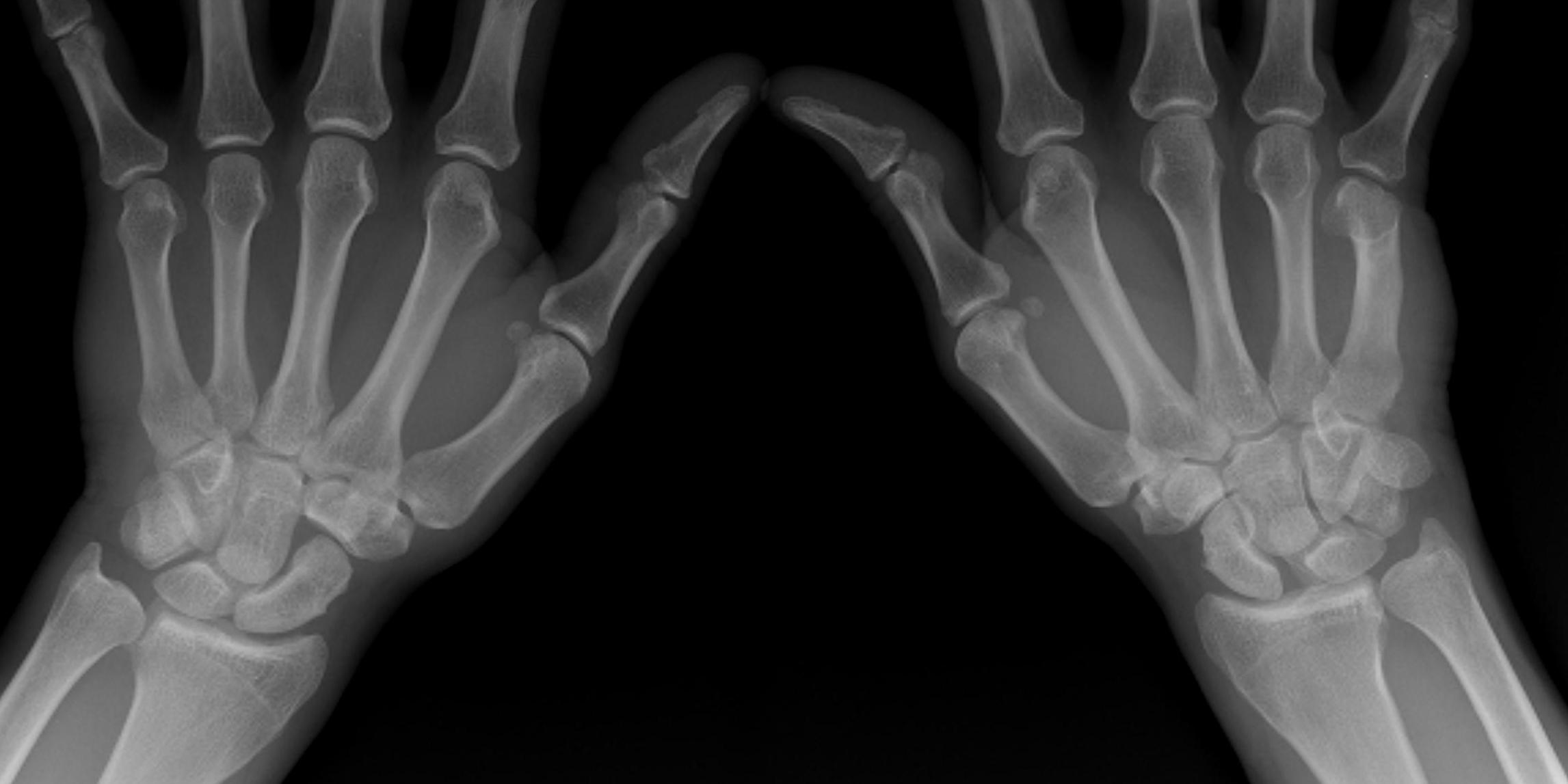
X-ray
Look for signs of SLAC wrist
- degenerative changes of scaphoid fossa with relative sparing lunate fossa
- indicates long standing
AP
Terry Thomas sign
- increased scapholunate interval
- > 3 mm compared with other side

Stress views
- bilateral wrists clenched
- in ulnar deviation
- in radial deviation
- may show Terry Thomas sign
Cortical Ring sign
- end-on view of cortex of distal pole of scaphoid

Scaphoid shortened
- due to palmar flexion

Lateral
Palmarflexion of scaphoid
Dorsiflexion of lunate
Increased scapholunate angle
- > 70o
- usually 30 - 60o



Increased luno-capitate angle
- normally < 10o

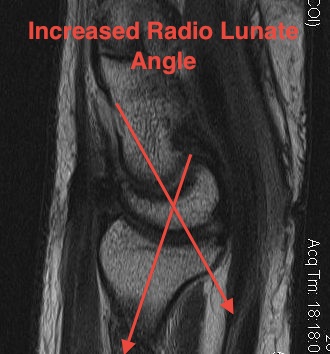
Increased radio-lunate angle
- normally < 10o
- lunate extended > 10o
MRI
Can demonstrate tear
- need experienced radiologist
- need MRI in correct plane
- sensitivity may be as low as 40%
Arthroscopy
Best method of diagnosis
Gold Standard
Acute Management
Definition
Within 3-6 weeks
Options
Partial
- immobilise 6 / 52
Complete
- SL diastasis
- usually torn off scaphoid
- repair
Technique
Approach
- dorsal midline approach
- 3 / 4 interval (3rd and 4th extensor compartments)
- open capsule between DRC and DIC ligaments
- radially based flap
Reduction
- K wires into scaphoid and lunate
- use as joystick to reduce
- extend scaphoid, some flexion of lunate
- K wire fixation to hold in place (SL and SC x 2)
- neutralises rotational forces during healing
Repair
- micro anchors ain scaphoid
- or can place drill holes in scaphoid to pass sutures
- 2.0 ethibond
+ / - Augmentation
- Blatt capsulodesis
- SL screw / pseudoarthrosis
Post op
- 8 weeks POP
- remove K wires
- patient will lose some ROM
Chronic
Definition
> 12 weeks
Indications
Failed reconstruction / missed injury

Surgery only for significant disability
- no reconstructive technique excellent
- inconsistent results, loss of reduction, loss of pain relief over time
Options
Ligament repair
Ligament reconstruction
Blatt capsulodesis
Reverse Blatt capsulodesis
Brunelli Tendodesis
Limited wrist fusion
1. Ligament repair and capsulodesis
Sufficient tissue available for repair
Reinforce with Blatt capsulodesis
2. Ligament reconstruction


3. Blatt Capsulodesis
Indications
- chronic DISI with insufficient tissue for repair
- to augment ligament repair
- dynamic instability
Technique
- dorsal, proximally based capsular flap 1 cm wide
- reduce scaphoid out of flexion and K wire (SL / SC)
- suture anchor distal pole scaphoid and attach capsular flap
- prevents flexion of scaphoid
- may combine with SLL reconstruction with PL
Post op
- plaster for 2/12
- removal K wires
The patients end up with a stiff wrist
4. Reverse Blatt
Difference
- leave capsule attached distally
- advance proximally
- limits wrist flexion
5. Brunelli Wrist Tenodesis
Harvest half FCR
- pass volar to dorsal through hole distal scaphoid
- insert dorsally into distal radius
- serves to derotate scaphoid
6. Limited fusion
Radial styloidectomy and STT fusion
Concept
- stabilise scaphoid in extended position
Kleinman J Hand Surg Am 1998
- no progression of arthritis seen in 16 wrists