Operative management / Rotator cuff repair (RCR)
Indications
Continued pain and dysfunction despite nonoperative management
Options
Open RCR
- detach deltoid from anterior acromion
- open acromioplasty
Mini-open RCR
- arthroscopic acromioplasty
- deltoid split for RCR
- avoid deltoid detachment
Arthroscopic RCR
Retear
Increased risk with larger tear size and patient age
- 1000 arthroscopic RCR with ultrasound at 6 months
- retear in 27% of full thickness tears
- increased risk as tear size increased
- increased risk with older patients
- 1600 arthroscopic RCR
- retear rate 7% with cuff tears < 2 cm2
- retear rate 44% with tears > 8 cm2
Increased risk with fatty degeneration
Wu et al J Orthop Surg Res 2025
- systematic review
- increased retear rates with increased fatty degeneration
Technical issues of surgery related to retear and patient outcomes
Acromioplasty
Distal clavicle resection
Open v arthroscopic
Single versus double row
Bone marrow stimulation
Biological augmentation of repairs
Collagen patch augmentation
Postoperative rehabilitation
RCR + Acromioplasty
- meta-analysis of 5 RCTs and 400 patients
- RCR +/- acromioplasty
- no difference in outcomes
- increased retear rates in non acromioplasty group
- thought to be related to type III acromions
RCR + Distal clavicle resection
- meta-analysis of 3 RCTs and 200 patients
- distal clavicle resection for ACJ OA did not improve outcomes
Open / mini open versus arthroscopic RCR
- systematic review of RCR with minimum 9 year follow up
- retear rate 41%
- no difference open v arthroscopic RCR
Long head of biceps pathology with RCR
Na et al J Orthop Surg Res 2019
- systematic review of tenotomy v tenodesis in RCR
- lower popeye and improved Constant scores with tenodesis
Franchesci et al Am J Sports Med 2008
- RCT 63 patients with RC tear and type II SLAP
- SLAP repair v tenotomy
- better outcomes with tenotomy
Single versus double row repair
- systematic review of single versus double row repair
- no difference for tears < 3 cm
- double row repair and tears > 3cm: improved ROM / clinical outcomes and decreased retear rates
Bone marrow stimulation
- systematic review of bone marrow stimulation of footprint
- K wire drilling of footprint / microfracture before RCR
- evidence that doing so decreases retear rate
Biological augmentation of RCR
- systematic review of 14 RCTs using PRP in RCR
- lower retear rates with PRP
- best with intra-operative application of leucocyte-poor PRP at time of surgery with large tears
- systematic review of mesenchymal stem cells for RCR
- 5 studies and 228 patients
- no difference in clinical outcomes
- may protect against retear
Collagen patch augmentation of RCR
- systematic review
- 6 RCTs and 400 patients
- lower retear rates for large tears
- no difference in outcomes
Postoperative rehabilitation
- meta-analysis of 8 RCTs and 670 patients
- early versus delayed range of motion
- early ROM superior ROM
- delayed ROM: better outcome scores and healing rates, especially with larger tears
- meta-analysis of 13 RCTs and 1000 patients
- early versus delayed range of motion
- better ROM with early ROM
- no difference in outcome scores or retear rates
Repair techniques
Transosseous
- with open repair
- pass cuff sutures through drill holes in bone
Single row anchor
- insert anchors at lateral edge of footprint
Double row anchors
- medial anchor row at articular margin and tie through medial cuff
- lateral anchor row at lateral footprint used to secure sutures
- increase surface area of cuff repaired to foot print
Trans-osseous equivalent / suture bridge
- cross sutures from medial row to lateral row
- increase contact between cuff and footprint
Arthroscopic Supraspinatous Repair
Technique
Vumedi arthroscopic double row small rotator cuff repair video
Vumedi arthroscopic double row large rotator cuff repair video
Set up
- lateral decubitus with arm traction
- beachchair in Tmax / Spyder (can depress arm and ER to aid visualisation)
- water pump
- adrenalin in bags
- stable BP 110
Portals
- posterior viewing portal
- lateral working portal over tear
- anterior portal for suture management
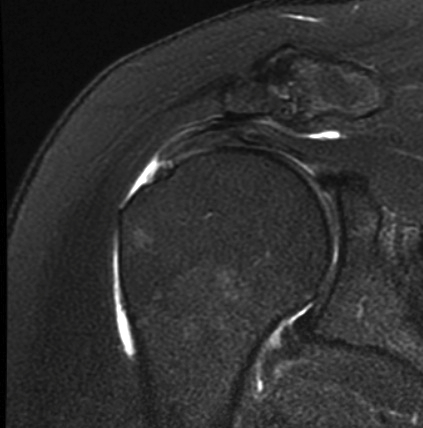
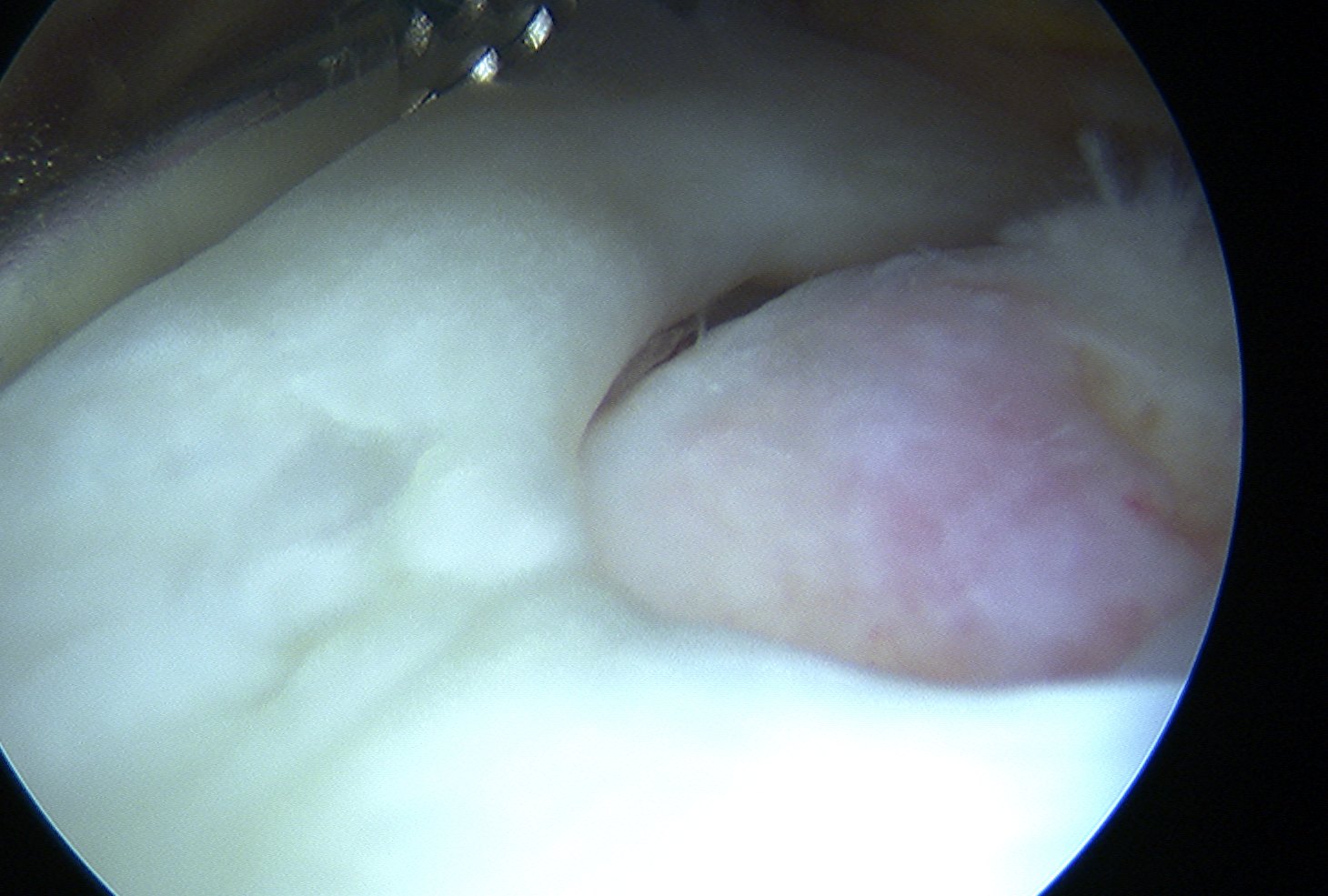
Glenohumeral joint
- inspect subscapularis
- evaluate SLAP / LHB tendinosis - tenotomy / tenodesis
Subacromial joint
- bursectomy for visualization
- acromioplasty if acromial spur
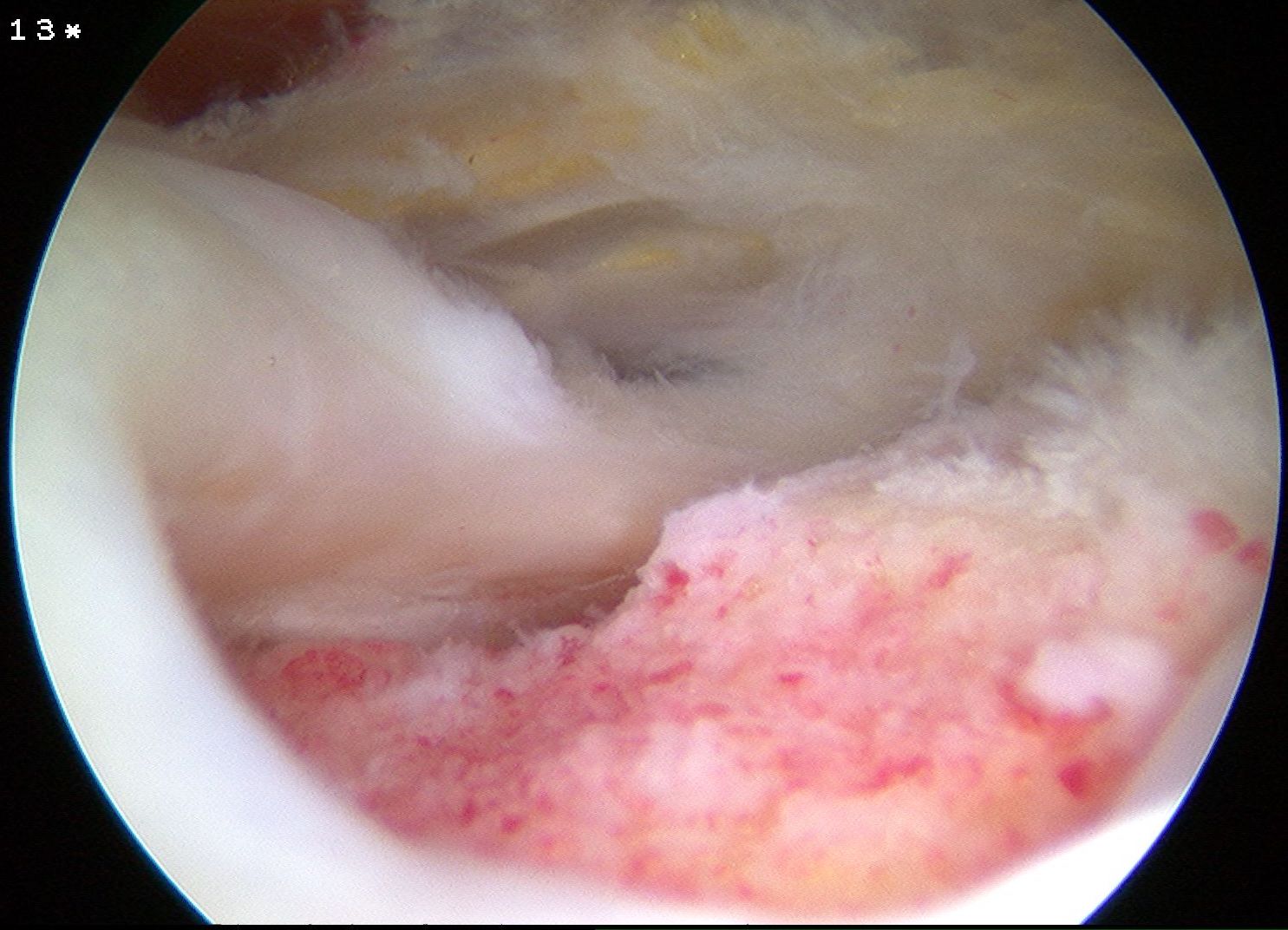
- debride footprint to bleeding bone
- +/- microfracture / K wire of footprint / marrow stimulation
Assess tear
- large tears may need releases
- consider margin convergence sutures for large U shaped tears
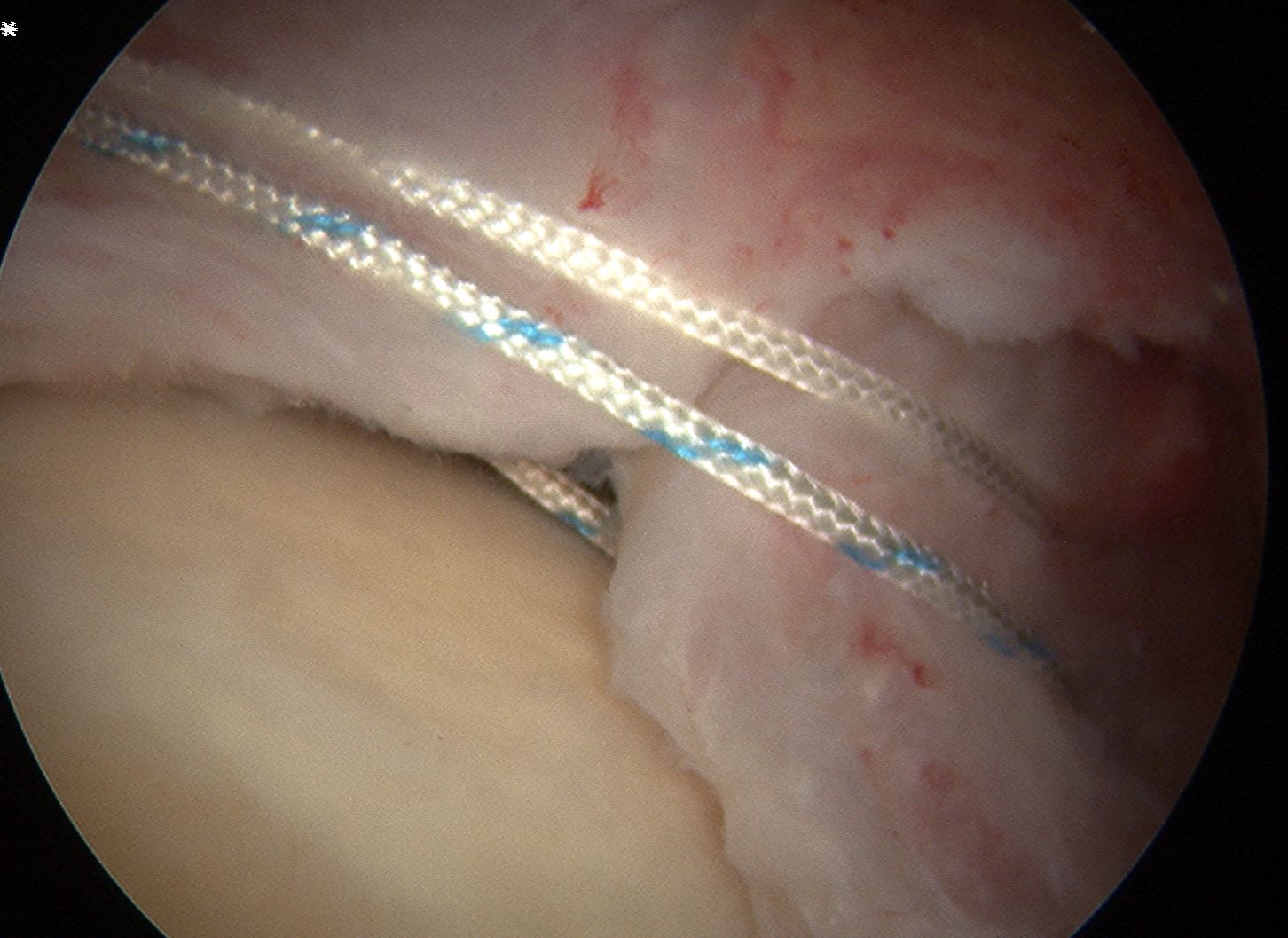
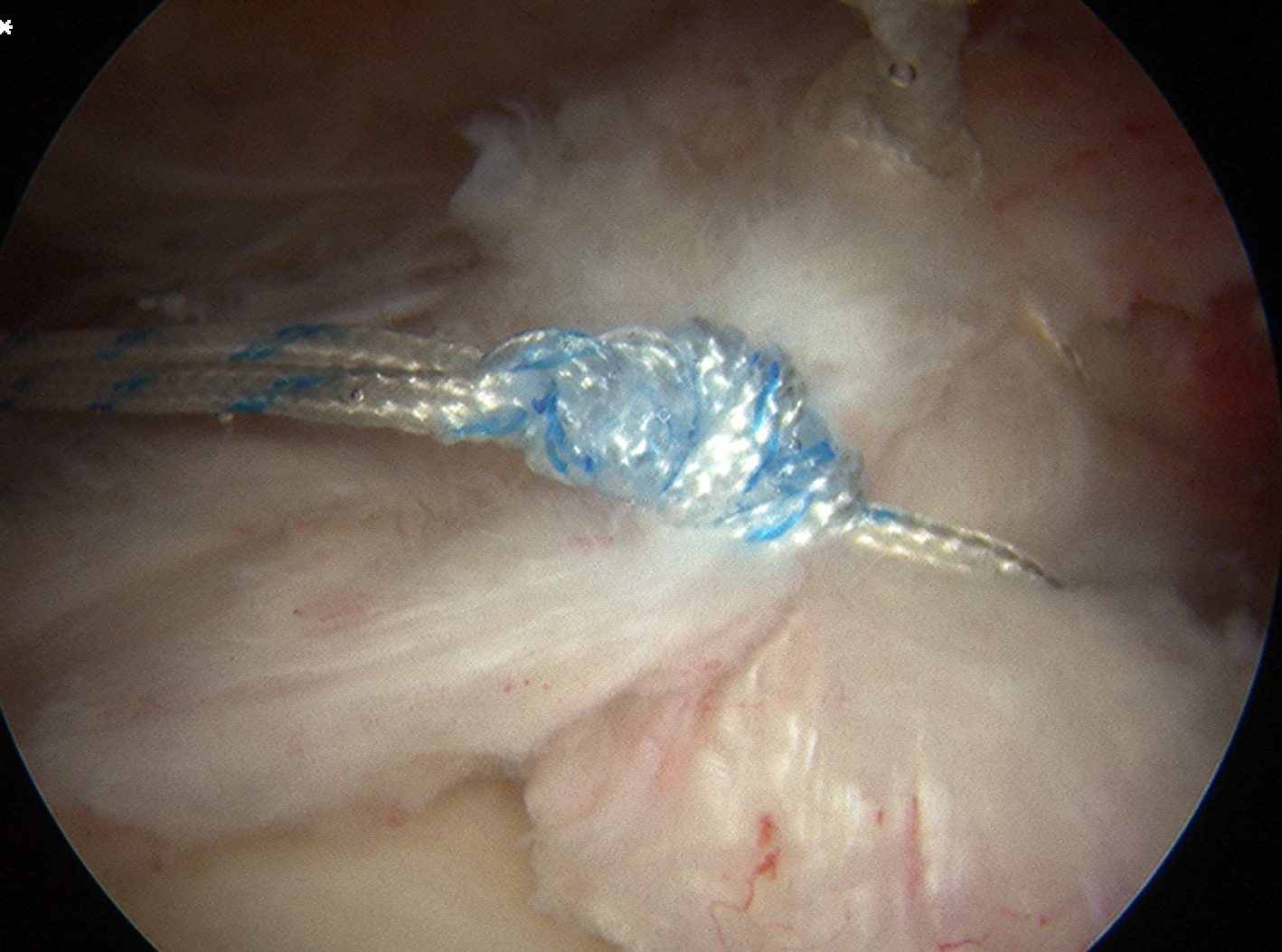
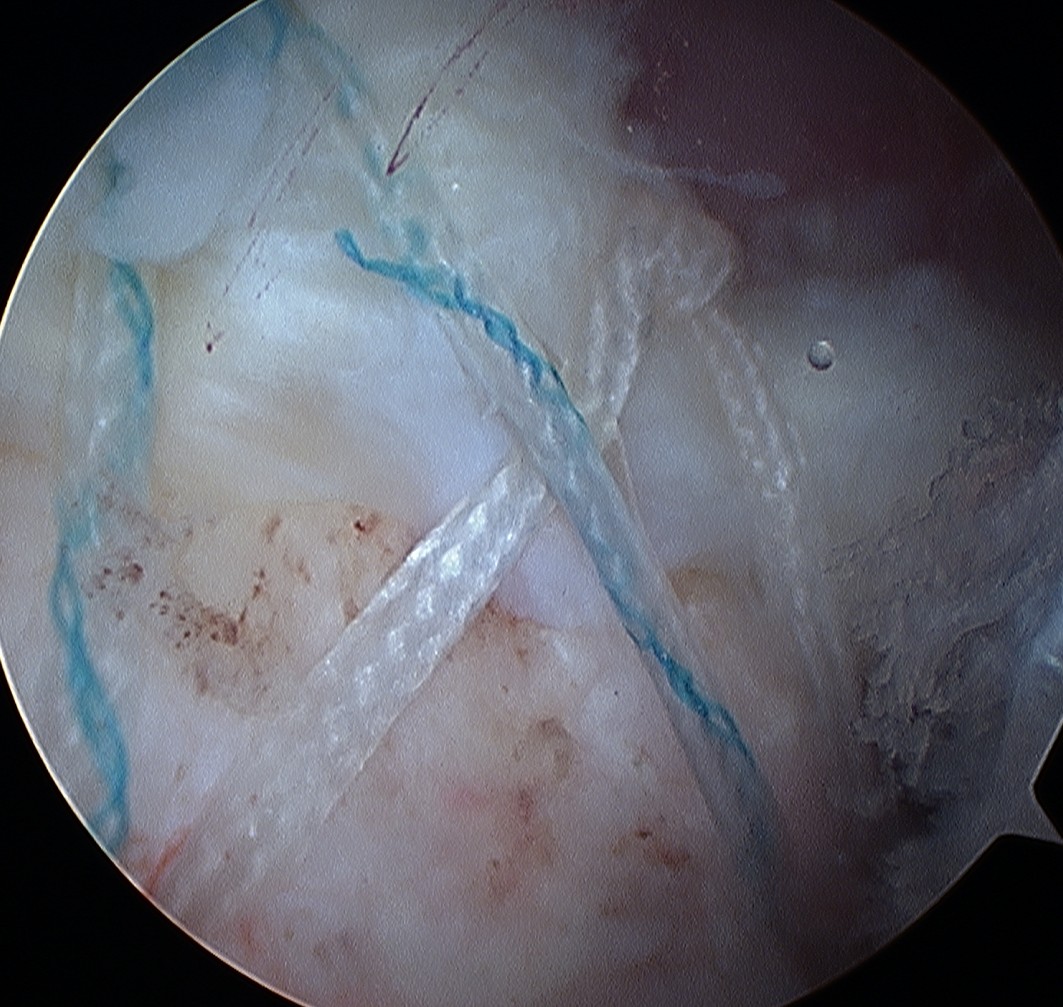
Margin convergence sutures
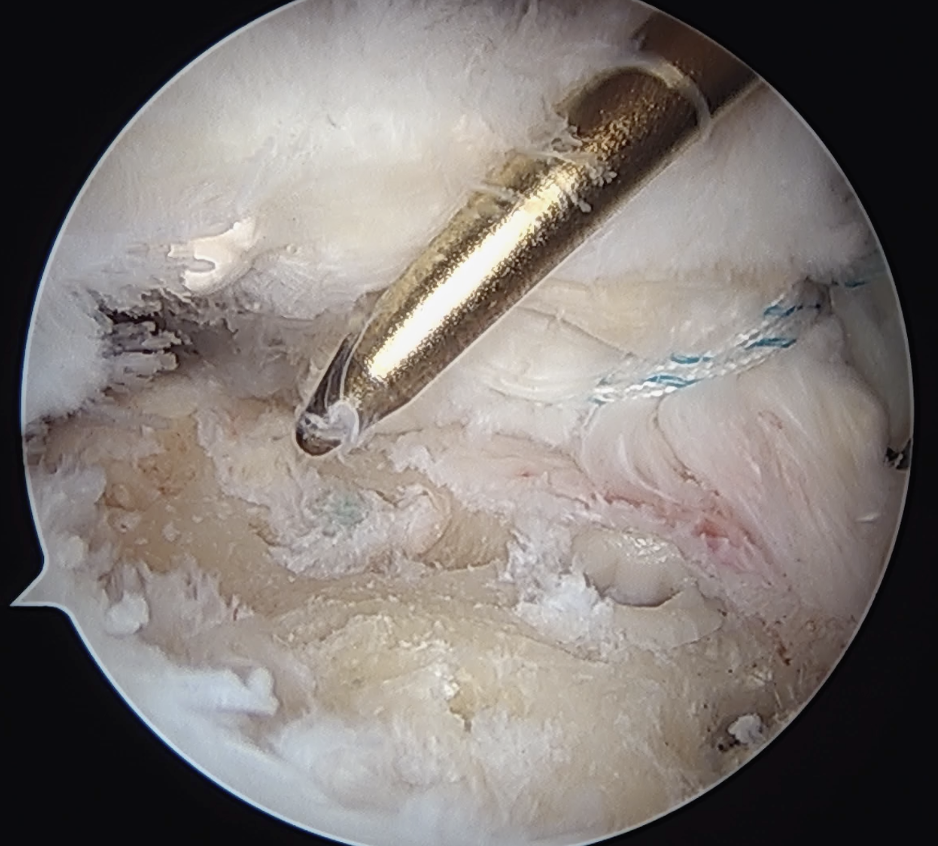
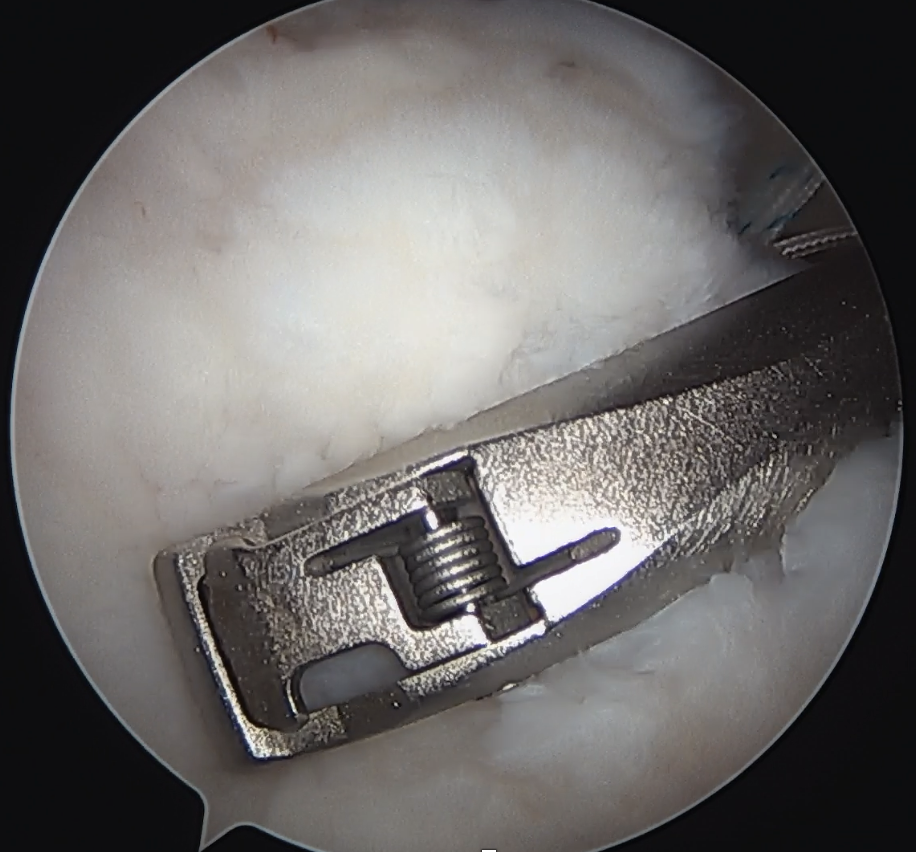
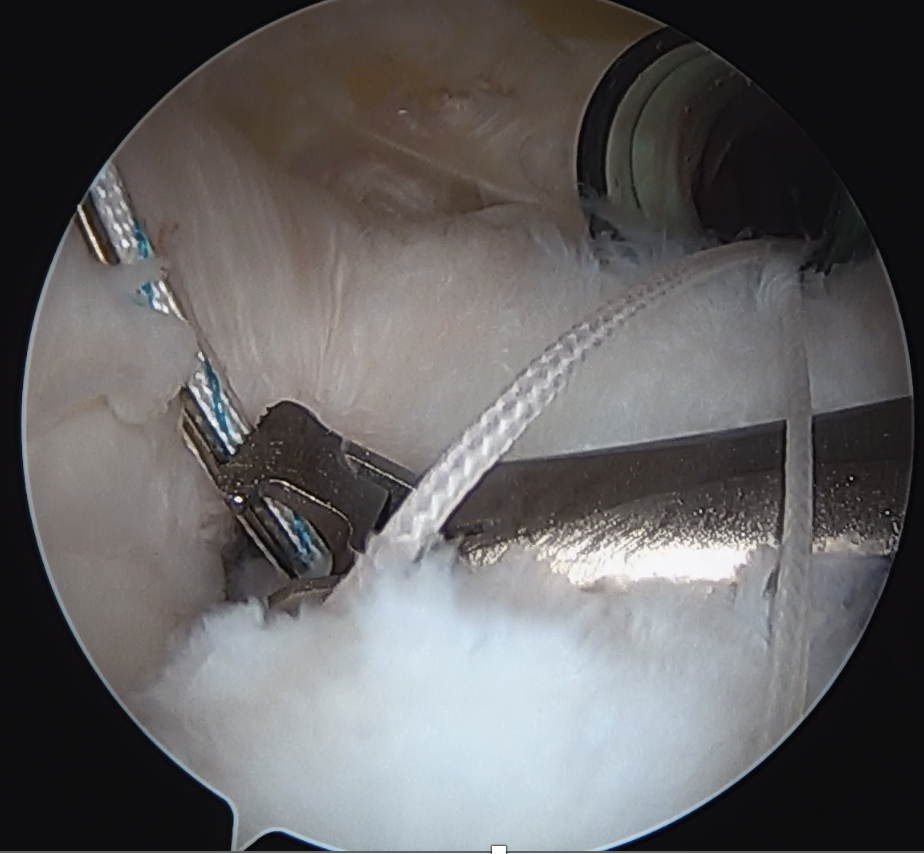
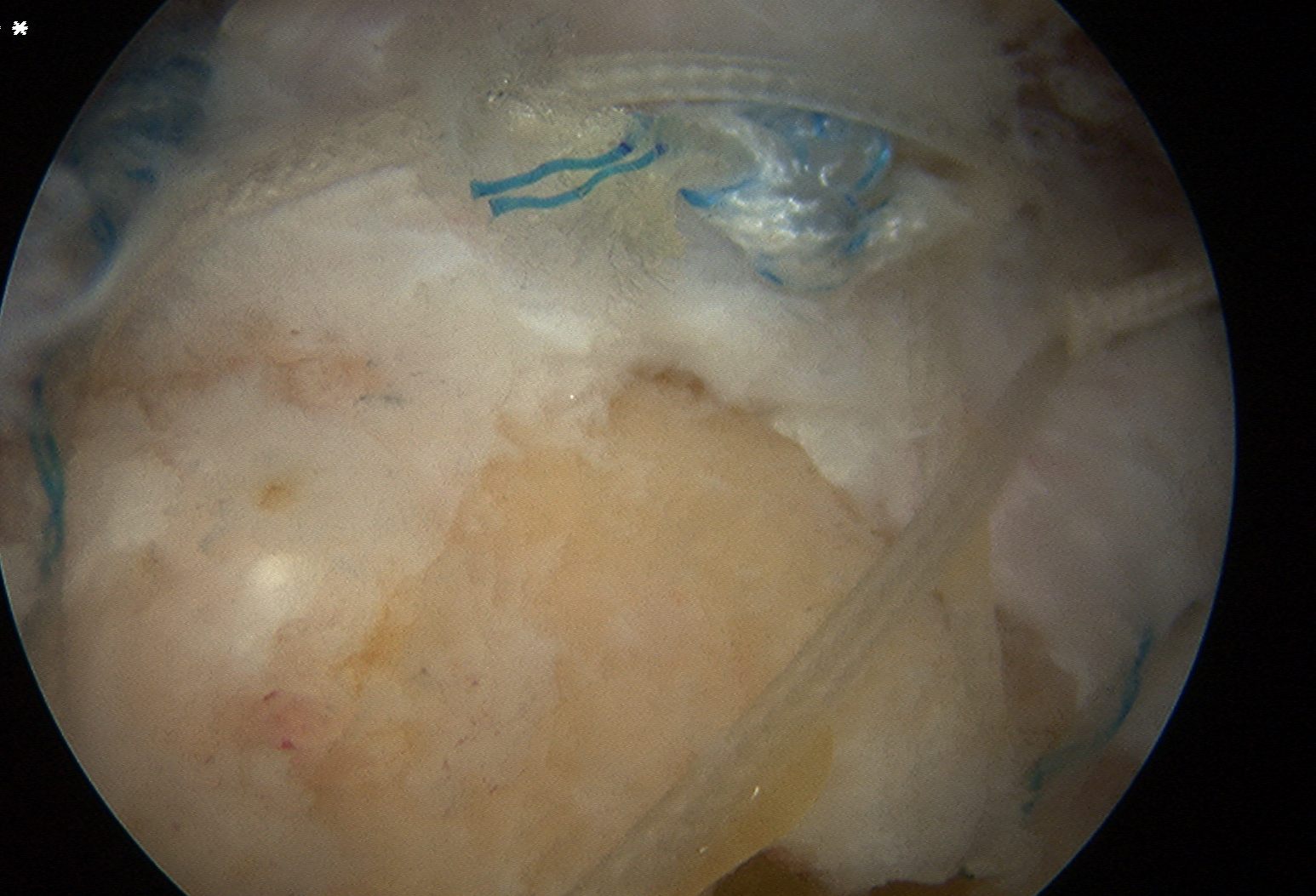
Medial row anchors
- inserted through additional stab incision for suture management
- just medial to articular cartilage

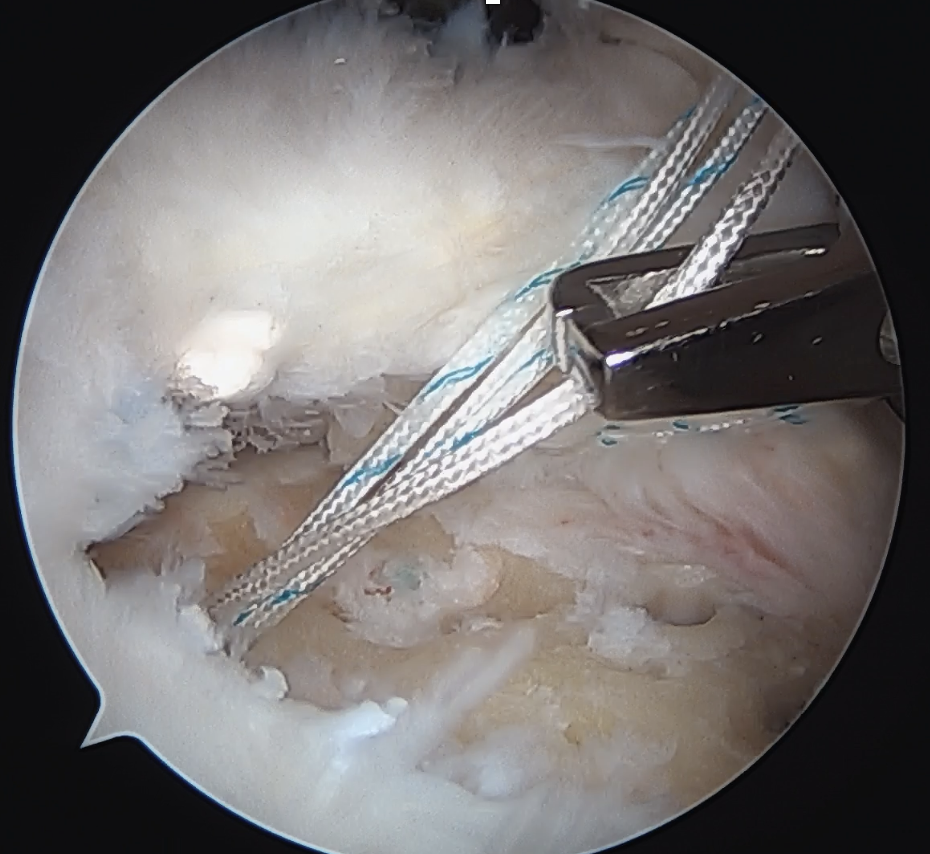
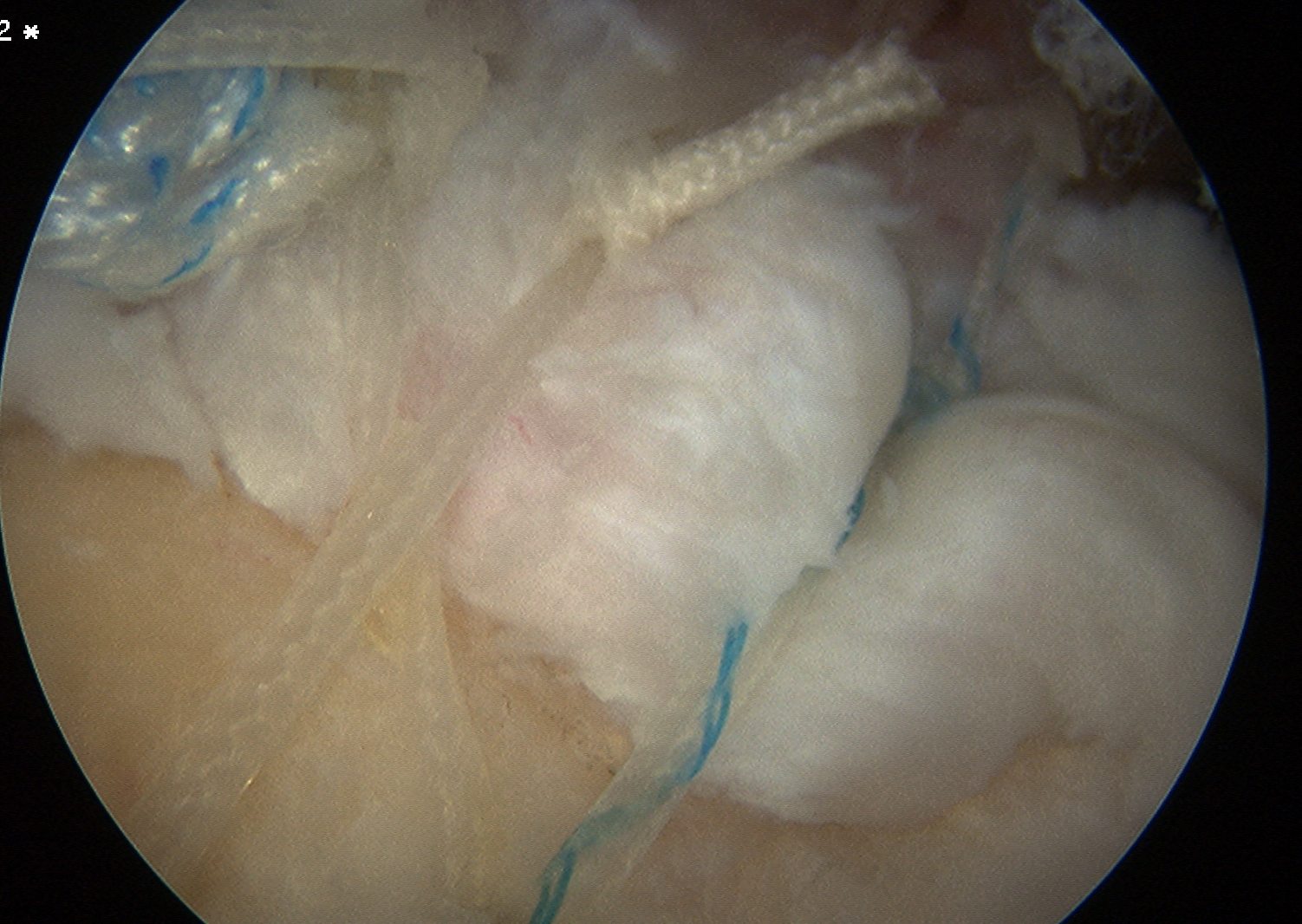
Pass sutures through medial cuff tendon
- camera posterior
- suture passer via lateral portal
- retrieve sutures through anterior portal
- repeat
- tie medial row
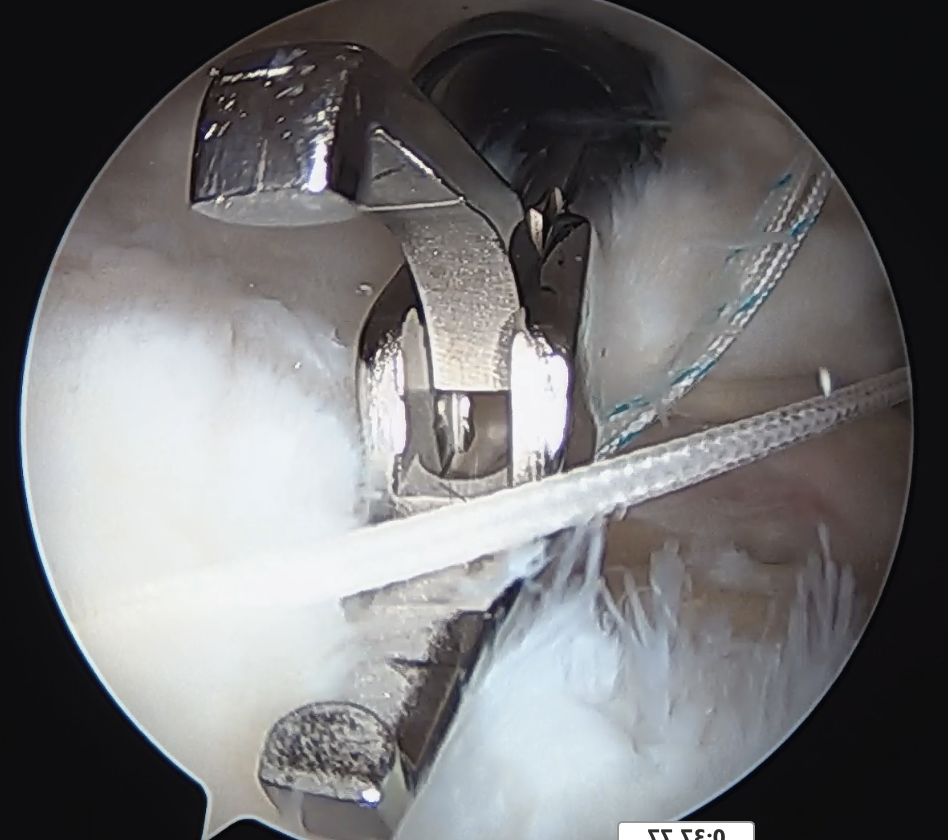
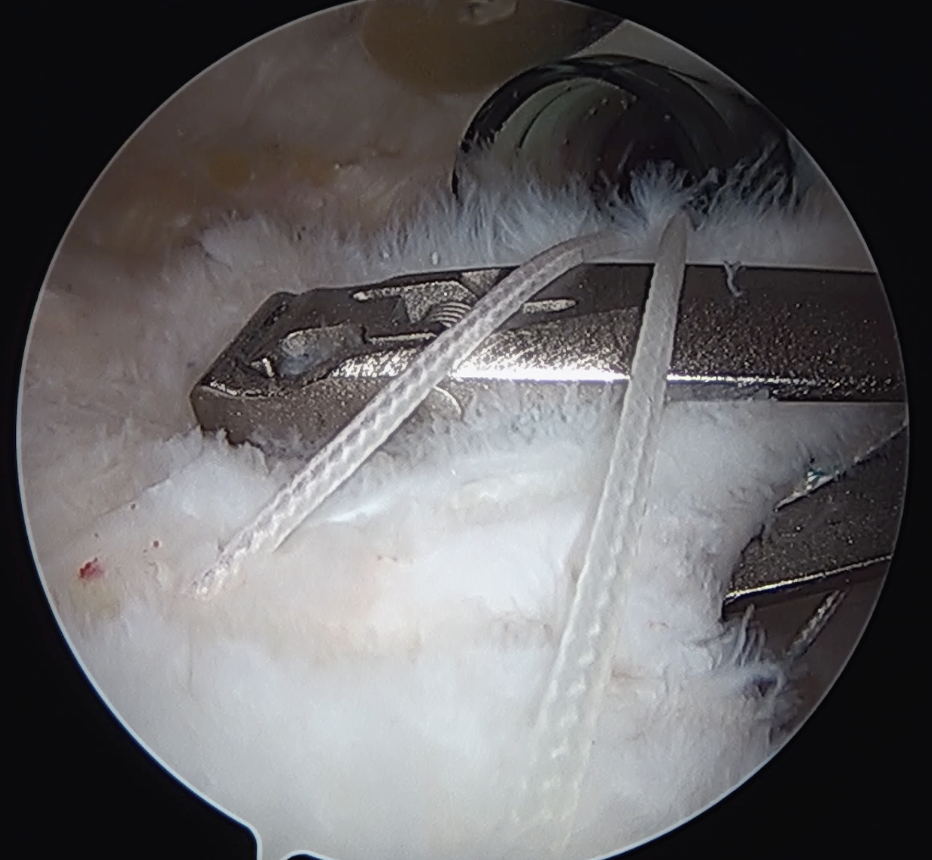
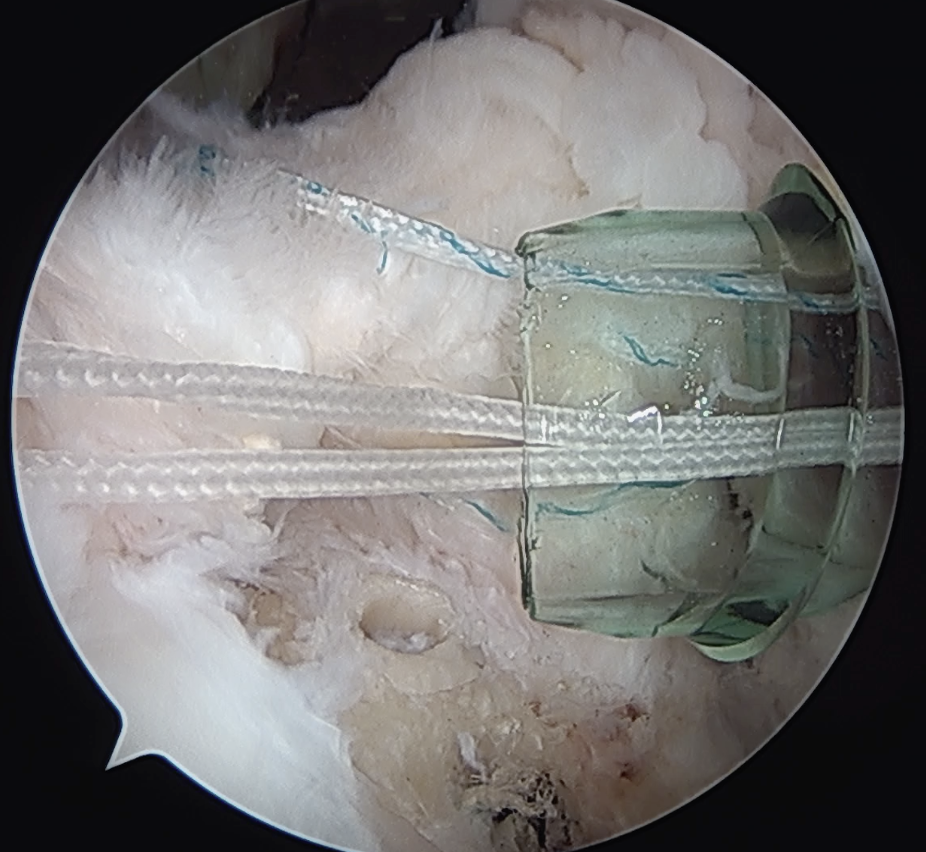
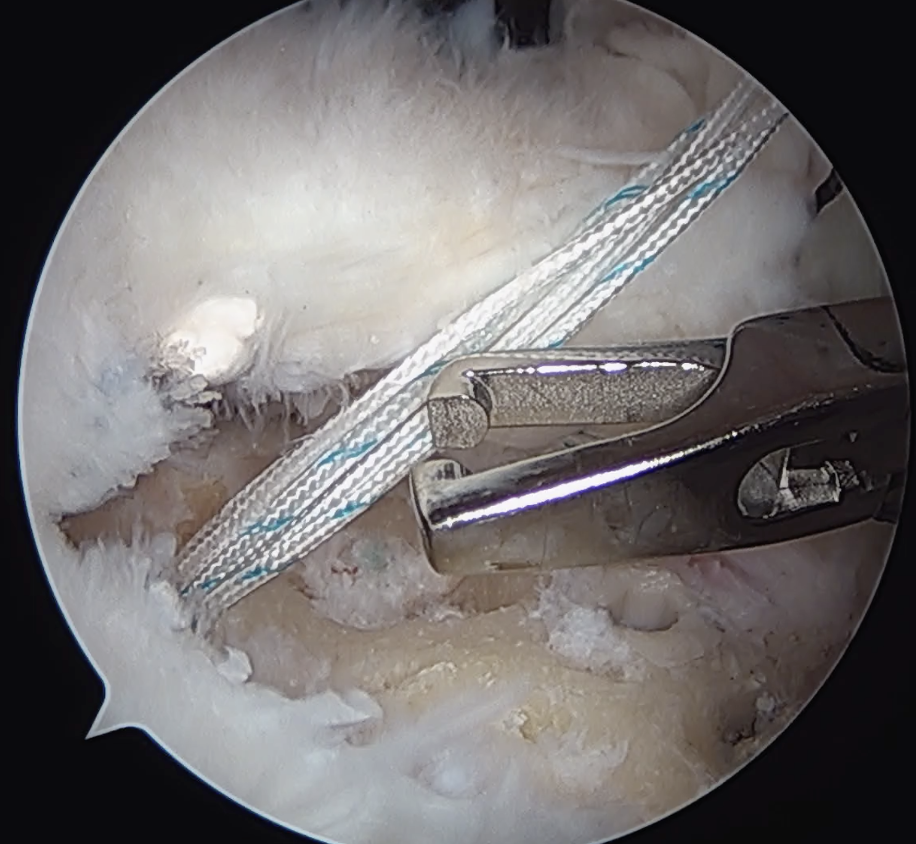
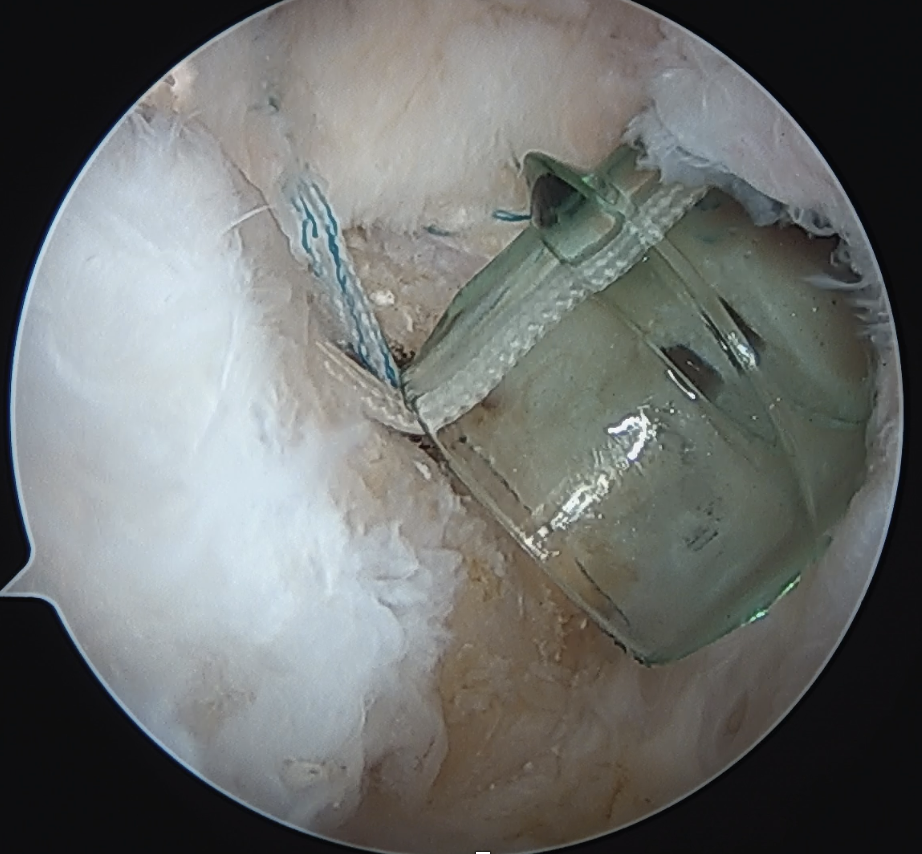
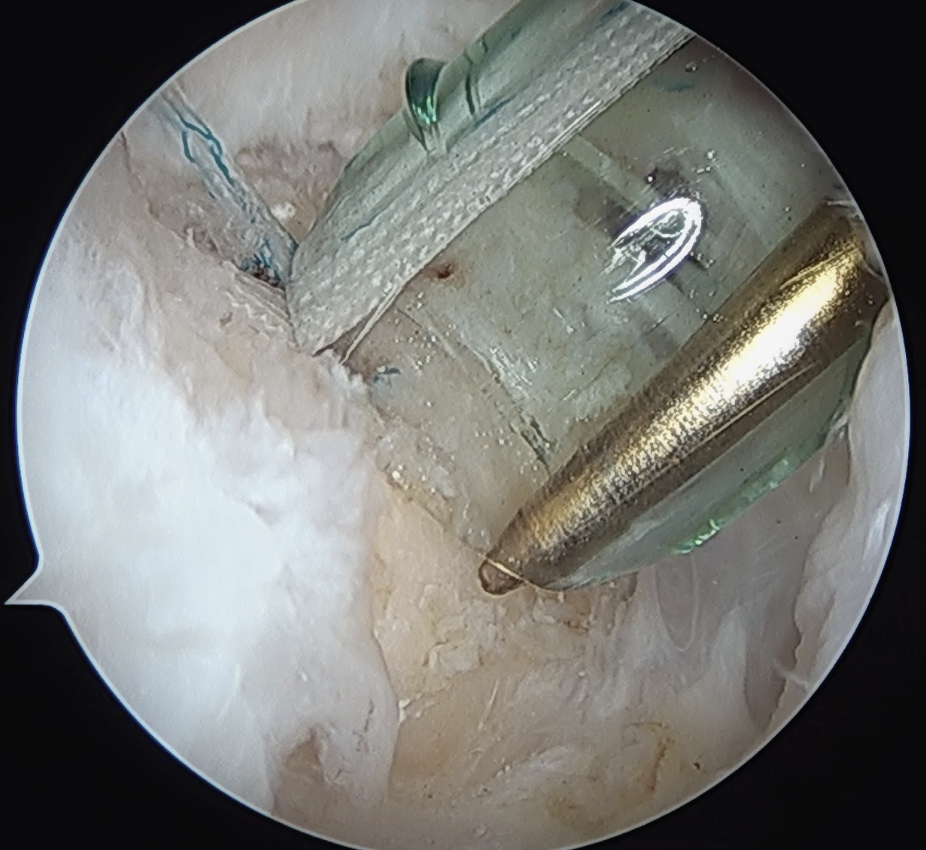
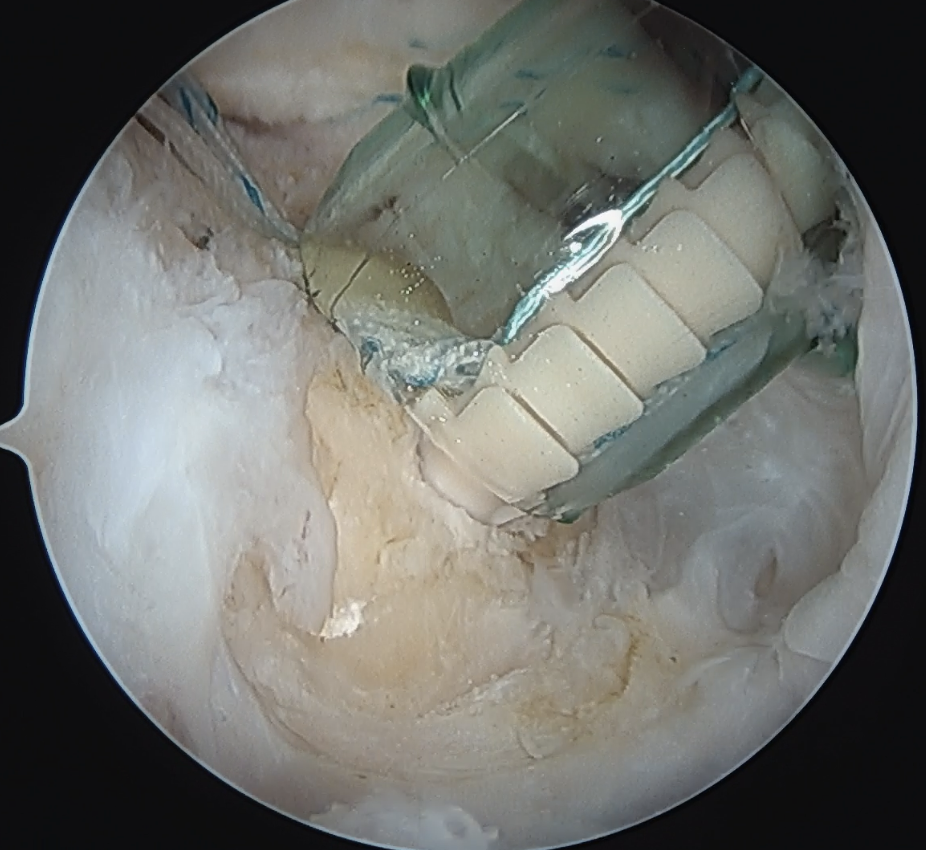
Double row / suture bridge
- use medial row sutures
- secure in knotless lateral row anchors
Open Rotator Cuff Repair
Open rotator cuff repair
Technique
Vumedi open rotator cuff repair video
Incision over ACJ and anterior acromion
- angle down between anterior and middle deltoid
- identify raphae between anterior and middle deltoid and split deltoid
- must not extend incision > 5 cm from acromion or risk damaging axillary nerve
- take deltoid off anterior acromion with diathermy
- control acromial branch of the thoracoacromial artery
- perform open acromioplasty
- perform rotator cuff repair to footprint
Mini-open rotator cuff repair
Technique
Vumedi mini open rotator cuff repair video
Arthroscopic acromioplasty
Deltoid split / repair rotator cuff
Complications of rotator cuff repair
Infection
Schairer et al Arthroscopy 2018
- 24,000 RCR in database
- infection 0.3%
- increased risk with open RCR
Venous Thromboembolism (VTE)
- database of 40,000 RCR
- VTE events 0.3%
- increased risk with prolonged surgery
Stiffness
- systematic review of stiffness after arthroscopic RCR
- 5% with full thickness tears
- 10% with partial thickness tears
Retear
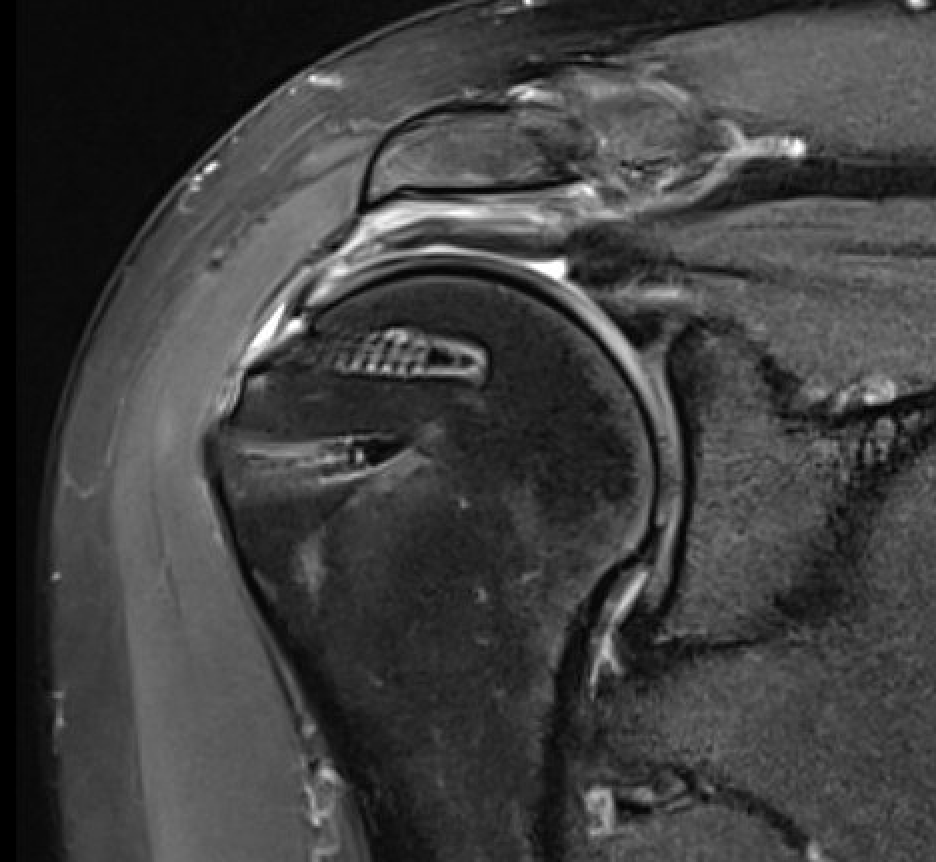
Presentation
Pain / stiffness / weakness
Incidence
- 1600 arthroscopic RCR
- retear rate 7% with cuff tears < 2 cm2
- retear rate 44% with tears > 8 cm2
Small - medium retears
Options
- revision rotator cuff repair
- +/- collagen patch augmentation
- systematic review of 900 arthroscopic revision RCR
- retear rate 25%
- reoperation rate 8%
- rTSA required in 3%
Large massive retears
Options
- superior capsular reconstruction
- tendon transfer - latissimus dorsi transfer / lower trapezius transfer
- reverse TSA
Welch et al Shoulder Elbow 2024
- systematic review rTSA with or without prior rotator cuff repair
- lower outcomes scores in patients with previous rotator cuff repair