

Definition
Chronic massive rotator cuff defect associated with high riding humeral head
- acetabularisation of the acromion
- glenohumeral osteoarthritis
Xray
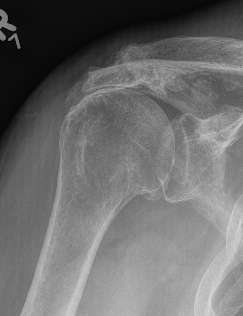
Superior migration of head without arthropathy
Acetabularization of the acromion and osteoarthritis
Differential diagnosis
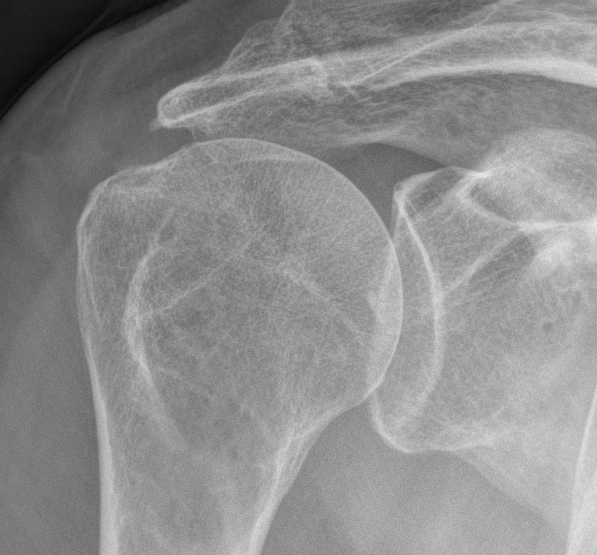
Glenohumeral osteoarthritis
- no superior migration of humeral head
- beard osteophytes on inferior aspect of the humeral head


Nonoperative management
Physiotherapy
- prospective cohort study of 450 patients with symptomatic full-thickness atraumatic cuff tears
- 6-12 weeks of physiotherapy
- only 27% elected for surgery (most in first 6 months)
- low expectation of physiotherapy, workers comp., and high functional demand predicted later surgery
Injections
Jiang et al J Orthop Surg Res 2023
- systematic review of cortisone v HA v PRP for rotator cuff tears
- 12 RCTs and 1000 patients
- short term pain relief with HA
- longer term pain relief and functional improvement with PRP
Operative Management
Options
Reverse TSA
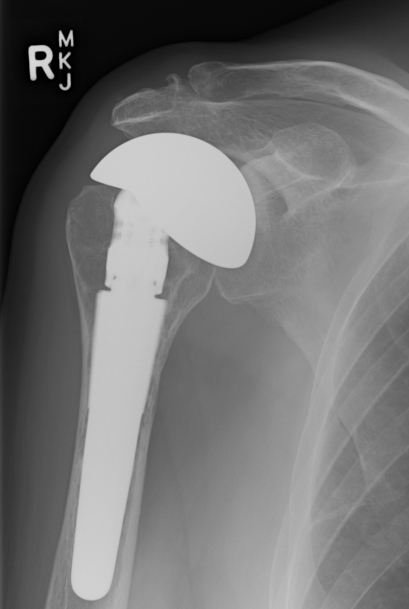
CTA humeral head
Reverse TSA
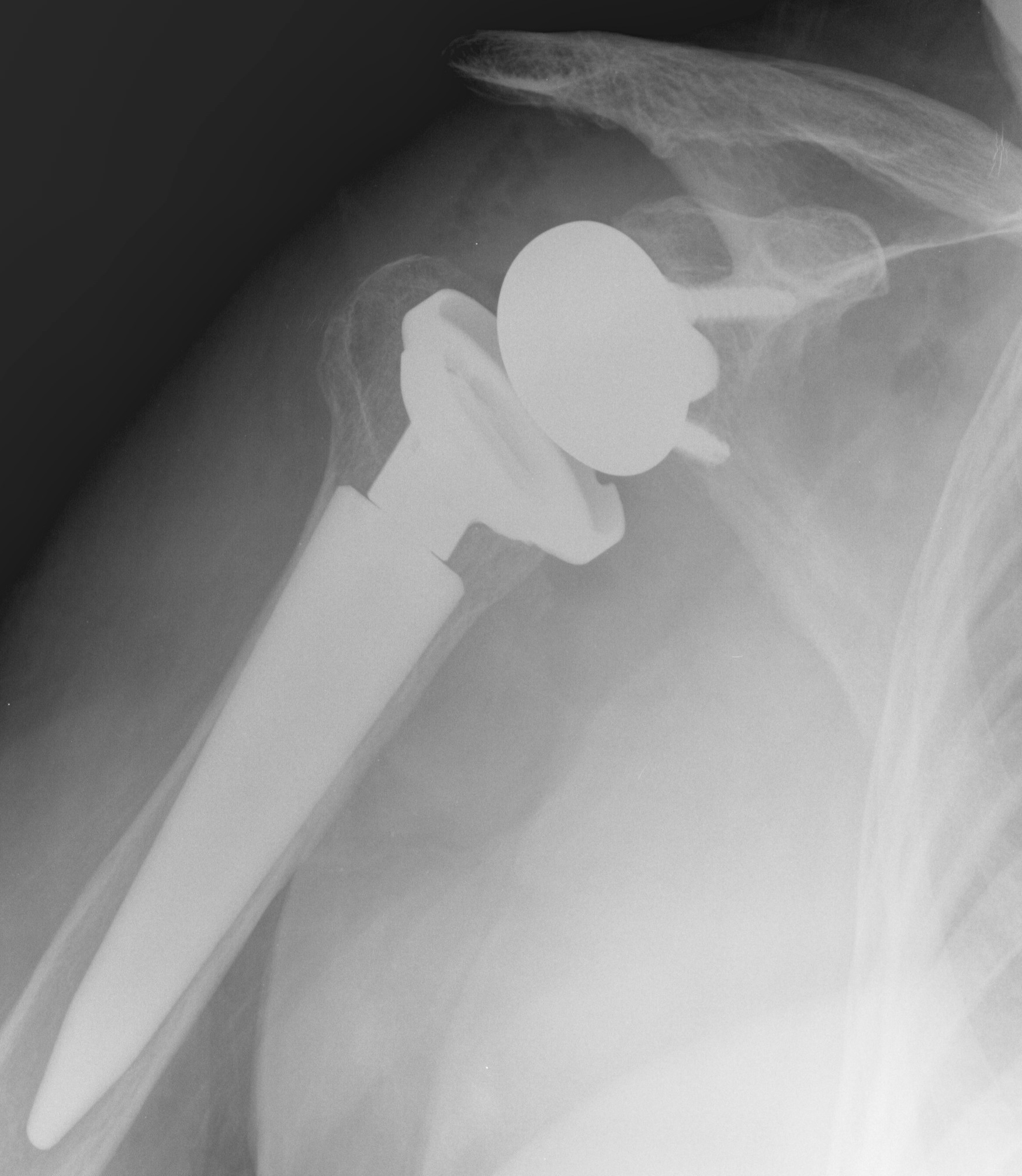
www.boneschool.com/reverse-TSA
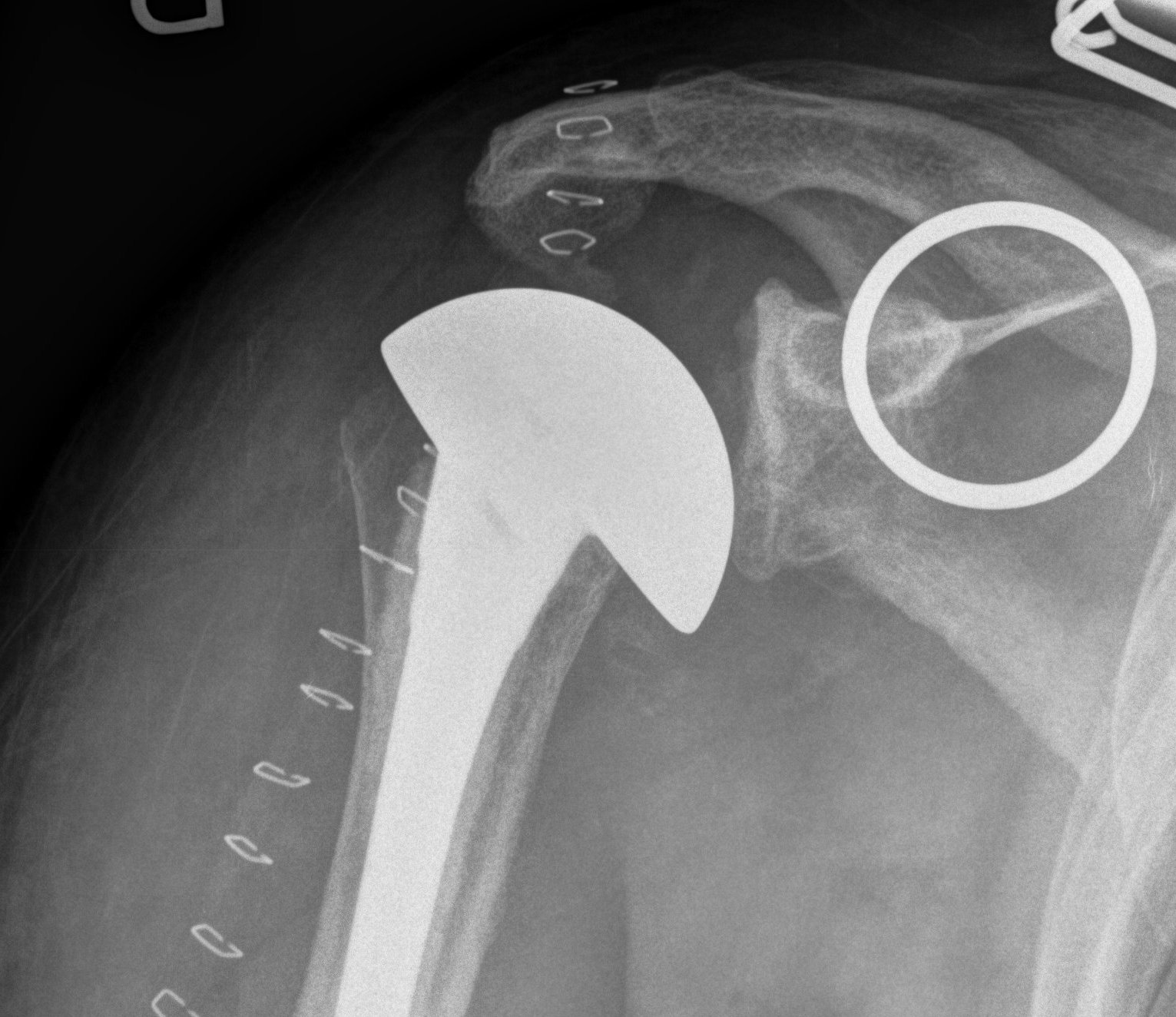
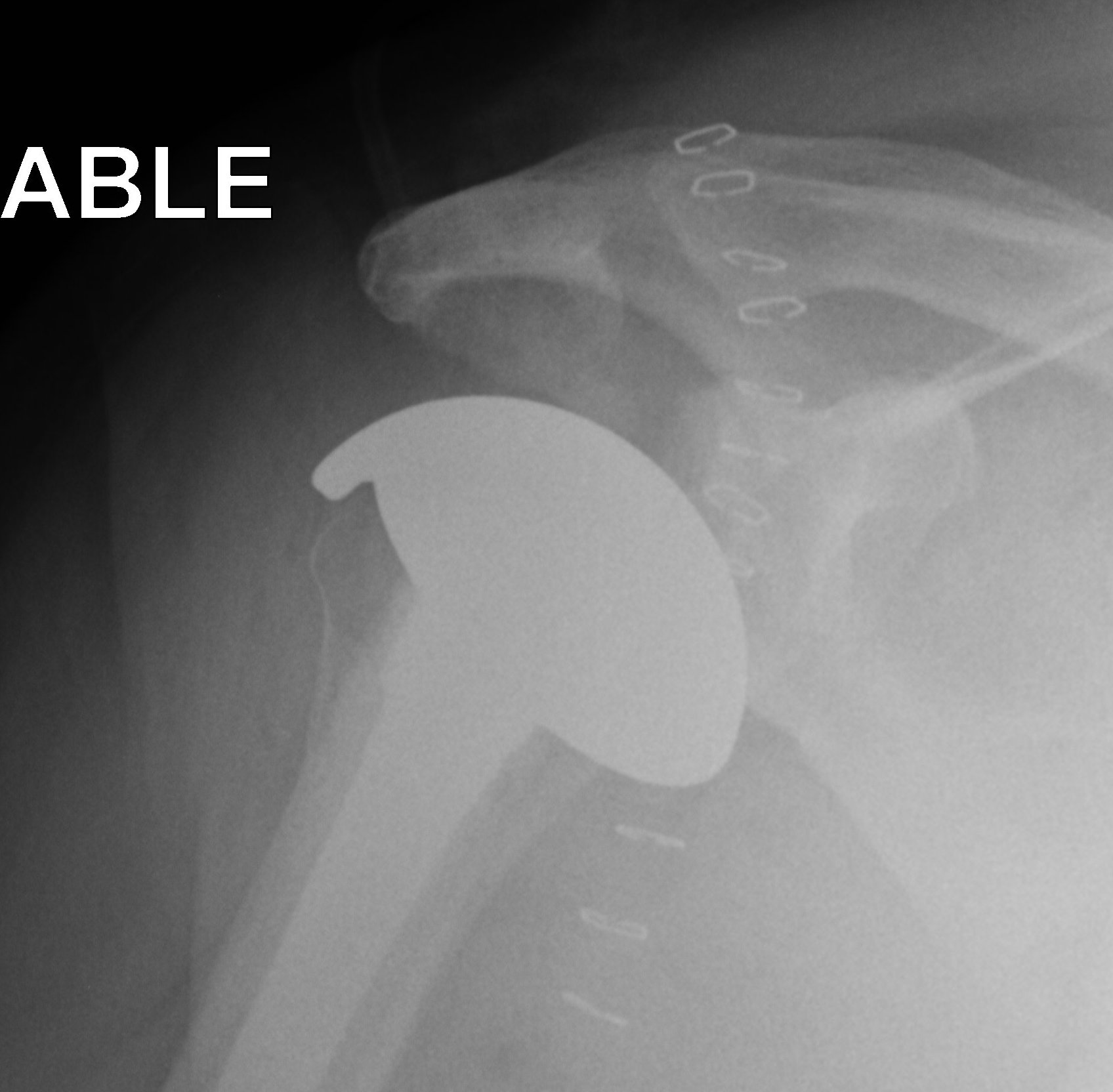
CTA Humeral Head / Extended Humeral Head Arthroplasty
Cuff Tear Arthropathy (CTA)
Extended humeral head prosthesis
- arc of surface > 180o
- allows articulation of lateral head with acromion
- increased articulation in abduction and external rotation
Indication
Young patient
Glenoid insufficiency
Revision from failed rTSA
Results
- 42 patients with 2 year follow up
- 71% able to sleep comfortably
- 86% able to use hand at shoulder height