Wrist arthroplasty
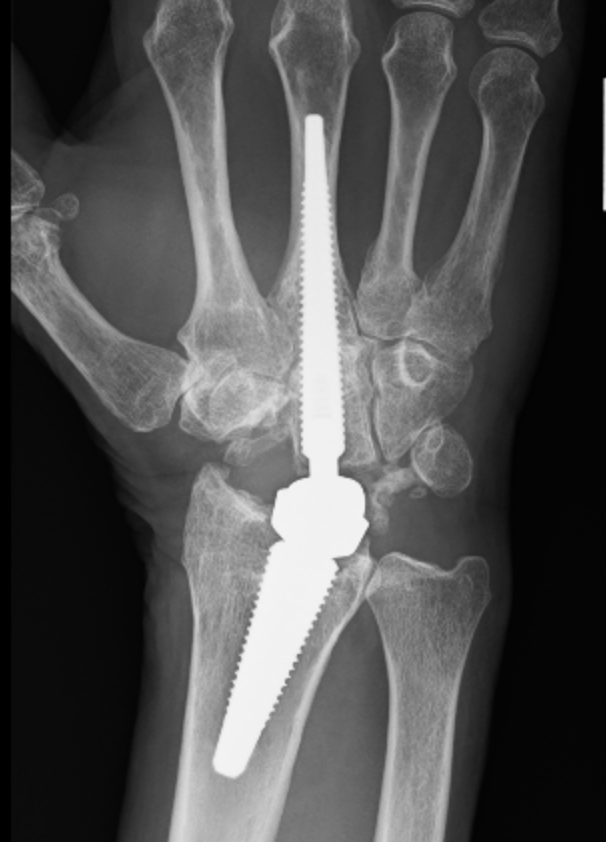
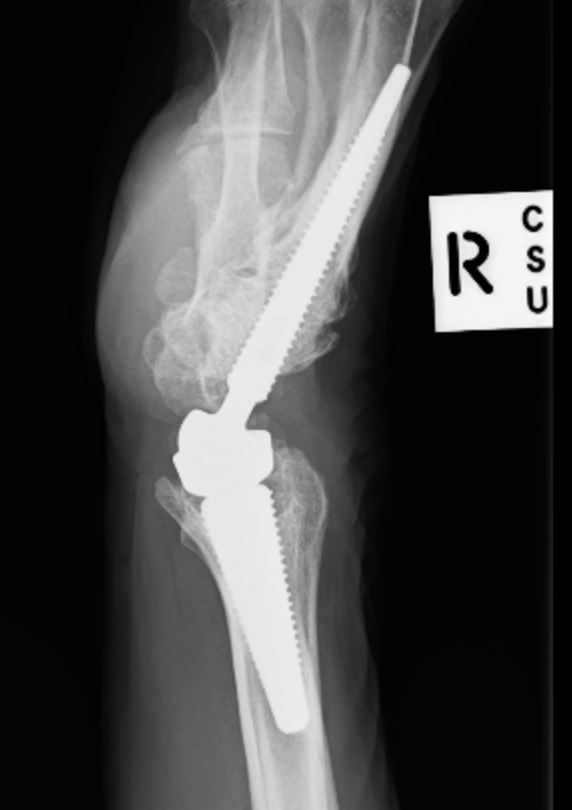
Indications


First generation (late 70s early 80s)
Results
1. Always resurface
2. Never resurface
3. Selectively resurface
Controversial
- literature divided on issue
Historically
- poor outcomes due to poor implant design
- now improved designs
- non resurfacing also improved due to better design and improved techniques in regard to tracking and rotation

1. RC arthropathy / > 70 / low functional demand
2. Revision TSR
3. Failed Hemiarthoplasty in proximal humerus fracture

Initial press fit
- implant geometry fits the cortical bone in the proximal femur
- good initial mechanical stability
Biological fixation for success
- good press fit
- minimal micromotion
- bony or fibrous tissue ingrowth or ongrowth

Optimize cement-bone interface
Cement mantle free of defects
Minimum 2 mm thickness
Femoral component centred in cement mantle
Swedish Joint Registry
Reflection All Poly / Spectron 92% 10 year
RA
- very good results
- 97% 10 year survival Coonrad-Morrey prosthesis
Other Dx
- OA / post-traumatic arthritis / nonunion
- tend to have worse survival than RA
Haemophilia
- elbow joint commonly involved
- 90% of haemophiliacs
Acute unreconstructable fracture > 60