
Mechanism
FOOSH
Variations
Neonates
- difficult vaginal delivery
Little leaguers shoulder
- stress fracture from repetitive throwing
- physeal widening / lateral physeal fragmentation or calcification
Unicameral bone cyst
Types
Metaphyseal 70%
Physeal 30%
- SHII > SHI
Issues
Great remodelling potential
Shoulder ROM compensatory
Physis
80% of longitudinal growth of the humerus
Closure
Females 16
Males 18
Deforming forces
Varus deformity most common
Neer-Horwitz Classification
Type I - < 5 mm displacement


Type II - < 1/3rd shaft width

Type III - 1/3 - 2/3rd shaft width


Type IV - > 2/3rd shaft width

Management
Nonoperative Management
Guidelines
Age Acceptable alignment
< 5 Up to 70° angulation, 100% displacement
5-12 Up to 60° angulation
> 12 Up to 40° angulation, 50% displacement
Case: 16 year old boy
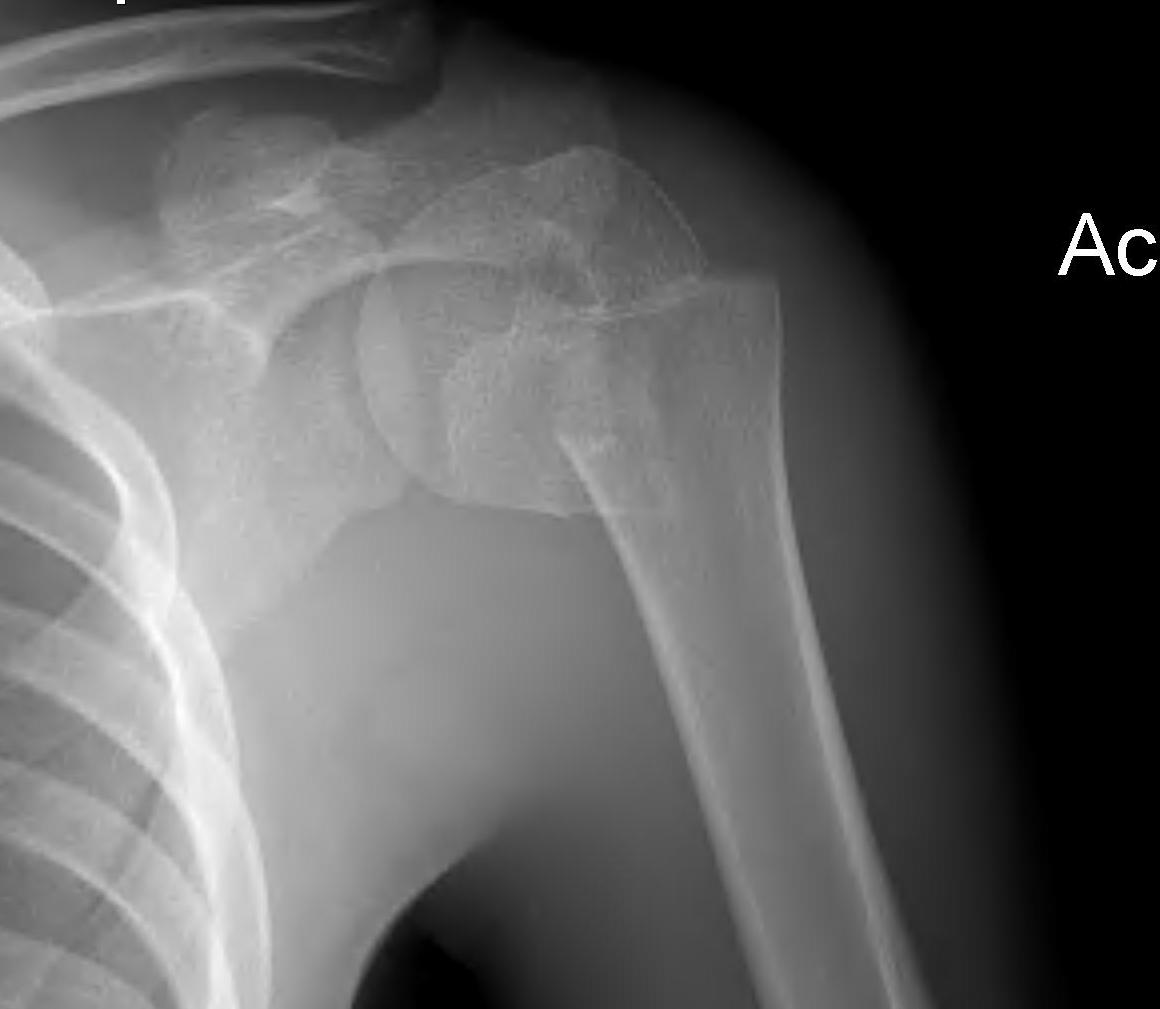

Initial injury 18 months post injury
Case: 18 year old boy

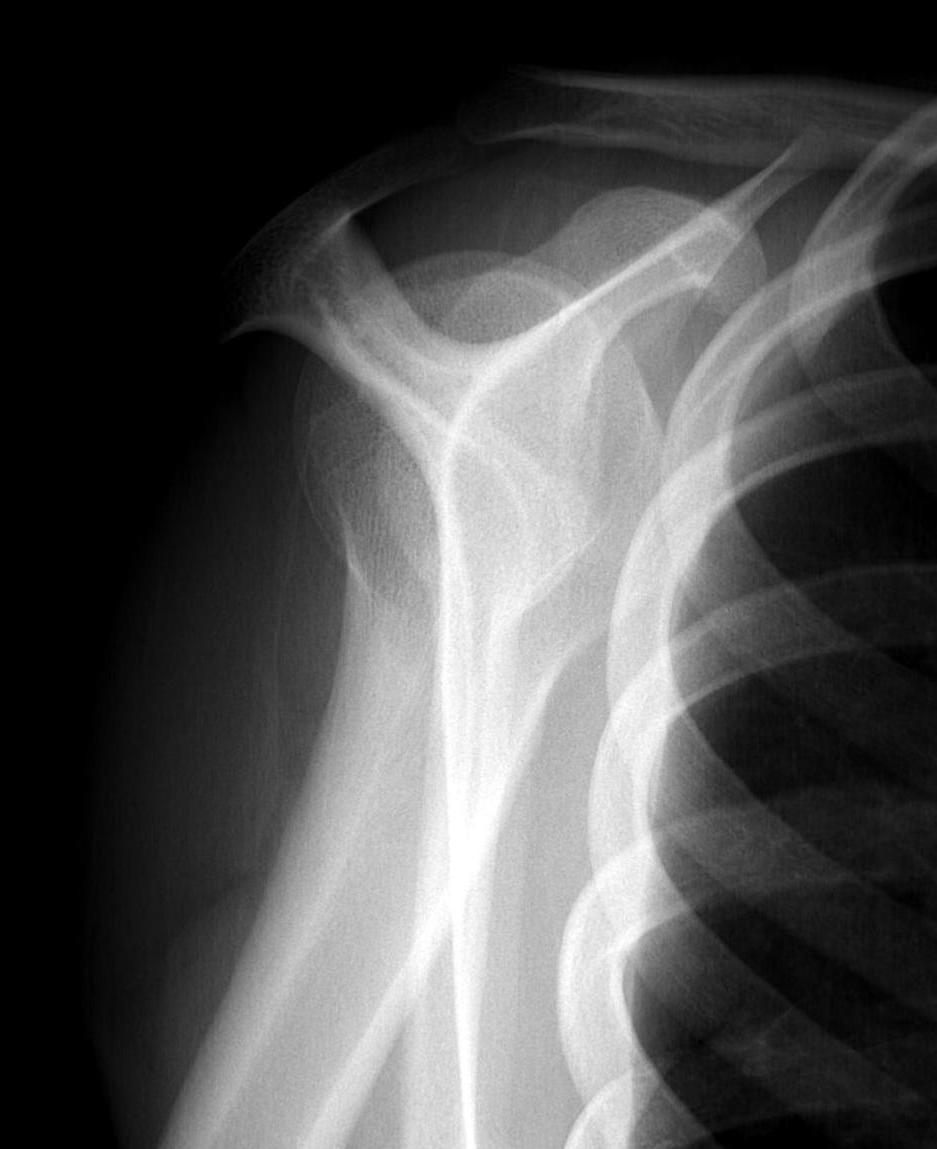
Initial xray 18 month xray
Operative Management
Indications
Unclear
- older adolescents with minimal remodelling potential
- Types III / IV
Results
- systematic review
- subgroup Neer III / IV
- good excellent outcomes: nonoperative 82%, K wire 95%, flexible nails 98%
- type Neer III / IV in juveniles
- 15 K wires, 16 flexible nails
- no difference in outcomes between two groups
Marengo et al. J Paediatr Orthop 2015
- 14 patients average age 10 years treated with retrograde flexible nails
- no loss of position, no growth arrest
Options
1. Manipulation under anaesthesia (MUA)
2. K wire / percutaneous pinning
3. Retrograde flexible nails
Open reduction
Indication
Failure of closed reduction
Pandya et al. J Child Orthop 2012
- 10 open reductions
- blocks to reduction: biceps (90%), periosteum (90%), deltoid (70%), bone fragments (10%)
Technique
- deltopectoral approach
- protect blood supply / ascending branch medial circumflex humeral
Manipulation under anesthesia
Risk loss of reduction and second surgery


Percutaneous pinning
JSJS Essential Surgical Technique
Technique
- K wires from metaphysis into head
- +/- K wire from GT down into metaphysis
- axillary nerve at risk
- begin distal
- dissect down to bone before inserting K wire


TENS
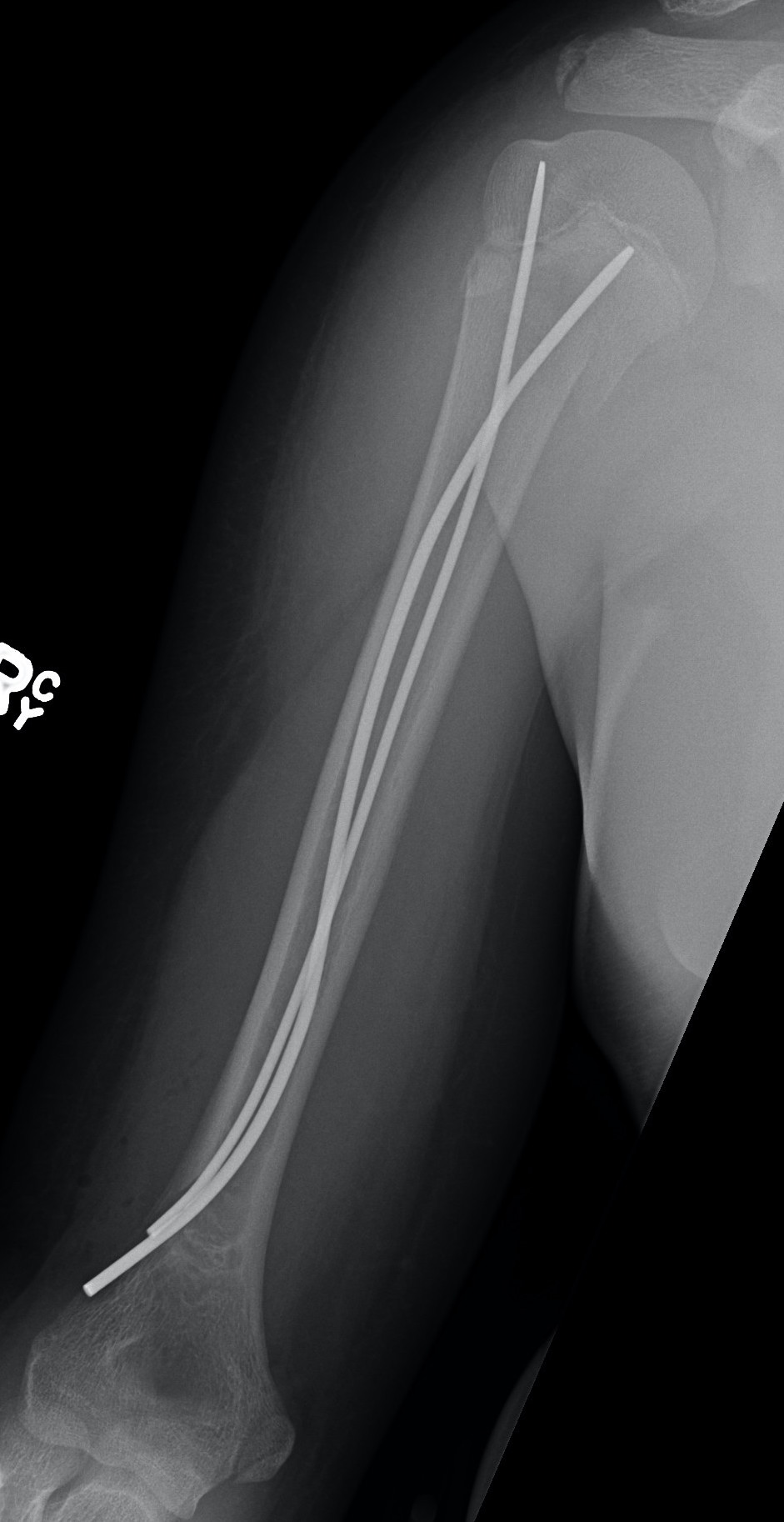

Technique
2 x drill holes in lateral supracondylar ridge
- 1 cm proximal to lateral epicondyle
- pass 2 x TENS
- standard 0.4 of diameter of bone
- usually 2.5 mm
- radial nerve at risk