



Epidemiology
20% of all pediatric fractures
School age children
50% both bone fractures
Ossification
Primary - 8 / 52 gestation radius & ulna
Secondary - distal radius age 1 / proximal radius 4 / distal ulna age 5
Growth - majority from distal physis / 75% radius / 80% ulna
Types
Single or both bone
Complete / greenstick / buckle
Galeazzi / Monteggia
www.boneschool.com/pediatrics/monteggia-fractures
Non Operative Management


Acceptable Position
< 10 years old: < 15 degrees malalignment
> 10 years old: < 10 degrees malalignment
< 1 - 2 years of growth remaining: anatomic alignment required
Operative Management
Indications
Outside parameters for non-operative treatment
Loss of reduction
Options
| Closed reduction | Compression plating | Flexible nails |
|---|---|---|
|
Patients < 10 Greenstick fractures |
Rigid anatomical fixation |
Small scars Easy to remove |
|
Large scars Plate removal - infection - nerve injury - refracture |
Non anatomical reduction Need to cast after surgery Risk to tendons at insertion Must be removed |
Results flexible nail v plate
Outcome
- meta-analysis of 13 RCTS
- IM nailing reduced operative time and complication rate compared to plate
- no difference in time to union, union rate, or loss of forearm rotation
- no difference functional outcome or time to union
- better cosmesis and shorter time to union in flexible nail
- increased radial bow with flexible nail, but did not affect outcome
Adolescents
Shah et al J Orthop Trauma 2010
- comparison of plate (46) v nail (15) for 61 adolescents average age 14
- 83% in both groups obtained full rotation
- no major complications in nail group
- 5 major complications in plate group
Refracture
Makki et al J Paediatr Orthop B 2014
- plate removal refracture rate 8.5% if removed within 12 months of implantation
- nail removal refracture rate 17% if nail removed within 6 months of implantation
Closed reduction / manipulation under anesthesia
Post reduction Positioning / Rule of Thirds
1. Fracture proximal to the insertion of Pronator Teres
Proximal fragment supinated by biceps - supinate the forearm to match proximal fragment




2. Fracture in the middle third
Midposition / neutral - biceps / pronator teres balanced




3. Fracture in the distal third
Proximal fragment pronated by pronator teres - pronation is the position of choice


Results
Jones et al J Pediatric Orthop B 1999
- 300 forearm fractures treated with closed reduction
- 7% (22/300) required remanipulation
- 4% (12/300) required surgery
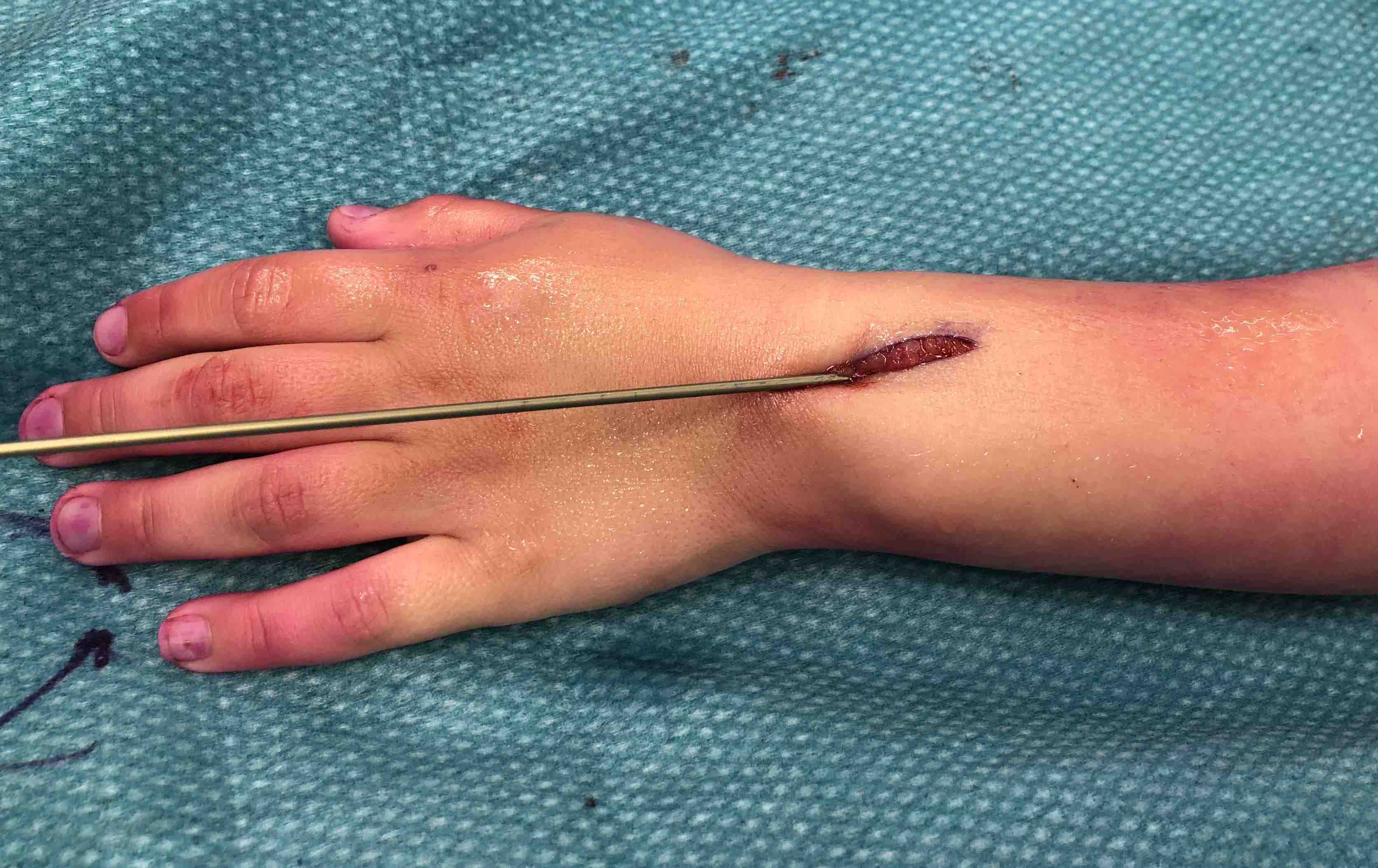
Flexible nail / TENS technique

Synthes titanium elastic nail technique PDF
AO surgery reference Radius Tens
AO surgery reference ulna Tens
Technique
Elastic nail size
- 60 - 70% of the intramedullary canal typically 1.5 - 2.5 mm
Radius
- typically first as more difficult to reduce
- entry point with awl 2 cm proximal to distal physis
- Radial styloid / distal lateral entry - ensure radial nerve / cephalic vein, 1st extensor compartment protected
- Listers tubercle / dorsal entry

Fracture reduction
- avoid passing nails incorrectly multiple times as may cause compartment syndrome
- bend tip of elastic nail
- may need small open reduction
Cut nail - withdraw 1 cm, cut with endcutter, then advance
Ulna
- usually reduced after radius fixation)
- entry point 2 cm distal to apophyseal plate
- Proximal lateral: avoids ulna nerve
- Distal medial

Postoperative
- cast in supination for 6 weeks to tighten interosseous membrane
- removal of TENS at after 6 months once osseous union established



Progression on complete healing on xray prior to nail removal
Results
Refracture
Tsukamoto et al Eur J Surg Traumatol 2020
- 60 patient treated with both bone flexible nails
- 10% refracture with falling or sports activities
- all evidence of immature healing before nails removed
Ulna nail only
Dietz et al. J Pediatr Orthop 2010
- retrospective review of 38 children with both bone forearm fractures
- treated only with ulna elastic nail
- all patients had union with restoration of rotation
- two patients had angulation of the radius > 20 degrees that underwent surgical intervention
Extensor tendon injuries with elastic nails
- 202 elastic nails
- 3/202 (1.5%) EPL ruptures
Murphy et al J Pediatr Orthop 2019
- systematic review of 33 EPL ruptures post elastic nail
- all with dorsal approach to the radius
- average 10 weeks post surgery
- treated with repair, EIP to EPL transfer, or graft reconstruction with palmeris longus
Nonunion


Fernandez et al J Paediatr Orthop 2009
- 592 patients treated with elastic nail
- 6/592 (1%) nonunion / pseudoarthrosis
- all in ulna, 5/6 opened in surgery to facilitate nail passage
Compartment syndrome
Martus et al J Paediatr Orthop 2013
- 205 fractures treated with elastic nail
- 3/205 (1.5%) compartment syndrome
ORIF with plates



AO surgery Henry approach to radius
AO surgery compression plating technique
Results
Plate removal and refracture
- 82 children with retained forearm plates followed for 8 years
- 7% incidence of implant related fractures
Yao et al Arch Orthop Trauma Surg 2014
- 122 patients treated with forearm plate
- plate removal: refracture 13% (low energy trauma)
- plate retention: refracture 3% (high energy trauma)
Single versus Double plate
- RCT of 100 patients with both bone forearm fractures
- ulna plating versus ulna & radius plating
- no difference in outcome, range of motion or union rates
- some loss of position in radius when not plated