


Background
Non walking age child
Failure of splint treatment during first 6 months of life
Late presenters
Clinical signs
Unilateral hip dislocation - decreased abduction / apparently short femur
Bilateral - more difficult, symmetrical decrease of abduction
Xray
Findings
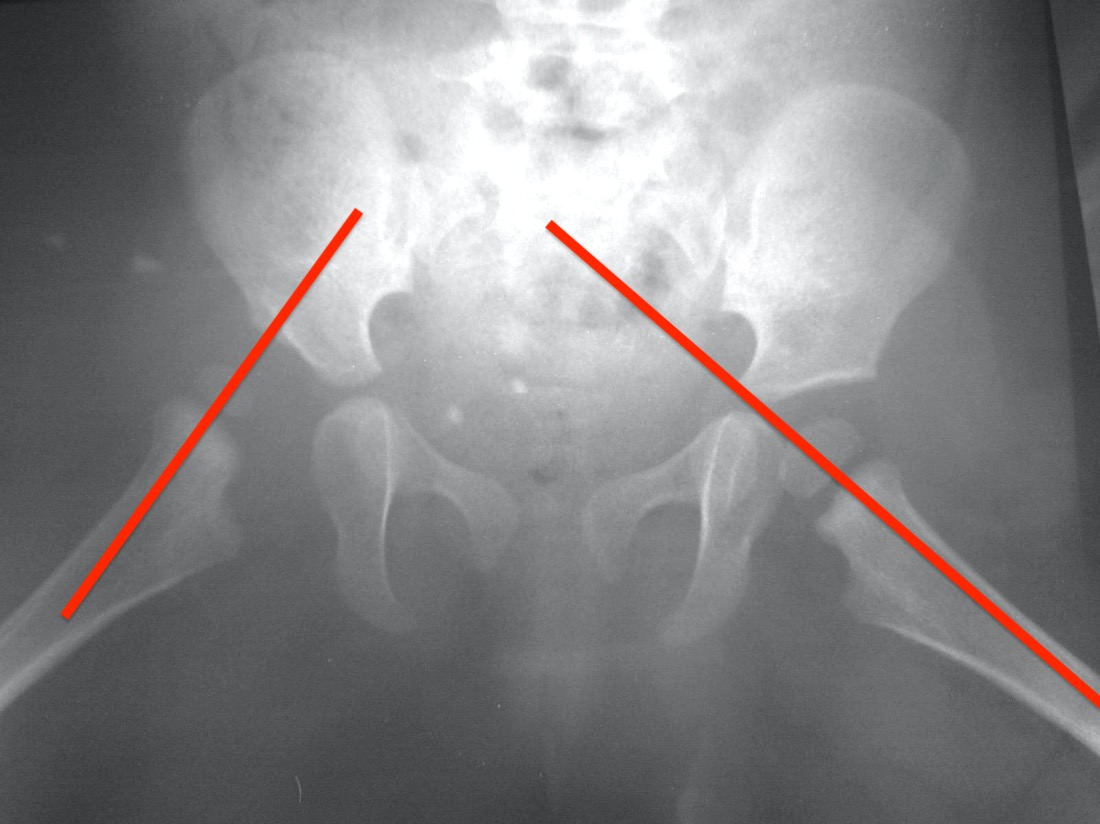
Small femoral epiphysis
Femoral epipysis in upper outer quadrant
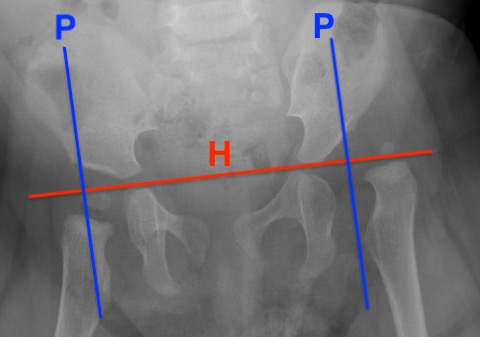
Disrupted Shenton's line
Increased acetabular index > 35°
Von Rosen view - hip not reduced

Dislocated hip with SFE in upper / outer quadrant

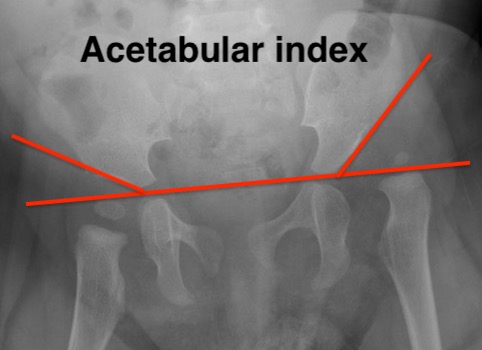
Dislocated hip with disruption of Shenton's line and increased acetabular index

Failure of the hip to reduce on von Rosen view
Management
Options
A. Adductor tenotomy + closed reduction
- able to reduce hip
- within safe zone of abduction to avoid AVN
B. Open reduction
- for failure of closed reduction
Timing
When safe for anaesthetic
Generally 6 - 12 months of age
Adductor Tenotomy / Closed reduction
Technique
Vumedi closed reduction adductor tenotomy and hip spica video
General anesthesia + percutaneous adductor tenotomy
- reduce hip with abduction and flexion
Ramsey's safe zone
- has to be at least 20° between re-dislocation & maximum abduction
- abduction < 50o / flexion 90o
- anything more has high risk of AVN
Arthrogram to confirm head reduced
- fluoroscopy
- spinal needle with 10 mls contrast
- anterior approach: 2.5 cm below ASIS, 45° angle to femoral head / neck junction
- medial approach: needle inferior to adductor longus tendon to inferior aspect of neck just below head
Abnormal hip
- widened medial joint space / medial pooling < 5 - 7 mm

Apply hip spica
- 3 months duration
- may need to change at 6 weeks due to child growth
Reduction assessment

Options
- xray
- ultrasound
- CT - irradiation risks
- MRI
- 136 DDH treated with closed or open reduction
- ultrasound more accurate than xray
MRI
- MRI post closed reduction in 92 hips
- one initial and one at end of spica treatment
- labrum initially inverted in 92% of hips
- labrum everted in 50% at end of cast treatment


MRI showing excellent reduction of the left femoral head despite closed reduction and application of spica
MRI showing continued subluxation of the left femoral head despite closed reduction and application of spica
Results


Successful closed reduction over time
Outcomes
Li et al J Pediatr Orthop B 2019
- closed reduction in 440 hips
- failure 8%
- rate AVN 14%
- preoperative traction had no effect
Domos et al EFORT Open Rev 2024
- systematic review of 3800 DDH treated with closed reduction
- overall failure 20%
- higher grade dislocation and male age risks factors for failure
- closed reduction in 250 hips
- increased success with age < 12 months
AVN
Schur et al J Child Orthop 2016
- closed reduction in 82 hips
- AVN 35%
- reduced AVN with abduction < 50°
Bradley et al J Child Orthop 2016
- systematic review of closed reduction in 538 hips
- AVN 10% at mean 7 years
Open Reduction
Indication
Irreducible hip on adductor tenotomy / closed reduction
Unstable outside of Ramsey safe zone
Widening of medial joint space on arthrogram
5 Blocks to reduction
1. Capsule / psoas tendon
2. Inverted or thickened labrum
3. Thickened ligamentum teres
4. Inverted inferior transverse ligament
5. Pulvinar / thickened medial acetabular fat
Surgical Options
Medial / Ludloff approach
Anterior / Smith-Petersen approach
+/- pelvic or femoral osteotomy if > 1 year old
| Medial approach | Anterior approach |
|---|---|
|
Risk of AVN from damage to MCFA
|
Larger dissection with more blood loss More difficult releases medial and inferior |
|
Direct approach to adductor and psoas tendon Cannot perform capsulorraphy
|
Can perform capsulorraphy Can perform pelvic osteotomy |
|
Under 12 months of age
|
Older than 12 months |
Medial versus anterior approach
- systematic review of medial versus anterior approach
- open reduction of DDH under 2 years of age
- 5 comparative studies with 257 patients
- no difference in clinical outcomes
Medial approach
Technique

POSNA academy medial approach to DDH video
Supine with hips abducted and flexed
- landmarks adductor longus and pubic tubercle
- 3 - 4 cm incision in groin crease over adductor longus
- open fascia over adductor longus in line with tendon
- release adductor longus
Intervals
- Weinstein: between pectineus and NV bundle
- Ludloff medial approach: interval between pectineus and adductor longus / brevis
- Ferguson: superficial between adductor longus anterior and gracilis / deep between adductor brevis and magnus
Identify and protect MCFA on the capsule
- identify lesser tuberosity and psoas tendon and divide psoas tendon
- T shaped capsulotomy
- release ligamentum teres from femoral head and excise
- release transverse ligament / remove pulvinar
Assess reduction with xray / arthrogram
Apply hip spica
Smith Petersen approach
Technique
Vumedi open reduction DDH Smith Peterson video
Consider supplementary medial approach
- release adductor tendon and psoas tendon
Anterior approach
- bikini incision below ASIS and parallel to inguinal ligament
- avoid crossing thigh crease
- split iliac apophysis
- identify and protect lateral femoral cutaneous nerve on sartorius
- interval between sartorius and TFL
- interval between rectus femoris and gluteus medius
- retract sartorius and rectus medially +/- tag and release rectus
- T shaped capsulotomy
Release
- ligamentum teres from femoral head and completely excise it
- sublux femoral head from acetabulum
- resect pulvinar / medial fatty tissue
- divide transverse ligament
- identify and protect labrum
Reduction of femoral head + capsulorraphy
Repair split in iliac apophysis
Apply hip spica