

Definition
Acute dislocation of the atlanto-axial facet joint
Present with acute torticollis
Etiology
Children
1. Post trauma - can be minor
- due to horizontal orientation of facet joints
- ligamentous laxity
- weak neck muscles
- relatively large head
2. Grisel's syndrome
- non traumatic
- post nasopharyngeal inflammation / infection
- hypothesised to be due to lymphatic swelling
3. Post ear / nose / throat surgery
Adults involved in trauma
- low incidence of neurological injury
- 44 children, mean age 9
- 21 (48%) related to previous infection / Grisel's sydrome
- 19 (43%) related to minor trauma
- 4 (9%) unknown cause
- delayed diagnosis common (mean presentation 178 days)
Examination
Cock Robin position
- the chin tilted to one side
the neck flexed laterally to the other
Torticollis
Myelopathy - gait disturbance, neurological deficits
DDx
Fibrosis sternocleidomastoid - chronic torticollis
Ondontoid fracture
Os ondontoid
Xray
Open mouth xray
Lateral mass C1 rotated & asymmetric
Wink Sign - C1 facet locked over C2
CT Scan
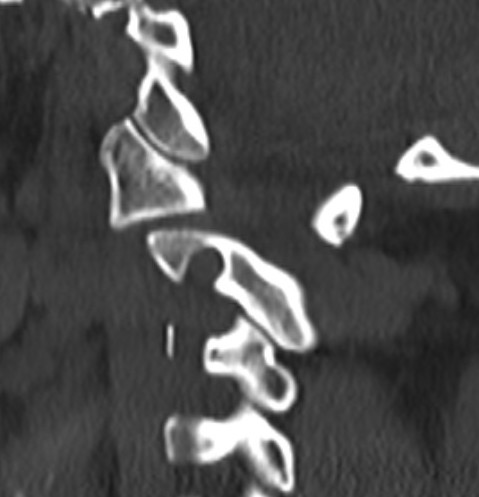
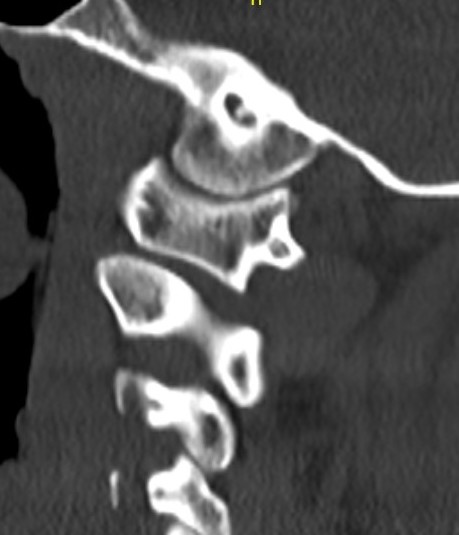
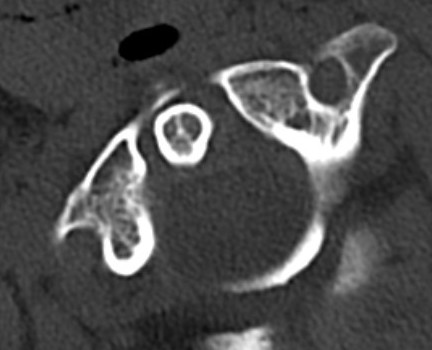
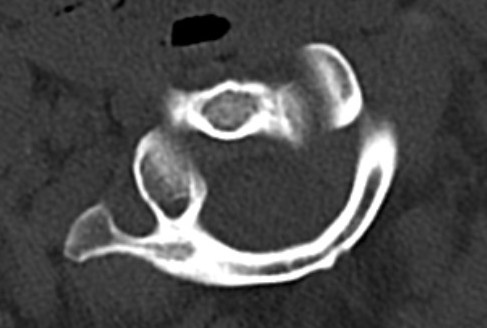
Atlanto-axial rotatory instability

Classification Fielding & Hawkins
| Type I |
Unilateral facet subluxation / dislocation ADI < 3 mm |
Transverse ligament intact | Most common |
| Type II |
Unilateral facet subluxation / dislocation Anterior displacement of the atlas by 3–5 mm ADI 3 - 5 mm |
Transverse ligament injury | |
| Type III |
Bilateral facet subluxation / dislocation Anterior displacement of atlas by more than 5 mm ADI > 5 mm |
Alar and tranverse ligament deficient Both lateral masses displaced anteriorly |
|
| Type IV | Posterior displacement of atlas | Ondontoid process deficient or fractured |
Rare Highest risk of neurological injury |
Management
Closed reduction
Admit
- bed rest
- NSAIDS / muscle relaxants
Options
- hard collar
- halter traction
- cervical traction
- reduction under GA
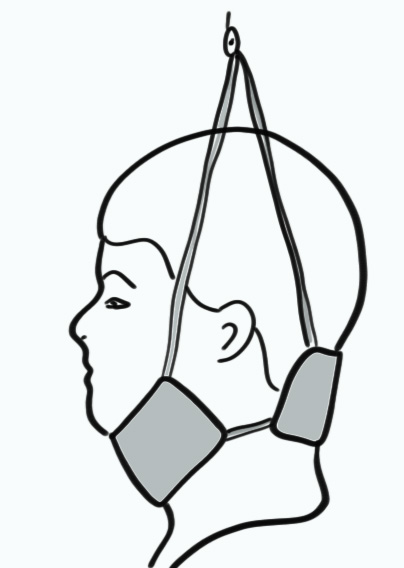
Halter traction
Results
- 7 patients with torticollis > 5 months duration
- closed reduction under GA then Halo-Thoracic Brace (HTB) 3 months
- no failures
Beier et al J Neurosurg Pediatr 2012
- 40 cases average age 8
- range of time periods since onset torticollis
- half successfully reduced with cervical collar
- remainder treated with halter traction or HTB
- 3 cases required operative fusion
- 43 patients mean age 8 average 3 months post onset of symptoms
- halter traction successful in 42/43 (98%) with average treatment 18 days
- 1 recurrence successfully treated with repeat halter traction
Open reduction
Indication
- failed closed reduction
- bony fusion / anatomical changes
Open reduction and posterior fusion
- cervical traction
- neurological monitoring
- care with vertebral artery
- reduction via anterior (trans-oral) or posterior approach
- posterior C1-C2 fusion
Posterior C1-C2 arthrodesis
1. Sublaminar wires - Gallie / Brooks
2. Pedicle screws
- C1 lateral mass C2 pedicle screws (Goel-Harms)
- trans-articular screws C1 C2 (Magerl)
Results
- 32 children with AARI > 6 weeks
- average 6 months of torticollis
- 8/32 (25%) had neurological symptoms
- half reducible with traction, posterior fusion
- half required trans-oral reduction and posterior fusion
- 31/32 (97%) had solid fusion
- 1 required revision due to recurrent torticollis