Scenarios
1. Isolated LCL injury
2. Isolated Posterolateral Corner
3. PCL + posterolateral corner
4. ACL / posterolateral corner
5. ACL / PCL / posterolateral corner
Repair versus Reconstruction Posterolateral Corner
Levy et al. Am J Sports Med 2010
- failure in 4/10 knees treated with acute primary repair
- failure in 1/18 knees treated with reconstruction
Stannard et al. Am J Sports Med 2005
- acute primary repair on 35 patients, with 37% failure at 2 years
- primary reconstruction on 22 patients, with 9% failure at 2 years
Geeslin et al. Am J Sports Med 2016
- systematic review of treatment of acute posterolateral corner injuries
- 134 patients
- overall, 81% achieved objective stability
- repair with staged reconstruction resulted in 38% failures
- early reconstruction +/- repair resulted in 9% failures
Takeaway message
- the ligaments stretch before becoming avulsed
- reasonable evidence that repair only more likely to fail
Repair
Indications
- femoral avulsion of popliteus / LCL
- fibular head avulsion of LCL / biceps femoris
- fibular head bony avulsion of LCL / biceps femoris
Timing
- need to do 2 - 3 weeks post injury to identify structures
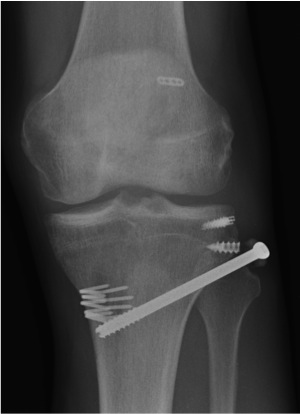
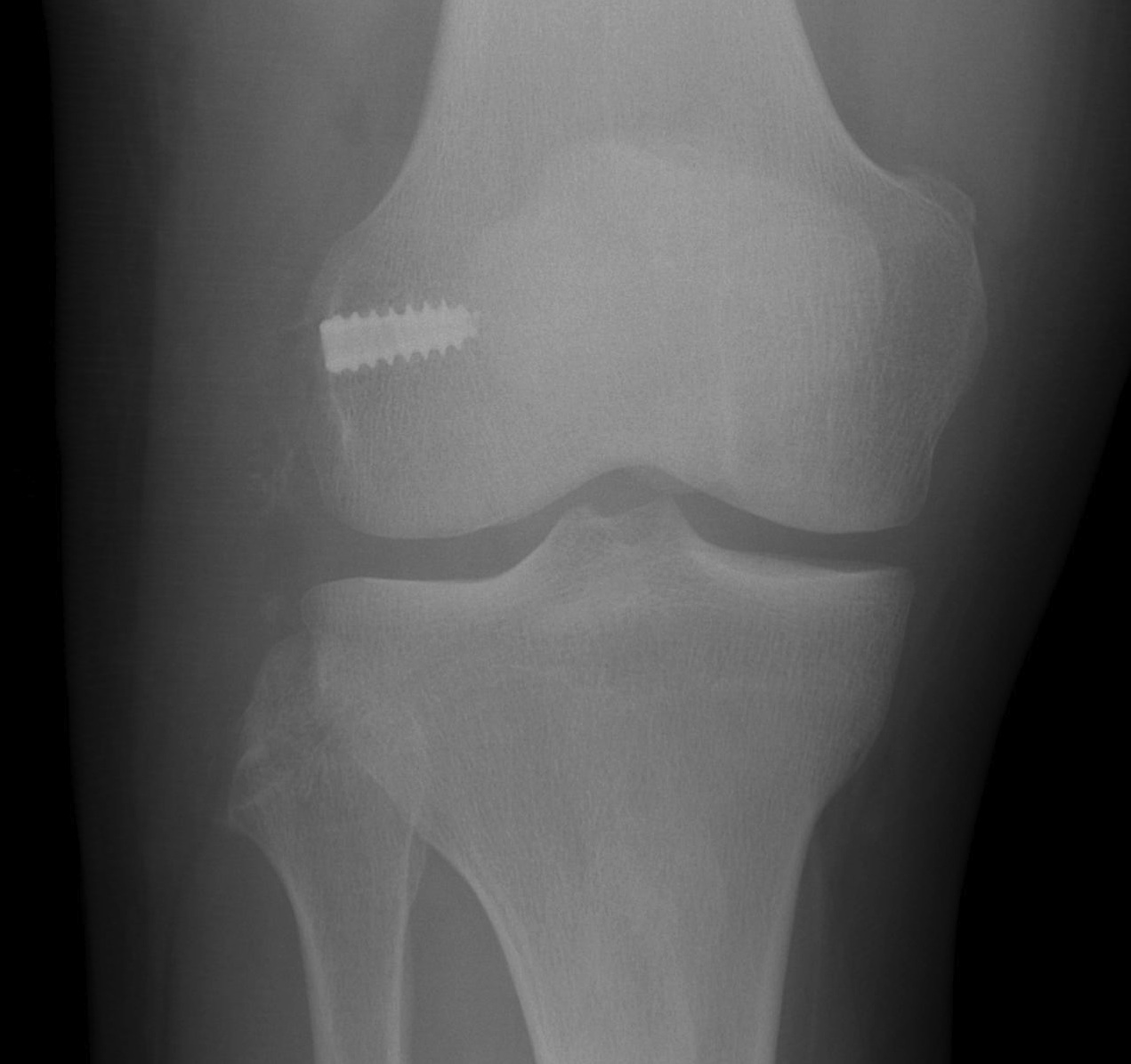
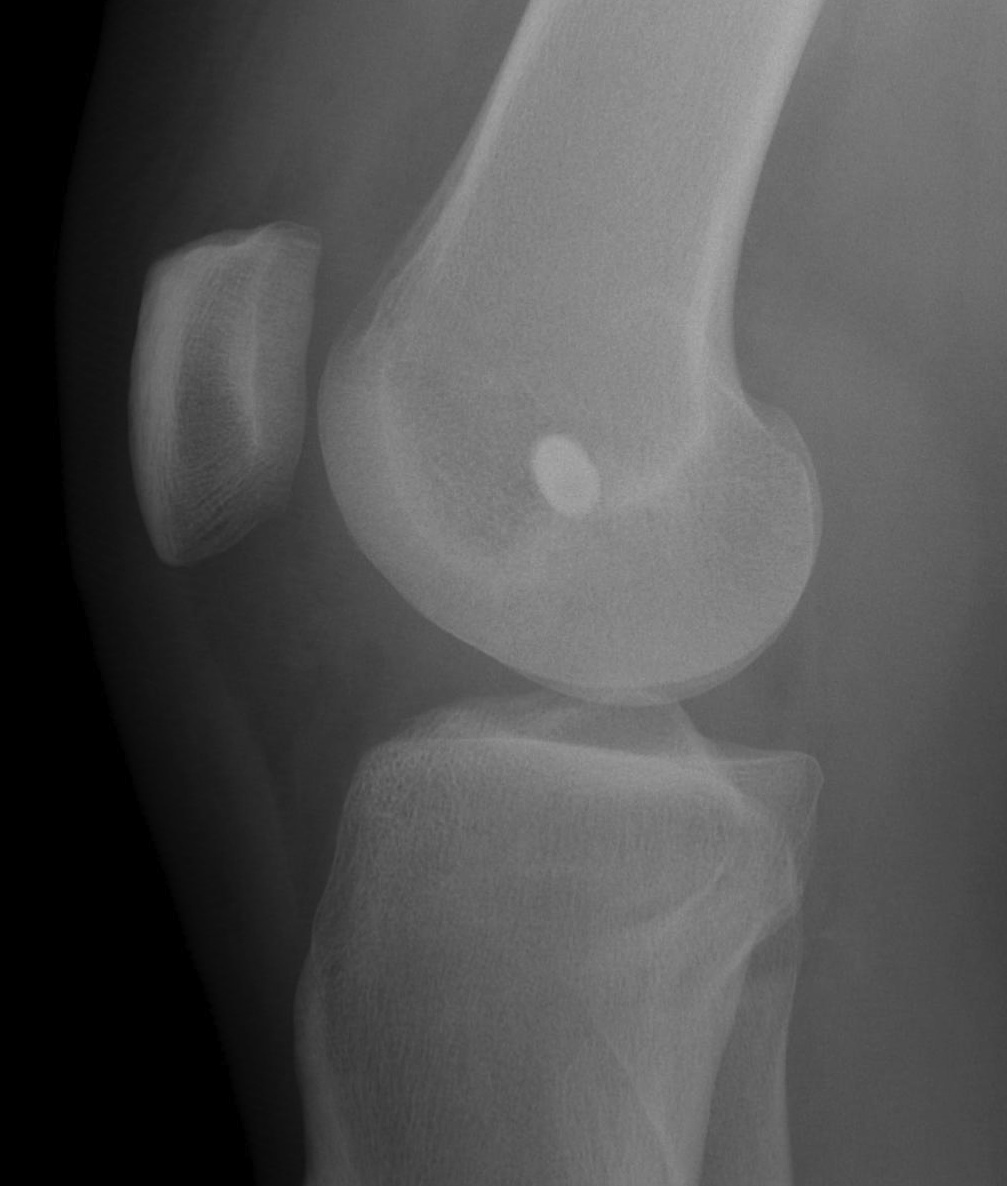
Acute fixation of bony avulsion of fibula with screw
Technique
- anchor repair of femoral or fibular avulsion
- screw fixation of bony fibular avulsion into tibia if piece large enough
- typically back up with reconstruction
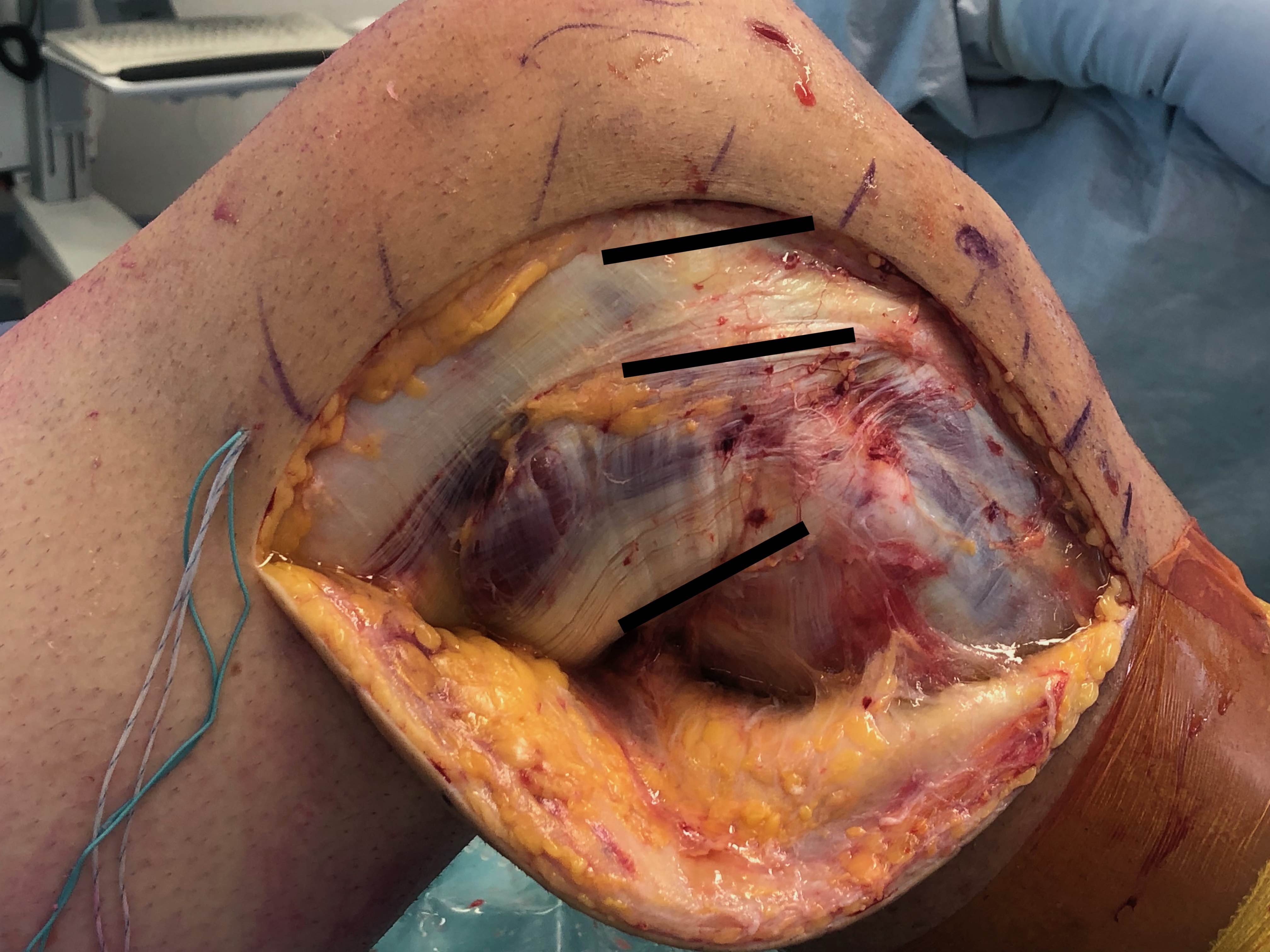
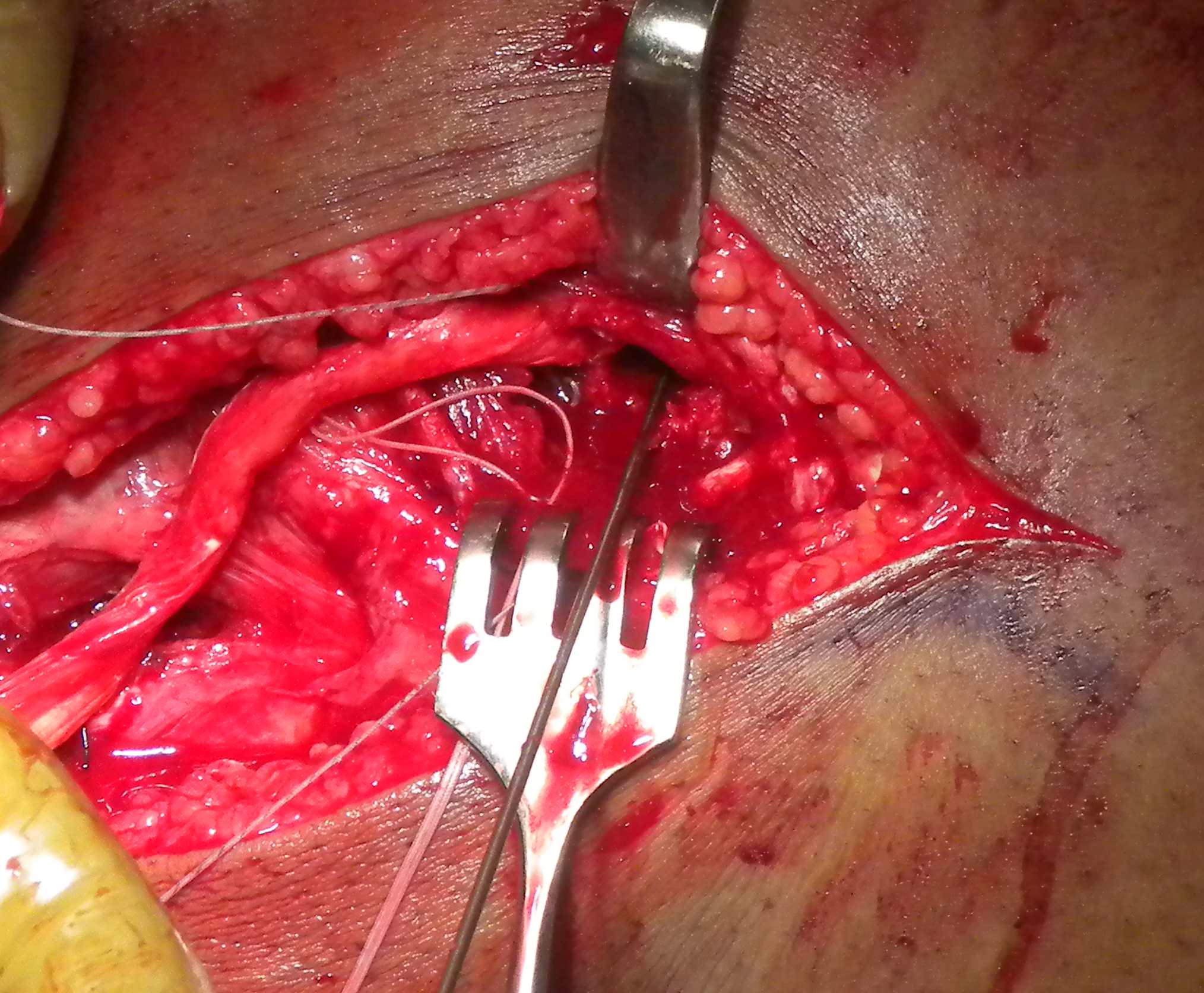
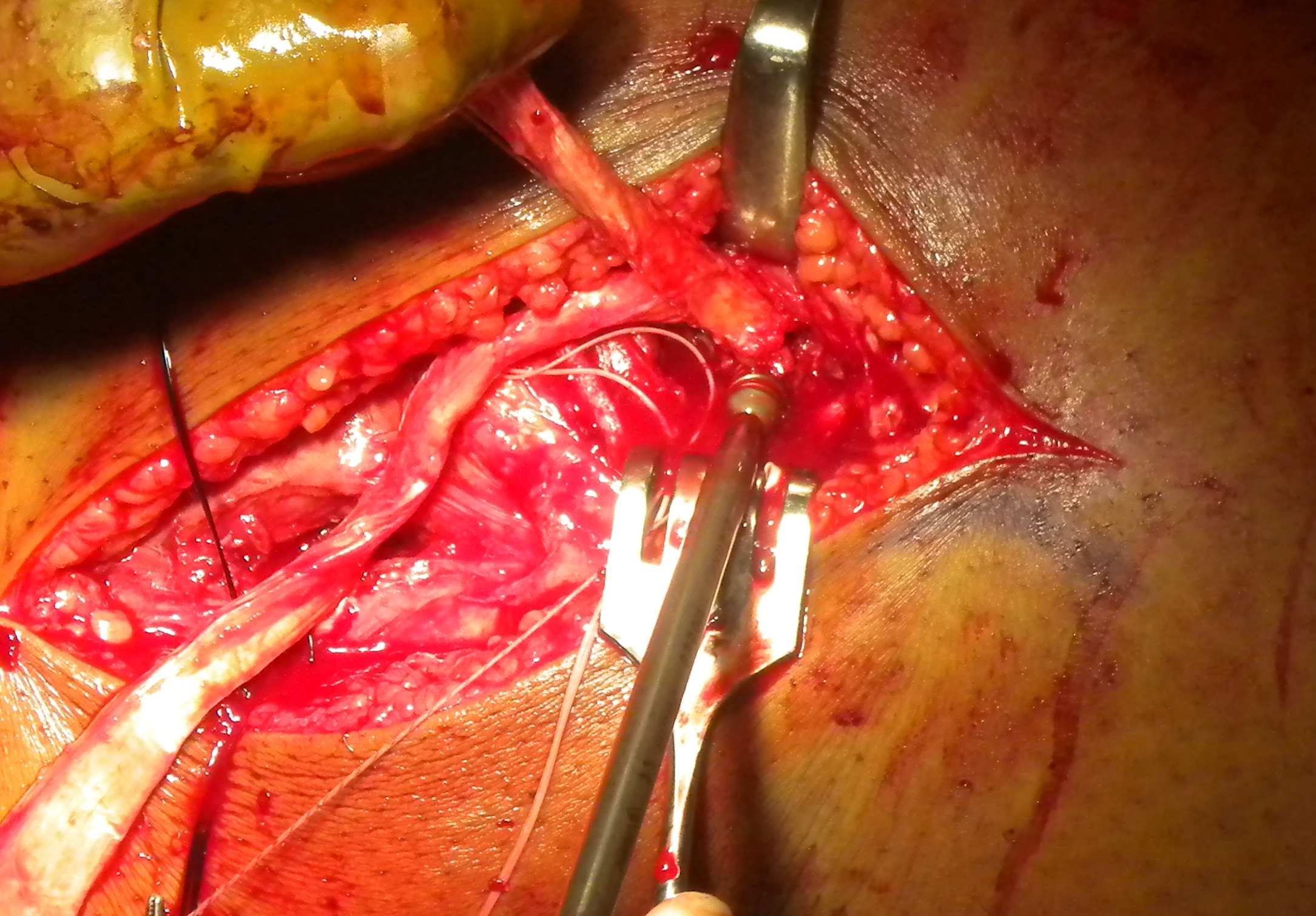
Surgical approach to posterolateral corner
Position
Supine with sandbag under buttock
- knee flexed 90°
- radiolucent table
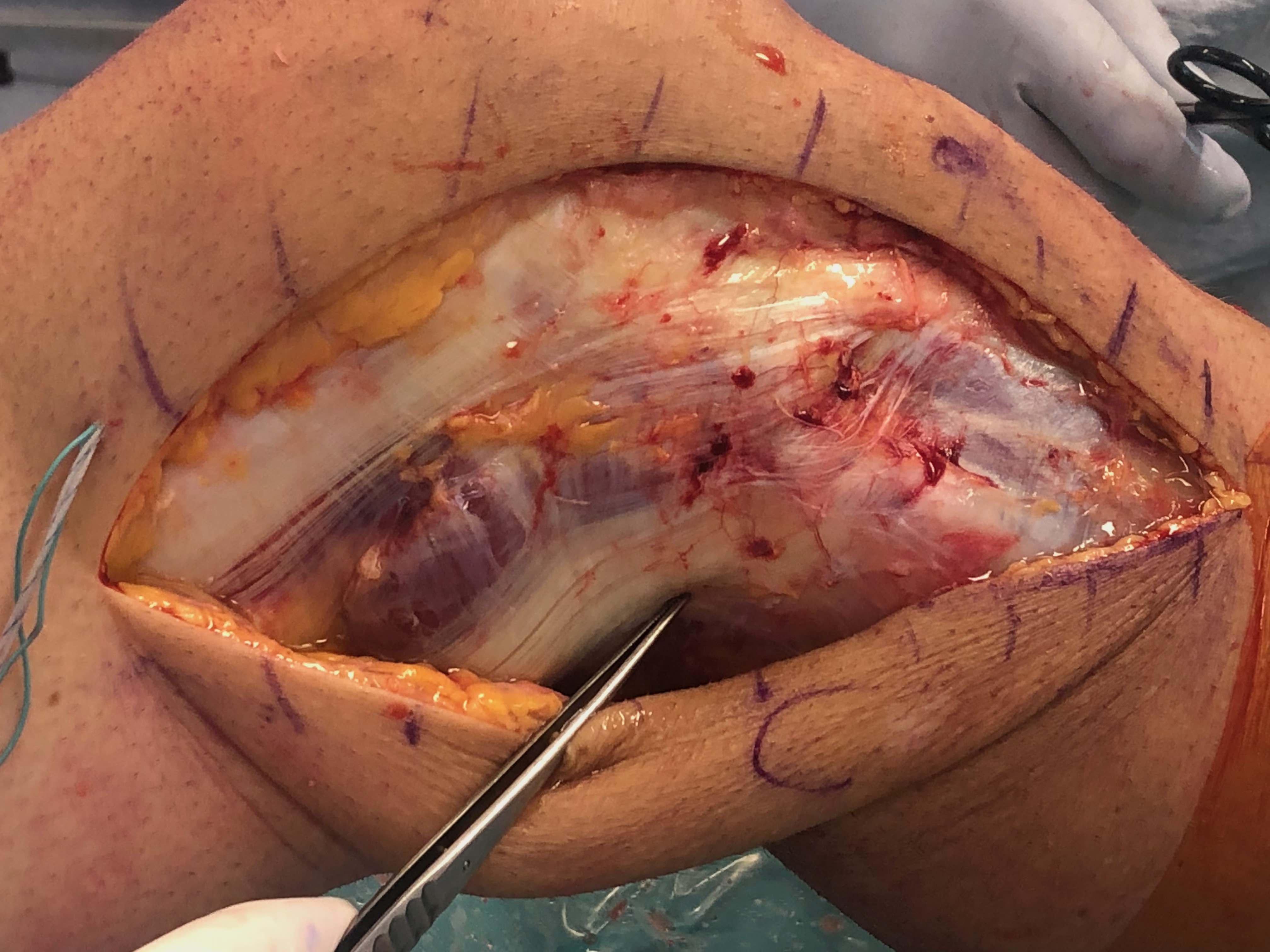
Incision
Landmarks
- Gerdy's tubercle and midpoint femoral condyles
- long curved incision centred over Gerdy's tubercle
- clear subcutaneous fascia down to ITB
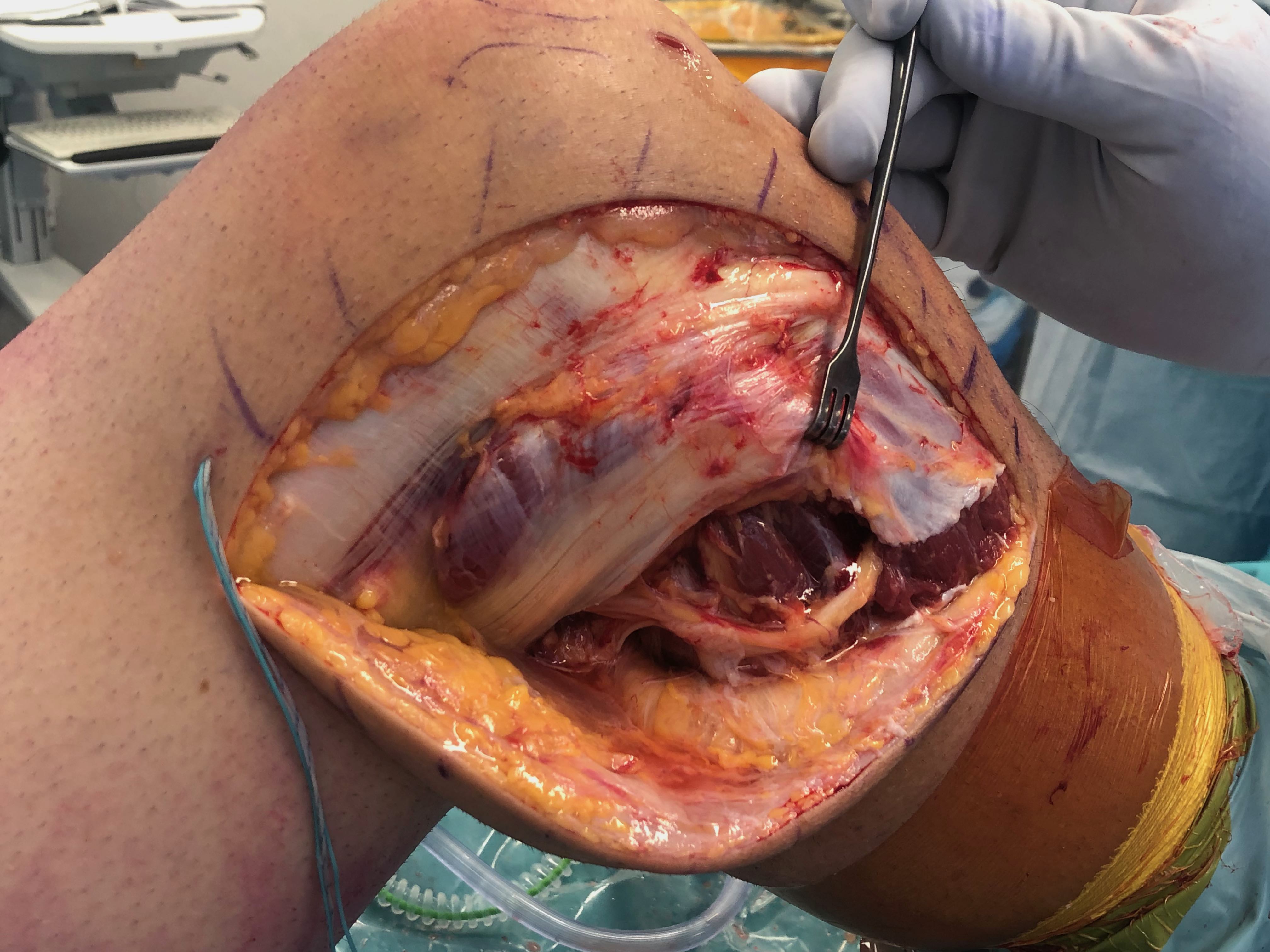
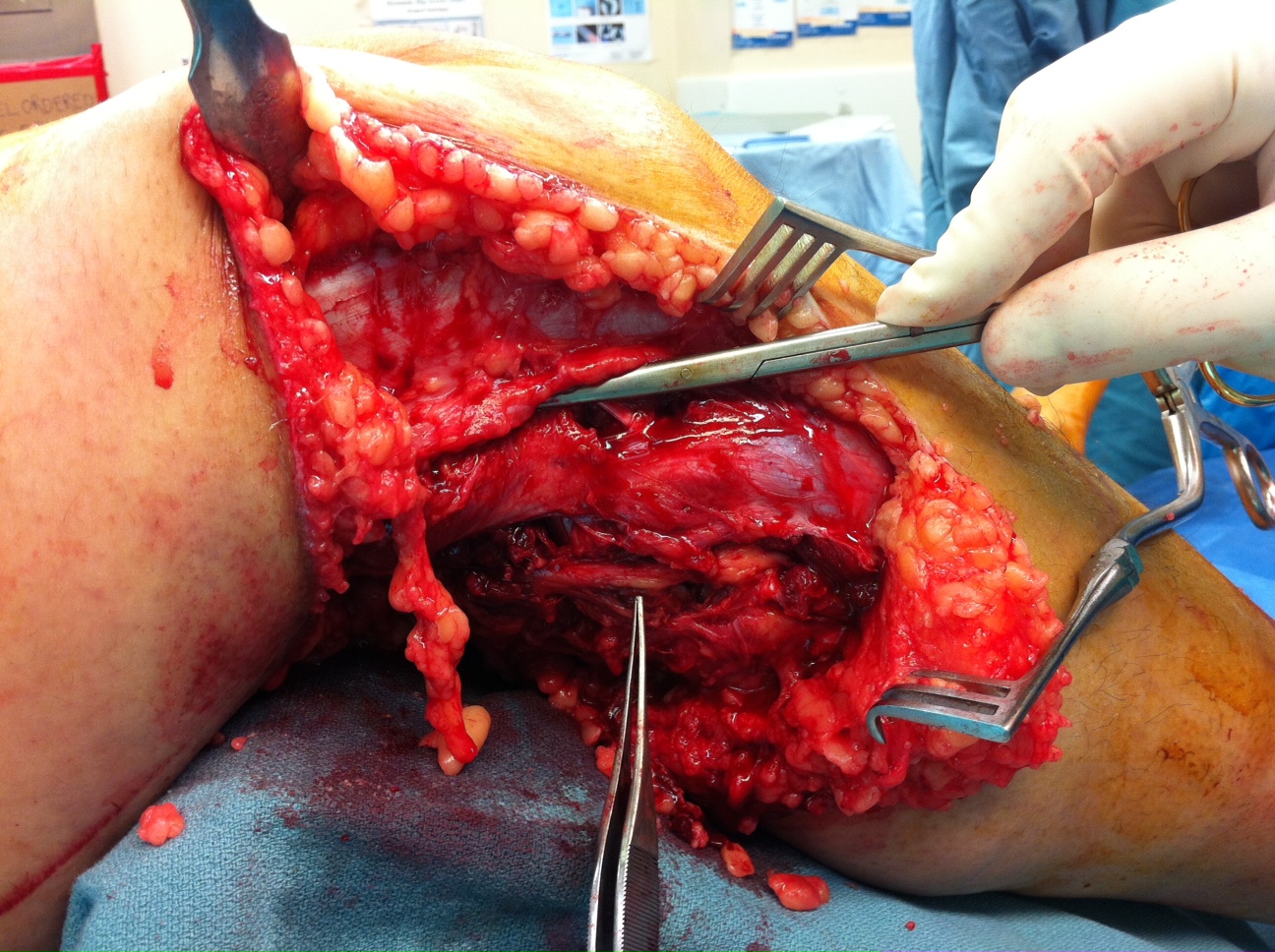
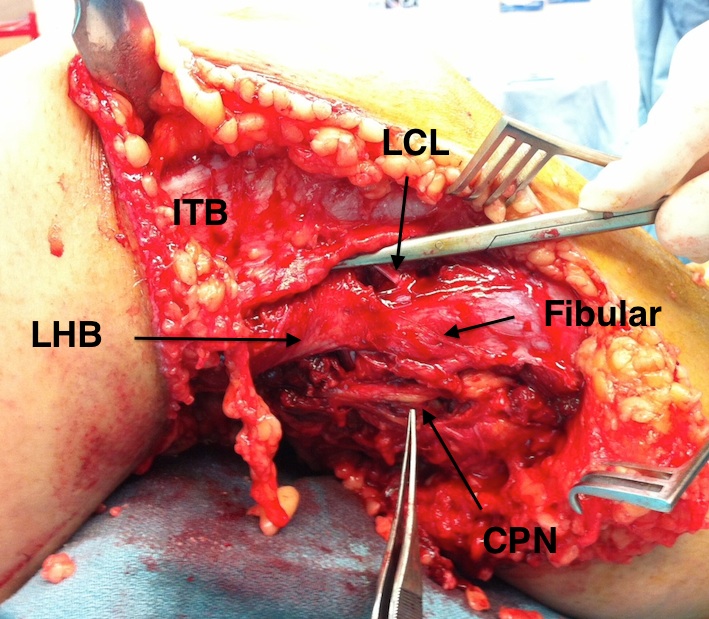
3 fascial windows
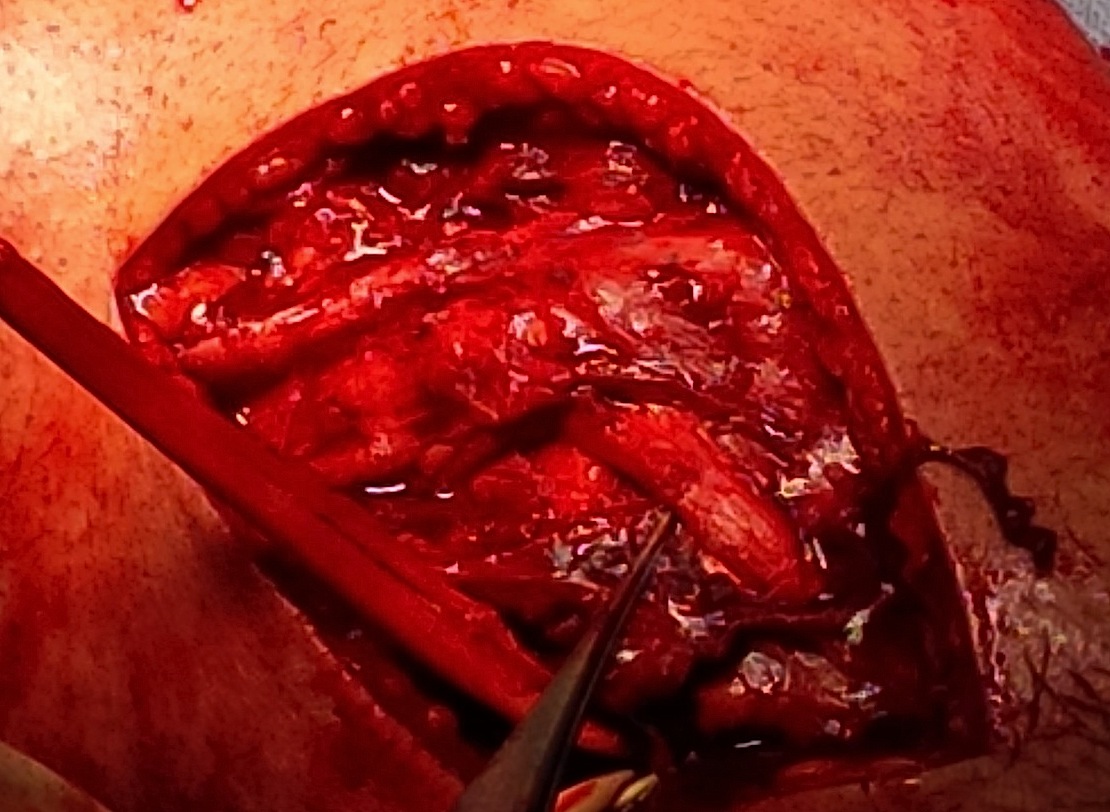
1. Posterior to Biceps femoris
Find and protect CPN
- identify out of zone of injury proximally
- posterior to biceps femoris
- open fascia
- identify nerve in fat
- release
- dissect down to fibular neck
- contained in fibular tunnel (peroneus longus muscle)
- has connective tissue securing to fibular neck which must be released
- release down into anterior compartment
- identify and protect with vessiloop
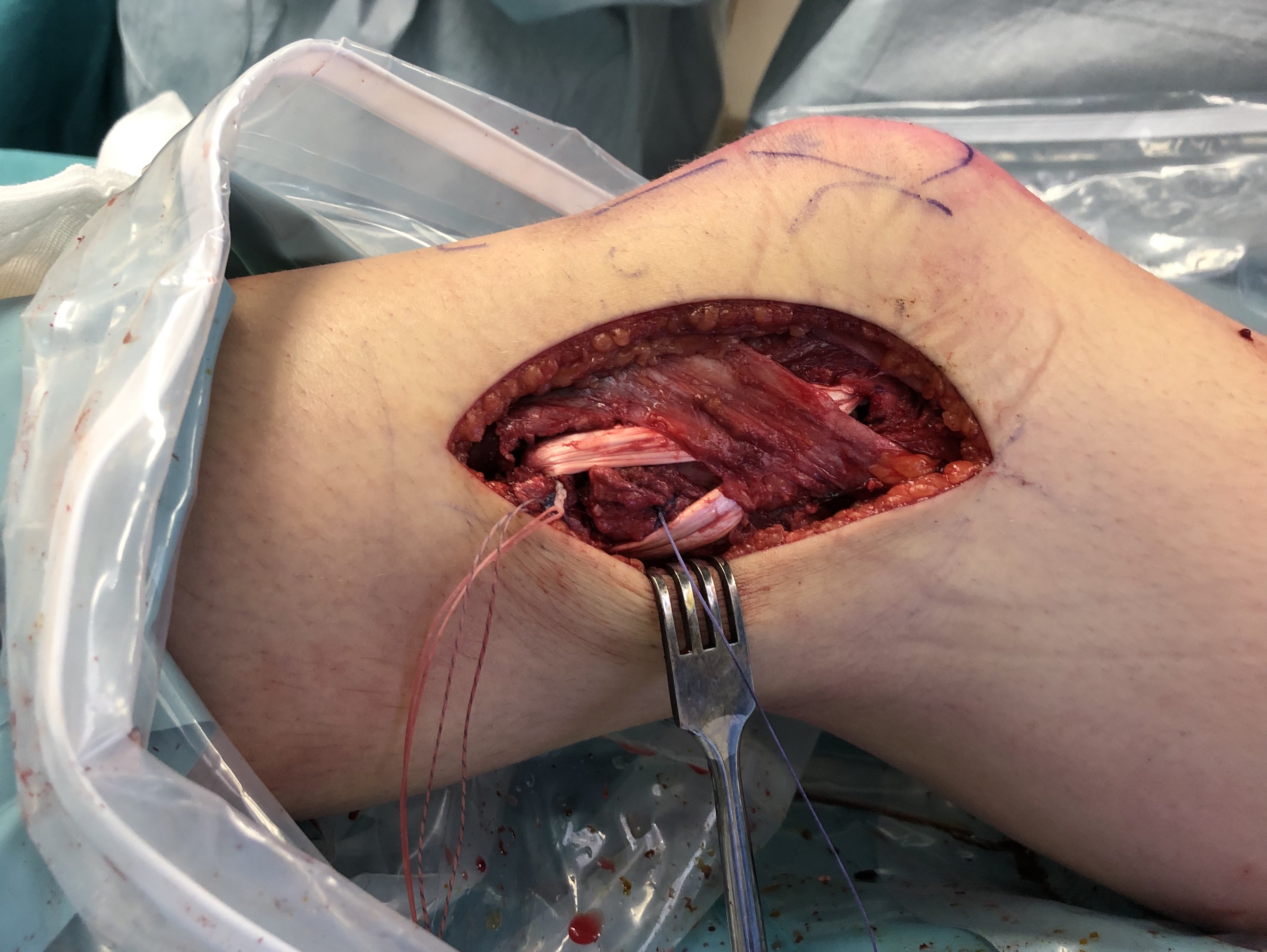
2. Between biceps and ITB
Elevate posterior border of ITB
- identifies the fibular head
- LCL and biceps femoris fibular insertion
- posterolateral window for exposing tibia
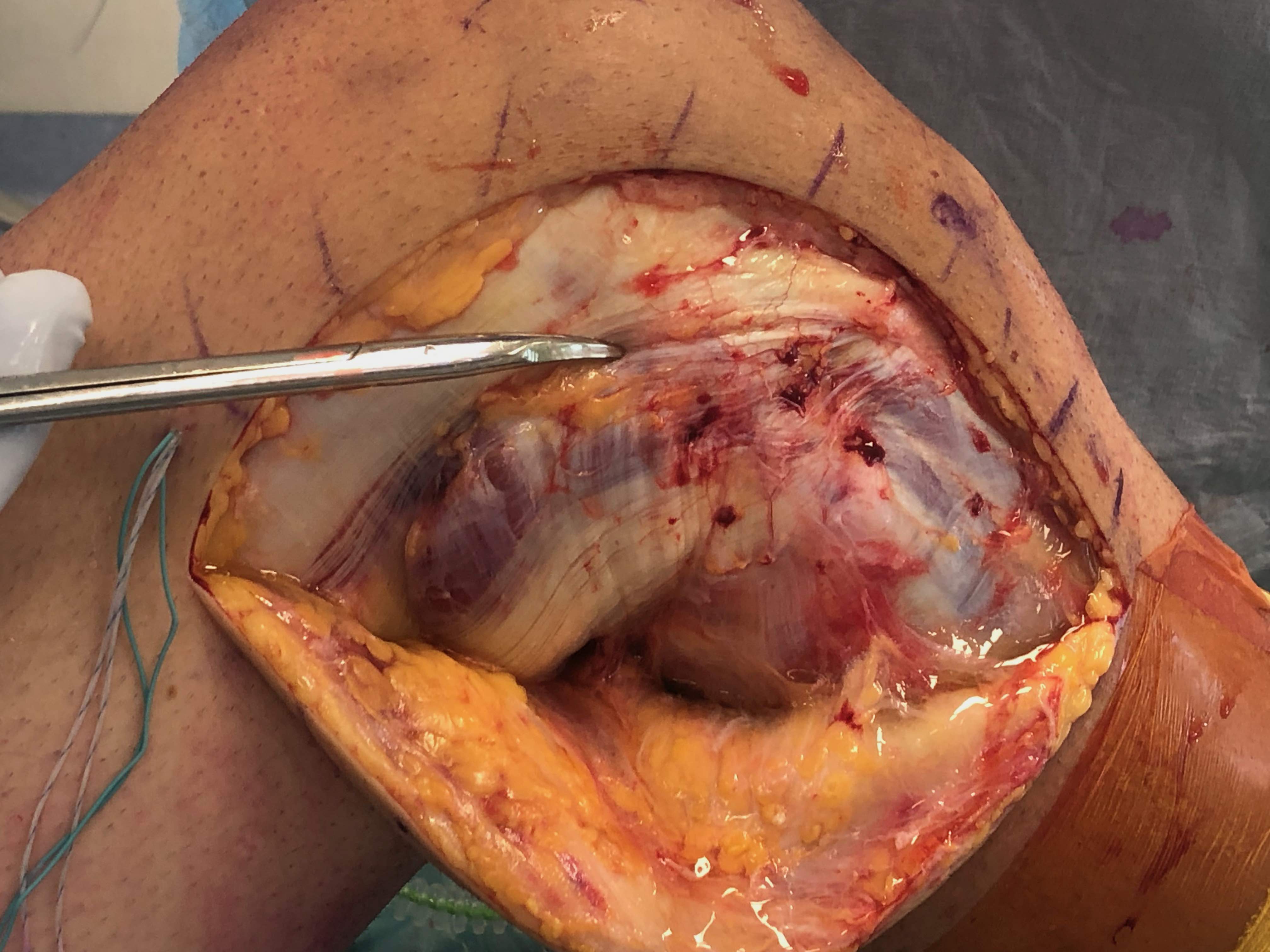
3. Bisect ITB
Midpoint of ITB
- dissect onto epicondyle
- femoral insertion LCL
- femoral insertion popliteus
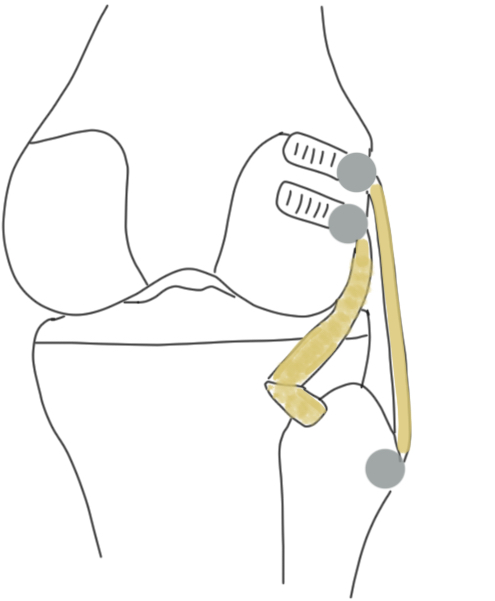
Identify femoral insertion of LCL and popliteus
Can tag LCL on fibular head
- pulling on it will identify femoral insertion
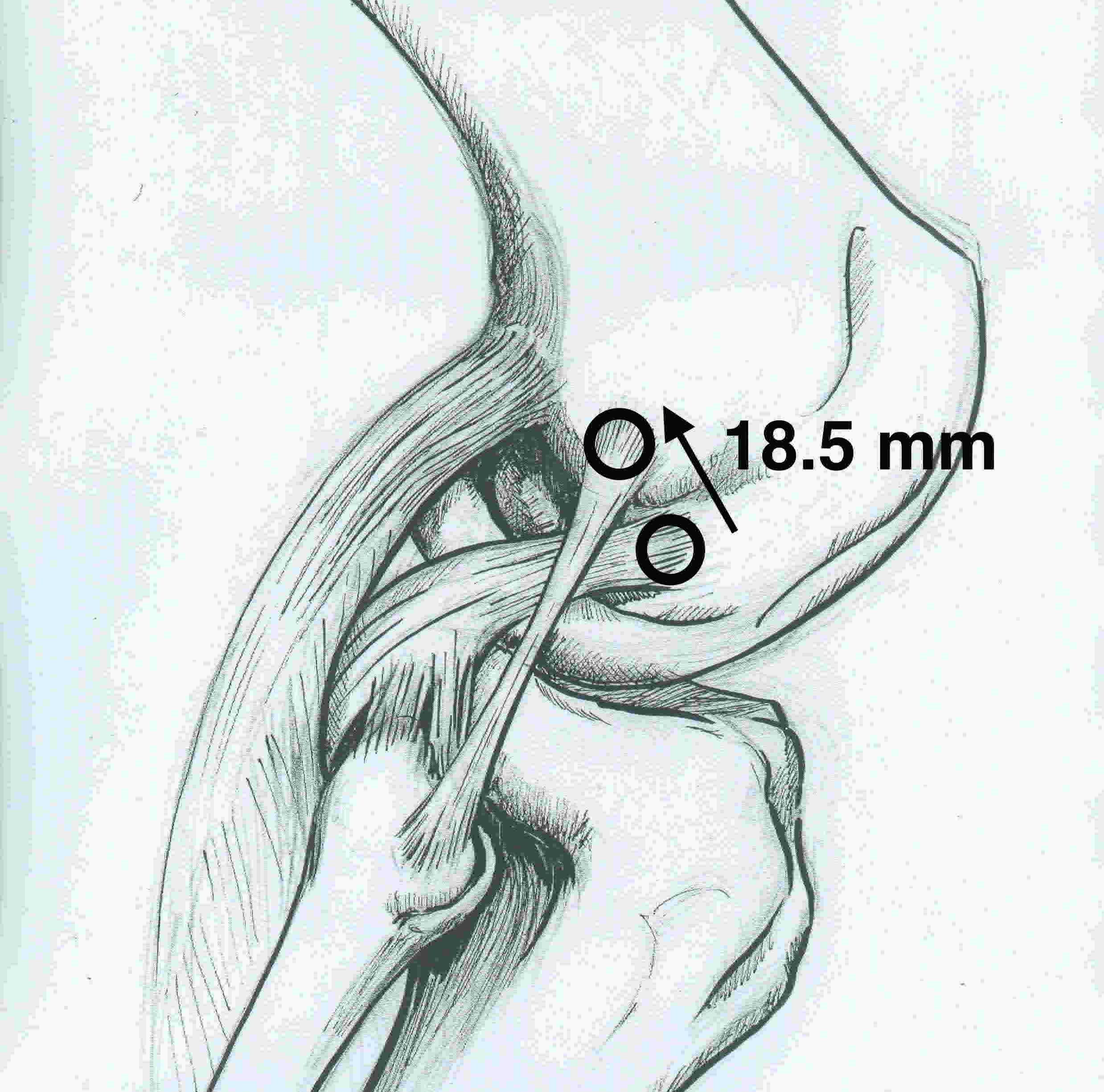
- insertion is 1.4 mm proximal and 3 mm posterior to lateral epicondyle
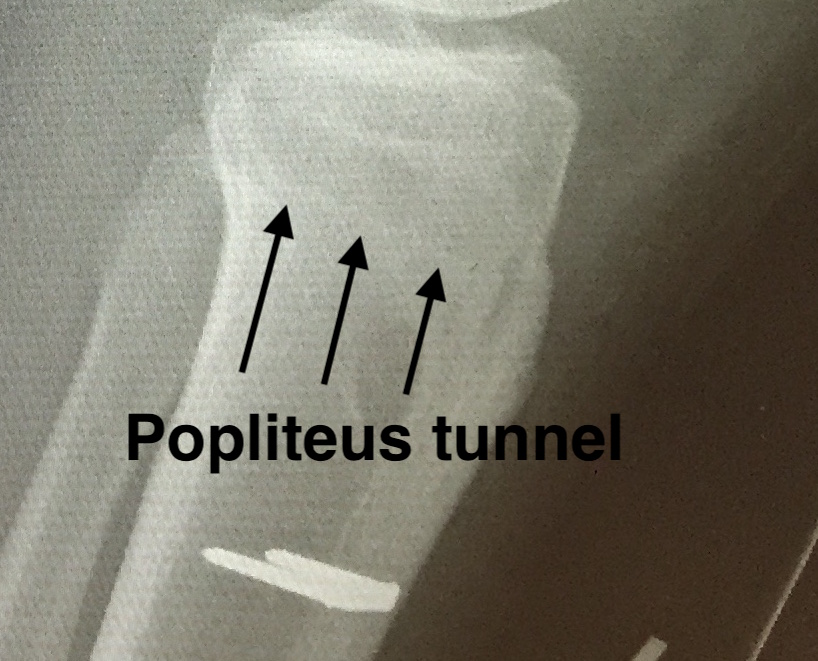
Open popliteal sulcus
- follow popliteal tendon into insertion at anterior 1/5 of sulcus
- this is intra-articular
- distal and anterior to LCL insertion
- 18.5 mm from LCL insertion
Prepare fibula for LCL reconstruction
Window posterior to ITB
- preserve insertion of long head of biceps femoris
- protect CPN
- open long head of biceps bursa to identify LCL insertion
Expose fibular neck
- release anterior compartment muscles and peroneus longus from anterior fibular head and neck
- clear posterior fibular head and neck (popliteus muscle)
Posterolateral corner (LCL + popliteus +/- popliteofibular ligament)
Options
1. LaPrade technique (anatomic popliteus / LCL / popliteofibular)
2. Arciero technique (fibular tunnel, single graft to anatomic insertion of LCL and popliteus)
3. Larson loop (fibula sling through fibula to LCL insertion)
LaPrade posterolateral corner reconstruction
Arceiro Larson loop
Results
Extremely mixed groups of patients, so conclusions difficult to make
Treme et al. Orthop J Sports Med 2019
- biomechanical comparison of LaPrade anatomical reconstruction and Arciero technique
- no significant difference in varus or external rotation stability for either
1a. LaPrade posterolateral corner reconstruction (allograft technique)
LaPrade surgical technique PDF
Concept
Reconstructs LCL / popliteus / popliteofibular ligament
Grafts
Achilles allograft split in two
- 8 x 20 mm bone blocks
- LCL - tendon needs to pass through a 7 mm fibular tunnel
- popliteus - tendon needs to pass through a 9 mm tunnel
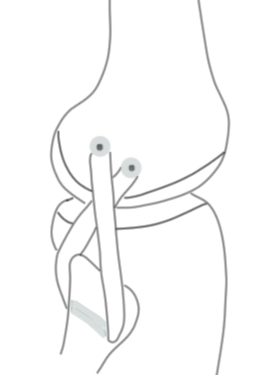
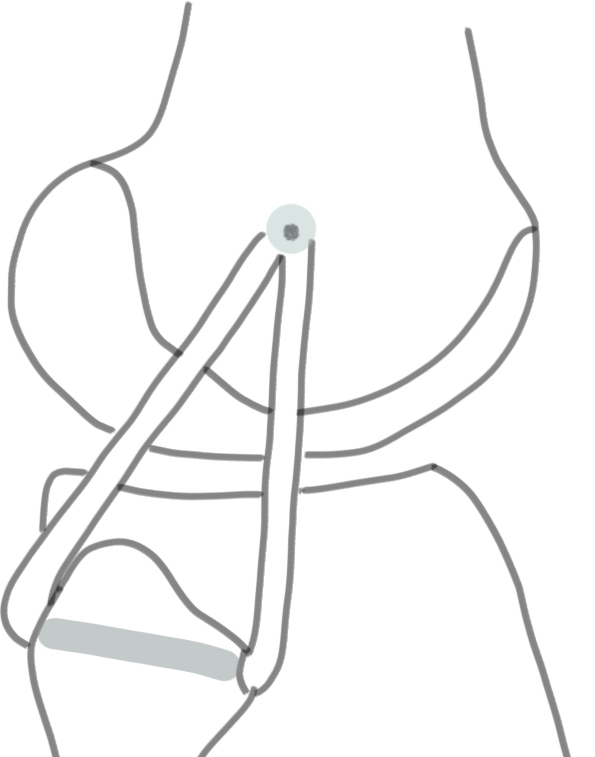
Femoral Tunnels
LCL femoral tunnel
- split ITB to identify the femoral insertion
- develop window posterior to ITB to identify insertion onto fibular head
- can place suture into LCL at fibular head, tugging on it will identify femoral insertion
- insertion is 1.4 mm proximal to epicondyle and 3 mm posterior
- drill 9 x 20 - 25 mm tunnel
- secure 8 x 20 mm bone block with 7 x 20 mm metal screw
Popliteus femoral tunnel
- use split ITB window
- follow popliteus sulcus anteriorly
- femoral tunnel is 18.5 mm anterior and distal from LCL
- drill 9 x 20 - 25 mm tunnel
- secure 8 x 20 mm bone block with 7 x 20 mm metal screw

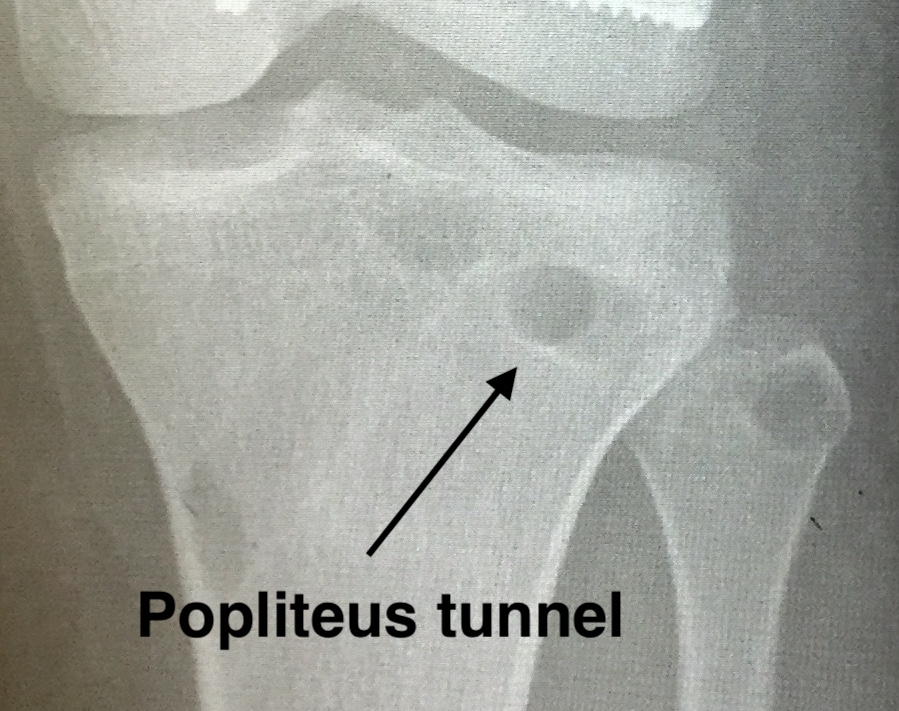
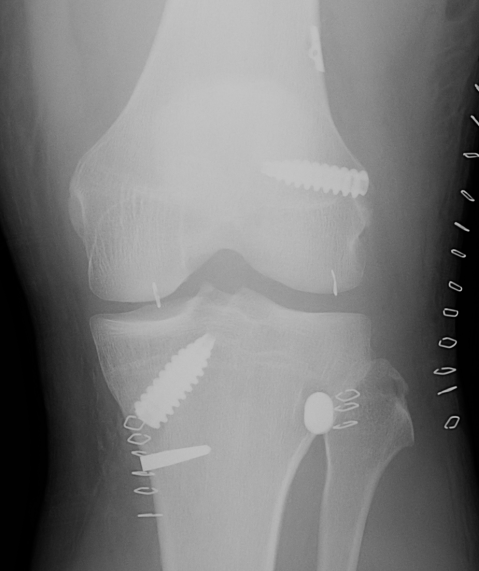
Left knee with LCL and popliteus tunnels and screw fixation of grafts
Tibial / Fibular tunnels
Fibular tunnel for LCL
- insertion of LCL is 8 mm from anterior fibular and 25 mm distal to fibula styloid
- tunnel will pass anterolateral in proximal fibular to posteromedial
- ensure that there is sufficient superior bone in fibular head
- if blow out fibular head will not be able to secure LCL
- place posterior retractor
- drill 7mm tunnel protecting the CPN

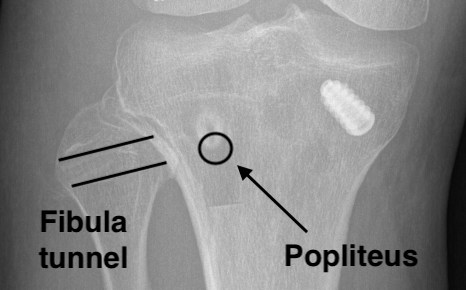
Popliteus tibial tunnel
- anterior entry point is distal and medial to gerdy's tubercle, below tibial plateau
- create posterior window
- anterior to lateral head of gastrocnemius, posterior to knee capsule, above LHB
- insert retractor under lateral head of gastrocnemius to protect vascular structures
- identify and ligate the lateral inferior geniculate artery
- identify with a finger the proximal tibio-fibular joint
- the posterior tunnel must exit medial to this joint, below tibial plateau
- at approximate site of the popliteus musculotendinous junction
- pass beath pin anterior to posterior
- drill to 9 mm
Pass and secure grafts
LCL graft
- pass under IT band
- pass front to back through fibular tunnel
- secure with front to back 7 x 20 mm soft tissue screw
- foot at 30o of flexion, neutral rotation, valgus force
- can pass second limb through popliteus tibial tunnel to reconstruct popliteofibular ligament
- can also secure second limb back onto itself
- or secure second limb onto femur with screw and soft tissue washer
Popliteus graft
- pass under IT band and the LCL
- pass back to front through tibial tunnel
- secure with front to back soft tissue screw 9 x 25 - 30 mm
- foot at 70o of flexion, neutral rotation


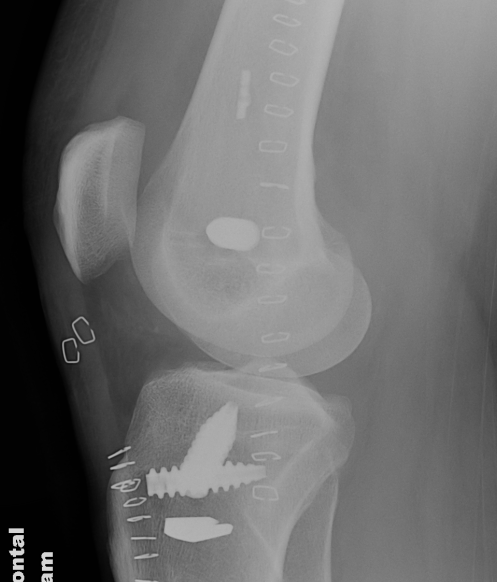
ACL + LaPrade reconstruction of LCL and popliteus
1b. LaPrade posterolateral corner reconstruction (hamstring autograft technique)
LaPrade surgical technique PDF
2. Arciero posterolateral corner reconstruction
Concept
Single graft technique
Femoral tunnels in the anatomic location of LCL and popliteus
Standard trans-fibular tunnel
Reconstructs LCL and popliteus ligament
Technique
Drill blind popliteus tunnel
- secure graft
Drill LCL tunnel is drilled through femoral condyles
- allows tensioning of the graft
Arciero surgical technique PDF
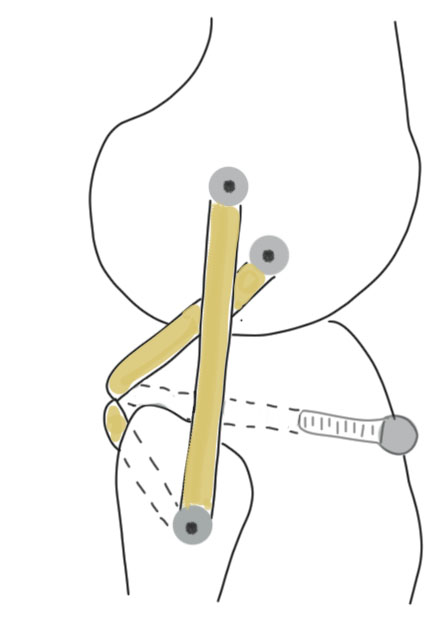
3. Modified Larson loop

Concept
Fibular sling
- single femoral tunnel
- standard transfibular tunnel
- dock both limbs into femoral tunnel
Technique
Single femoral tunnel at eipcondyle
- standard fibula tunnel
- pass graft through fibula
- posterior limb passed deep to ITB and long head of biceps
- anterior limb passed deep to ITB
- secure both limbs in single femoral tunnel
- need to drill femoral tunnel though femoral condyles to allow tensioning

ACL + Posterolateral corner
Issue
Convergence of ACL tunnel and femoral tunnels of popliteus / LCL
Drill anterior to avoid more posterior ACL femoral tunnel
Avoid proximal drilling of LCL tunnel, as will approach ACL femoral tunnel
Moatshe et al. Am J Sports Med 2017
- avoiding tunnel convergence
- aim LCL and popliteus tunnel anteriorly 35o
Gelber et al. Arthroscopy 2013
- CT analysis of PLC tunnels in setting of ACL
- popliteus tunnel: drill at 30o proximal and 30o anterior
- LCL tunnel: drill at 30o anterior, but 0o proximal
Graft tensioning sequence
Evidence unclear
1. ACL
2. LCL
3. Popliteus