Anatomy
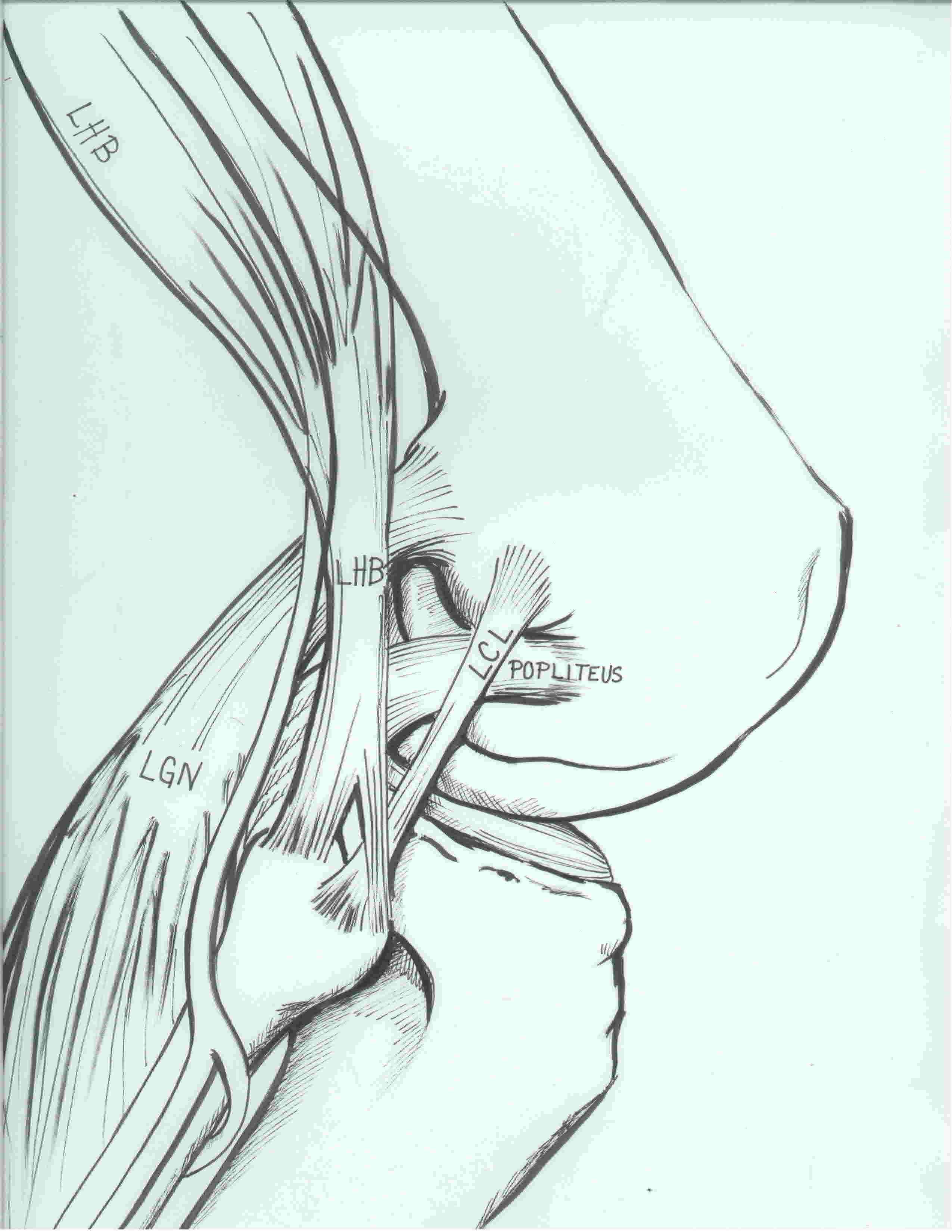
3 primary stabilizers (plus posterolateral capsule)
LCL / Popliteus / Popliteofibular ligament
1. Lateral collateral ligament
Femoral attachment
- small bony depression just behind lateral epicondyle
- 1.4 mm proximal and 3 mm posterior to lateral epicondyle
Fibular attachment
- 25 mm distal to fibula styloid
- 8 mm posterior to anterior fibular head
- attaches to anterolateral fibular head
Action
- primary varus stabilizer of the knee
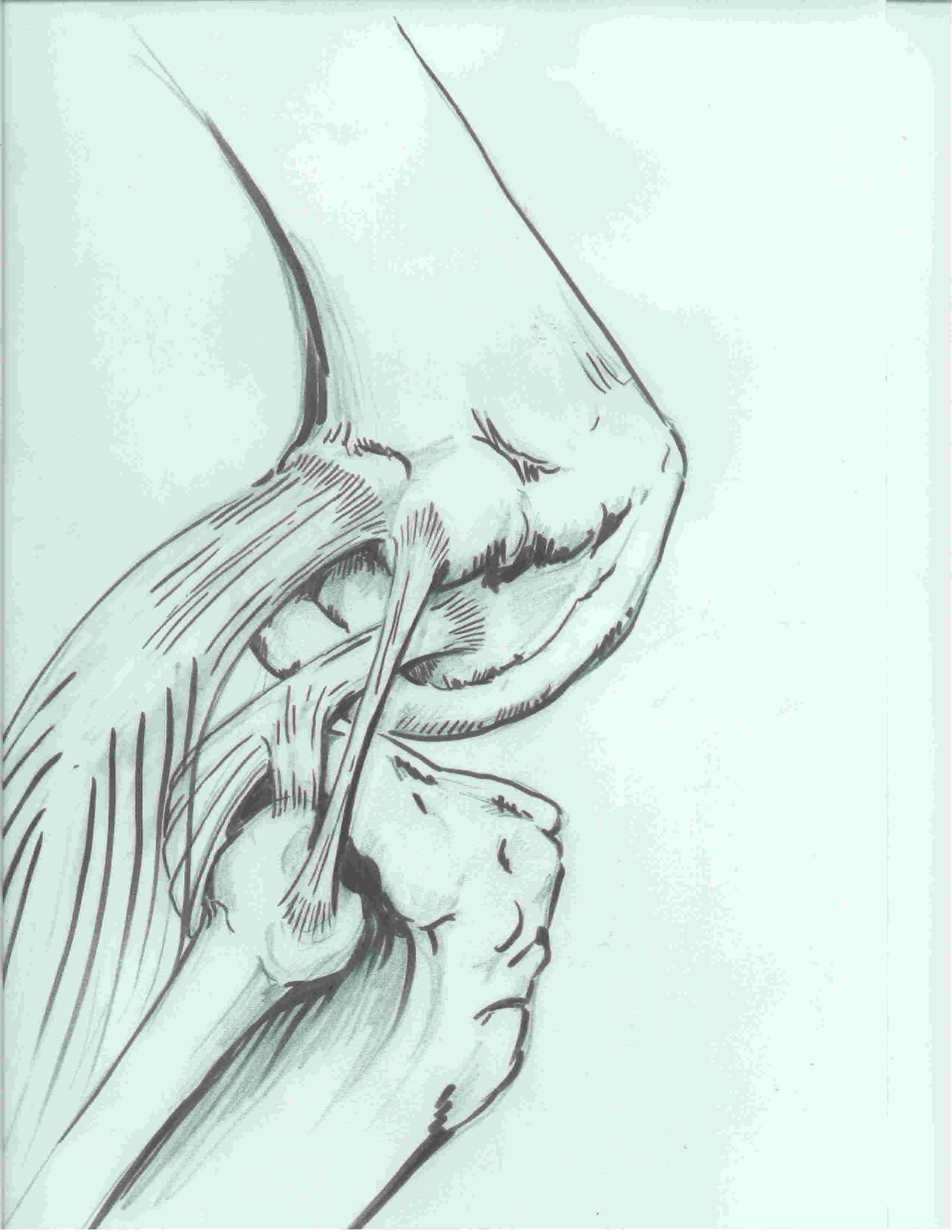
2. Popliteus tendon
Origin
- posteromedial tibial
- becomes tendon at lateral one third of the popliteal fossa
Insertion
- tendon passes through capsule and hiatus in coronary ligament of lateral meniscus
- runs around lateral femoral condyle
- passes deep to LCL
- inserts into most anterior aspect of the popliteus sulcus
- always anterior and distal to LCL
- average 18.5 mm between LCL and popliteus femoral insertion
Action
- laterally rotates the femur (important when unlocking the knee from full extension)
- also retracts the lateral meniscus in flexion to prevent entrapment of lateral meniscus
- resists external rotation of the tibia
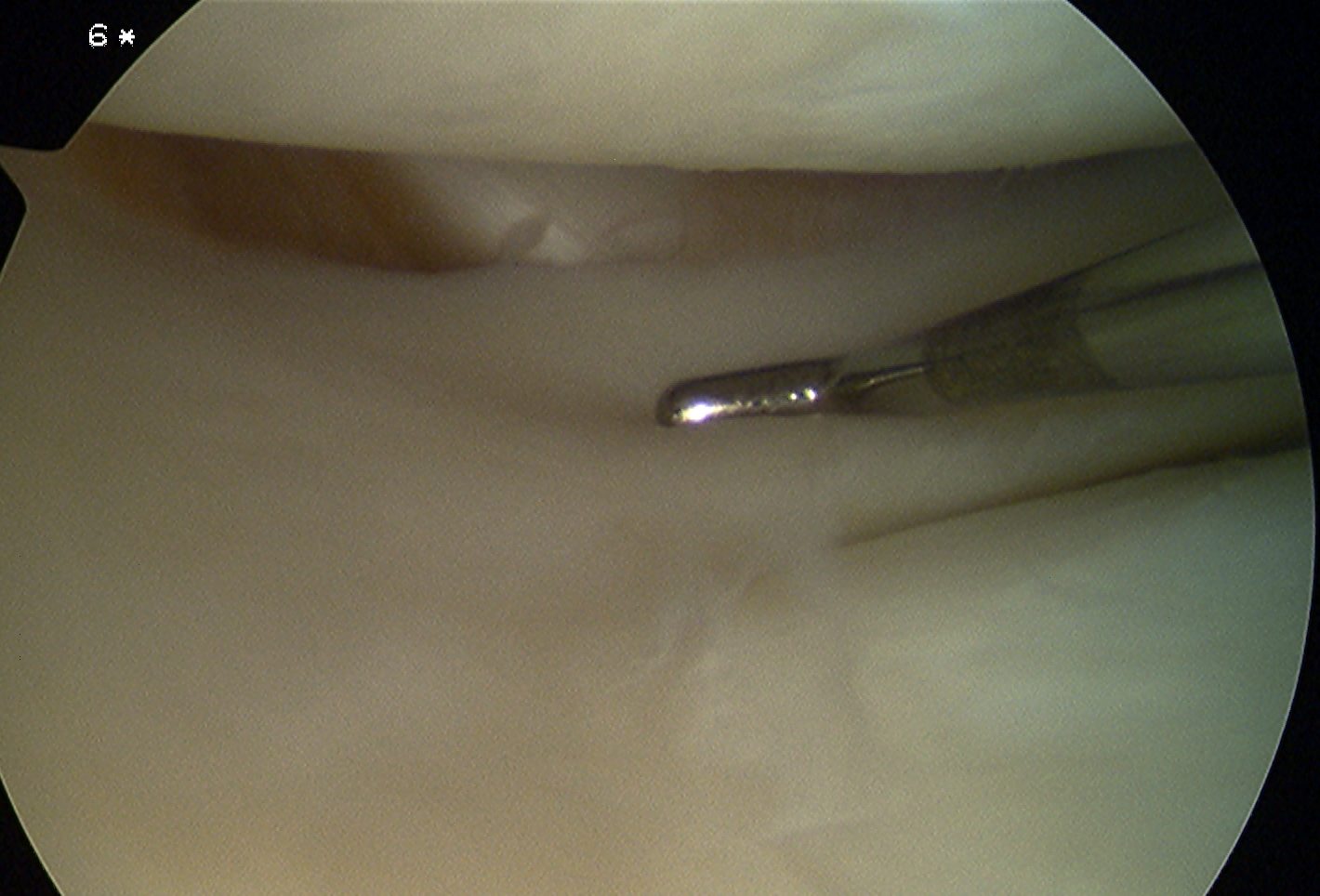
Arthroscopy of right knee showing intra-articular popliteus tendon behind lateral meniscus
3. Popliteofibular ligament

Origin
- musculotendinous junction of the popliteus tendon
Insertion
- fibular styloid
Action
- acts as check rein to popliteus
- resists external rotation
Seebacher lateral layers of the knee
1. Superficial
ITB, biceps femoris tendon, CPN
2. Middle
Patella retinaculum
3. Deep
Posterolateral capsule
LCL / Popliteus / Popliteofibular ligament
Other anatomy
Common Peroneal Nerve
Origin in bifurcation of sciatic nerve in popliteal fossa
- runs along posterior border of biceps femoris
- around neck of fibula in the fibula tunnel covered by peroneus longus
- attached to bone here by connective tissue
- then branches into deep peroneal and superficial peroneal nerve
- also gives branches to the knee joint
Lateral inferior geniculate artery
Orginates from the popliteal artery
- runs anterior to lateral head of gastrocnemius
- along superior border of popliteus muscle
- above fibular head and under LCL
- provides a branch that runs around fibula neck
- need to identify and ligate
Incidence
LaPrade et al. Arthroscopy 2007
Isolated PLC injuries rare but occur
Isolated LCL injuries rare but occur
Majority of PLC injuries occur in setting of other ligament injuries (ACL / PCL / multiligament knee injury)
Mechanism
Twisting injury
Direct blow to anteromedial side of knee
Hyperextension injury
Associated Injuries
PCL
ACL
CPN (15%)
History
Significant injury
Swelling may be delayed in setting of isolated injury
Instability with extension
- knee may buckle into hyperextension with weight bearing
- may walk with knee in flexion to maintain stability
Examination
Gait / Stance
Varus thrust in gait and single leg stance
- due to ER of tibia
- apparent varus
- flexed attitude to knee
LCL
Varus force at 30° flexion and in full extension


Examination of right knee demonstrating grade 2 instability of LCL
Grade 1
- < 5mm laxity in 30o flexion
- partial tear
Grade 2
- 5 - 10 mm laxity in flexion
- isolated injury to LCL
Grade 3
- > 10 mm laxity in flexion
- laxity in full extension
- indicates complete disruption of LCL plus a secondary restraint (ACL and or PCL)


EUA of right knee demonstrating grade 3 laxity of LCL in full extension
Posterolateral Corner instability
Dial Test
- patient prone
- increased external rotation of tibia >10 - 15° compared to other side
- increased external rotation at 30o of knee flexion only - posterolateral corner
- increased external rotation at both 30o and 90o - PCL + posterolateral corner

Prone dial test, with increased external rotation of left knee at 30 degrees - isolated posterolateral corner


Intraoperative dial test with patient supine. Increased external rotation of the right foot at 30 degrees - isolated posterolateral corner
External rotation recurvatum test
- patient supine
- pick up both legs leg via great toe
- tibia hyperextends and externally rotates with injury to posterolateral corner

External rotation of the right knee
Posterolateral draw
- knee at 90o flexion with the foot externally rotated
- apply a posterolateral rotatory force
- excessive posterolateral tibial subluxation
Reverse Pivot Shift
- valgus force, foot externally rotated
- flexion to extension
- reduction of posteriorly subluxed lateral tibial condyle
- NB: 35% of uninjured patients positive / check normal knee
PCL
Laxity demonstrated by positive Lachmann
- posterior sag / loss of step off
- posterior drawer
- quadriceps active
- grade III posterior drawer associated with injury to the posterolateral corner as well as PCL

Posterior sag of the knee as a result of PCL injury
ACL
X-ray
Often normal
Bony avulsion of Fibula Head
Avulsion of LCL and long head of biceps



Bony avulsion of Gerdy's tubercle
Avulsion of ITB
Lateral joint widening and subluxation

Right knee in POP with opening of lateral compartment
PCL bony avulsion
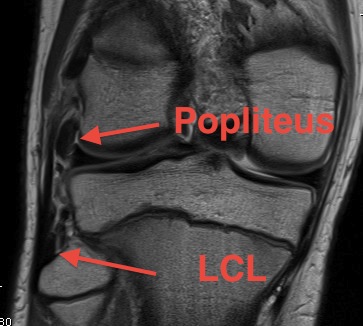
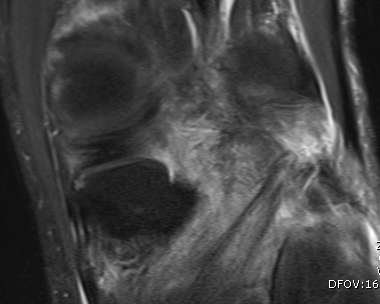
MRI
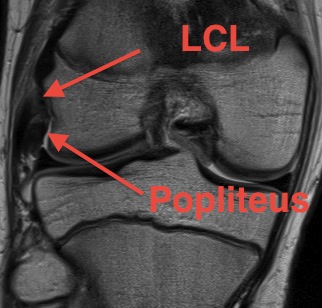
Lateral collateral ligament anatomy
Don't see entire length on single MRI
- use coronal to look for origin from lateral epicondyle above popliteal insertion
- use coronal to look for insertion onto anterolateral fibular head



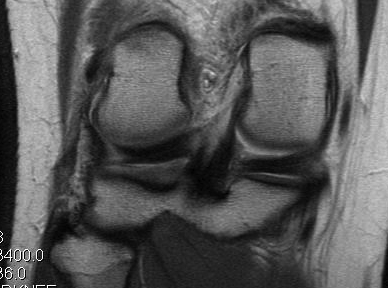
Normal anatomy
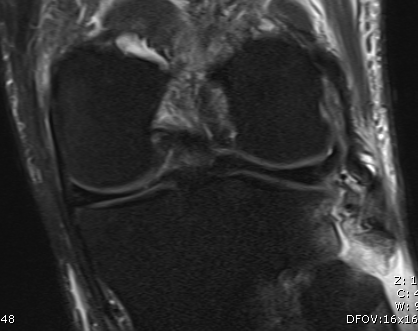
Midsubstance tear of LCL
Popliteus anatomy
Don't see entire length on single images
- coronal image to see insertion onto popliteal fossa below LCL
- follow tendon around on coronal images
- watch as becomes musculo-tendinous (can often be torn here)
- muscle inserts onto posteromedial tibia
Normal anatomy
Popliteofibular ligament anatomy

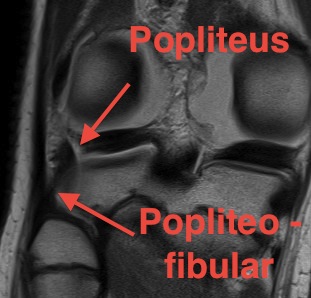
Normal anatomy
Injury

Femoral avulsion of popliteus and LCL

Femoral avulsion of popliteus
Avulsion of LCL and biceps femoris from fibula head
Musculotendinous injury to popliteus