Issues
1. Painful Bunion / Hallux valgus

2. Metatarsalgia / MTPJ dislocation

3. Claw toes

Pathology
Earliest manifestation is synovitis of MTPJ
- capsular destruction
Dorsal subluxation MTPJ
- claw toes develop (MTPJ hyperextended, PIPJ flexed)
Plantar fat pad displaced distally
- MT heads exposed to plantar skin
- corns develop over PIPJ & under MT heads
Management
Non-operative Management
Shoe-wear modification
Extra-depth shoe / low heel / roomy toe-box
Custom-made arch support
Pre-MT dome for metatarsalgia
Heel cup to prevent heel valgus
STJ - single lateral upright with medial T strap
AKJ - double upright with square ferrule
Operative Management
Indications
Continuing pain
Increasing deformity
Footwear modification failure
Issues
Poor wound healing
Infection
Non-union
Recurrence of deformity
Timing in multiple joint surgery
Forefoot often first
- eliminates pedal sepsis
Hallux Valgus / Rigidus
Options
- arthrodesis
- arthroplasty
- Keller's procedure
Arthrodesis
Procedure of choice
- provides forefoot power & buttresses lesser toes
Contra-indication
- involvement of IPJ
- need to have mobile IPJ to put tip of toe onto the ground
- consider arthroplasty
Complication
- non-union
- malposition
- stress transfer to IPJ
Silicone Arthroplasty / Double-Stemmed Swanson
Indication
- low-demand patient
- IPJ of hallux affected
Complication
- breakage
- silicone synovitis
Keller's Procedure
Indication
- in low demand patient where bony union expected to be difficult
- salvage procedure
Complication
- cock up deformity
- transfer metatarsalgia
- loss of power
- recurrence
Metarsalgia
Options
- synovectomy
- Weil's osteotomy
- Fowler's procedure
Synovectomy
Indication
- early disease / synovitis
Technique
- 3 incision
- one over first MT
- 2 between 2/3 and 4/5
- incise extensor hood
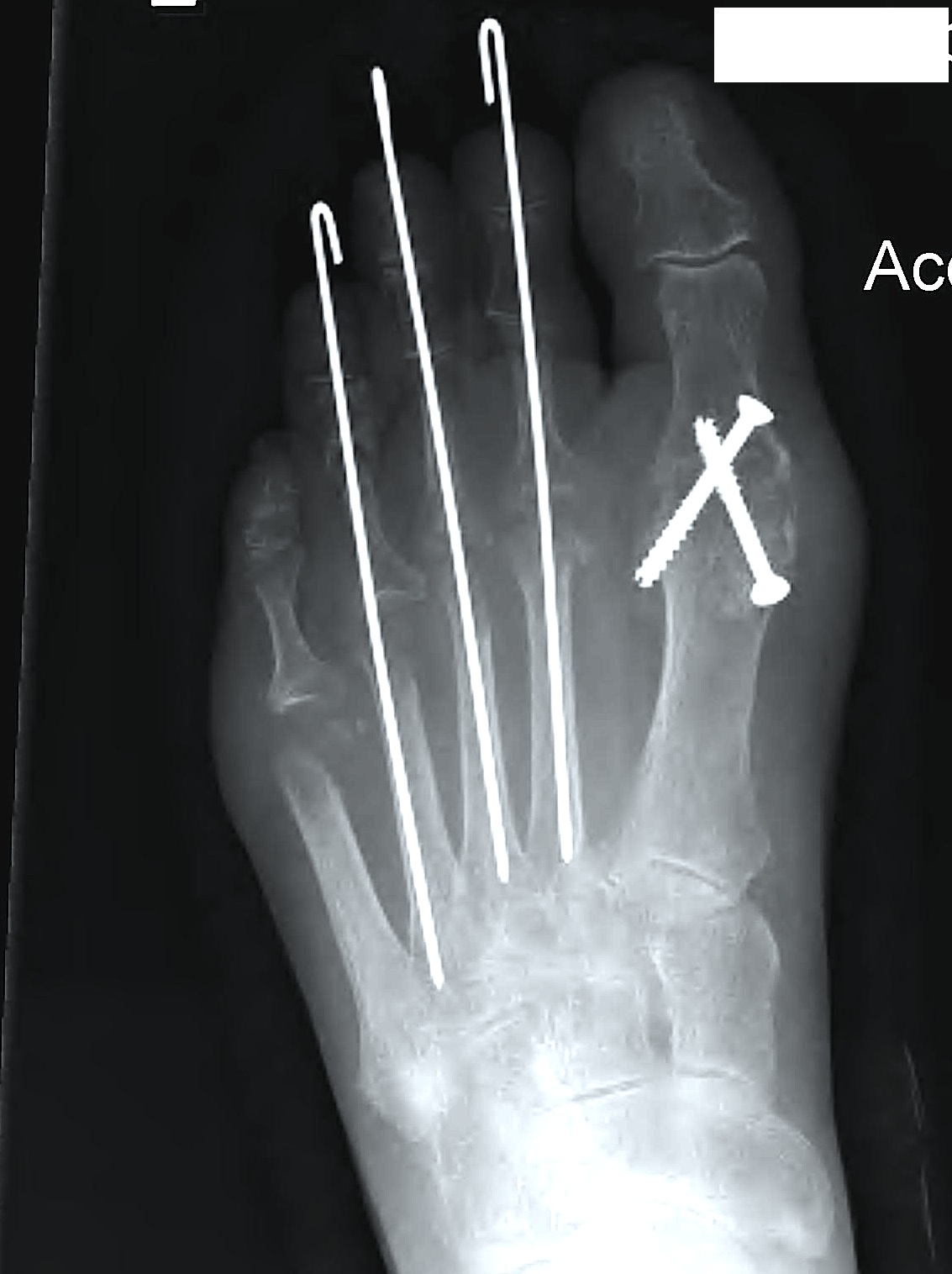
Weil's Osteotomy
Indications
- enlocated MTPJ
- i.e. in conjuction with treatment of claw toe
Technique
- transverse osteotomy
- MT head moved proximally
- secured with screw
Fowler's operation

Indication
- dislocation MTPJ
Concept
- cascading excision of II - V MT heads
- 2nd 3 mm longer than 1st or 3rd
- 3rd 3mm longer than 4th
- 4th 3 mm longer than 5th
Technique
Single dorsal transverse skin excision just proximal to toe webs
- can be performed via transverse plantar ellipse
- with severe dislocation may be easier to approach through plantar aspect
- MT heads subcutaneous & NV bundle usually subluxed dorsally
Extensor tenotomy
MT heads excised in gentle curve
- dorsal distal to plantar proximal
- contoured on plantar surface to give rounded surface
- very little length removed from 5th MT
- must not leave bony fragments in weight bearing pad
Second incision on plantar surface
- proximal to MT heads
- ellipse of skin only excised
- closed to pull skin of forefoot under MT ends
Claw toes
EPL lengthening / EDB tenotomy / PIPJ fusion