
Function
LHB primary function is humeral head depressor
Also accelerate / decelerate arm in overhead sports
Anatomy
Average 9 cm long
- intra-articular and extra-synovial
- thickest at its insertion, progressively narrows
- origin - supraglenoid tubercle and superior glenoid labrum
- takes a 30 degree turn
- biceps pulley - superior glenohumeral ligament, coracohumeral ligament, lateral subscapularis insertion
- enters bicipital groove - between greater and lesser tuberosity
Pain generator
- synovial lining becomes inflammed
- sympathetic innervation on proximal aspect
Problems
| Tendinosis / Tendinopathy | Subluxation / Dislocation | SLAP tears |
|---|---|---|
|
Inflammation Thickening Tearing |
Usually seen with subscapularis tear | www.boneschool.com/SLAP-tears |
| Can completely rupture | ||
 |
 |
 |
Examination
| Speed's test | Yergason's test | O'Brien's test |
|---|---|---|
|
Resisted forward flexion at 90° Forearm supinated Pan in bicipital groove |
Externally rotate arm with elbow 90° Resisted supination - assess pain or popping at bicipital groove |
Shoulder flexed 90o in plane of scapula Adducted 30-45o Max internal rotation / thumb down Resist downward force causes pain No pain with external rotation / thumb up |
 |
 |
 |
Rupture - Popeye appearance

MRI
Tendonitis / tendinopathy
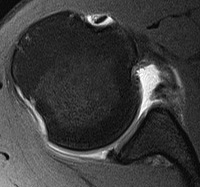
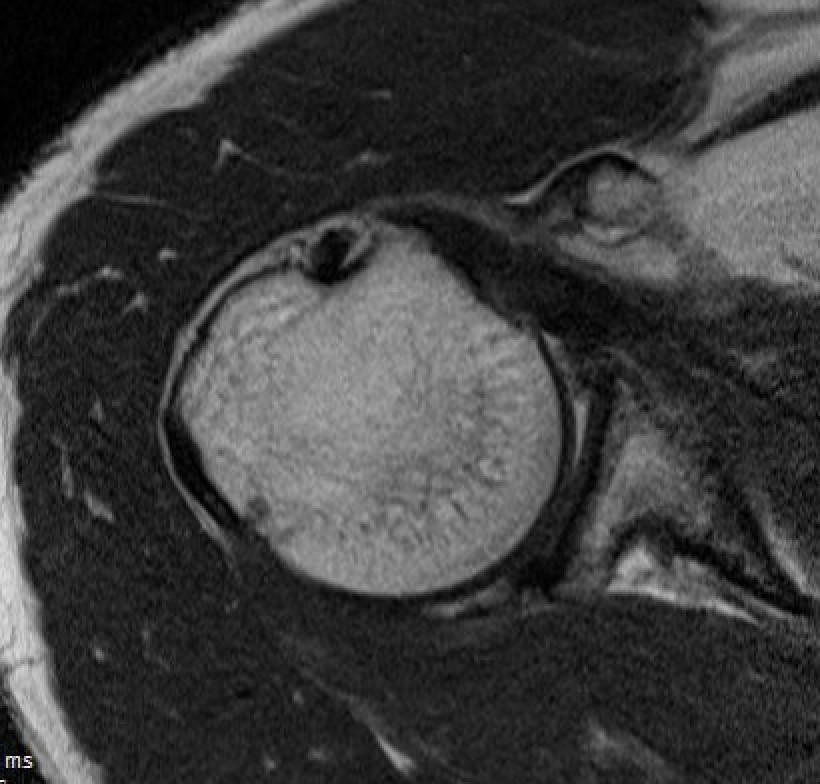
Normal
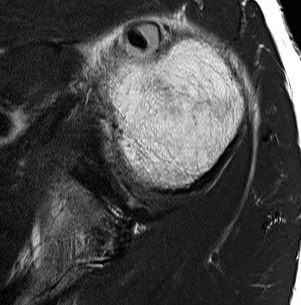
Tendonitis
Tendon thickening / tendinopathy
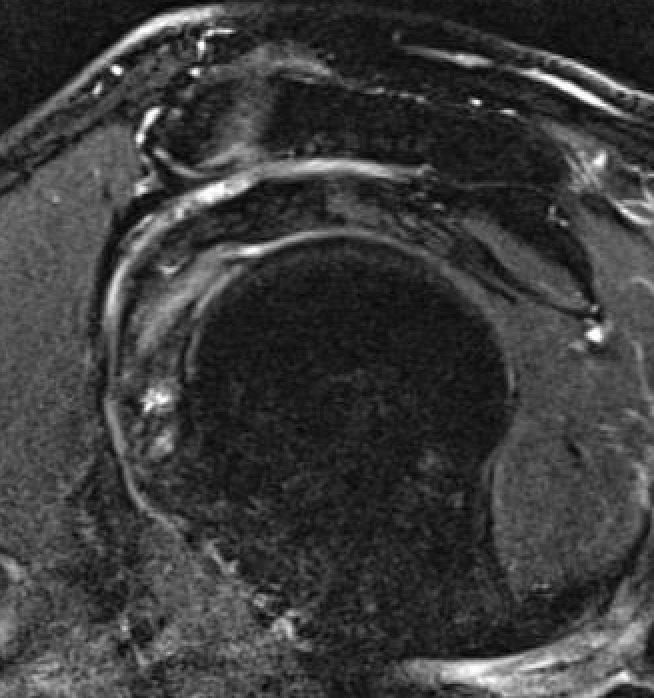
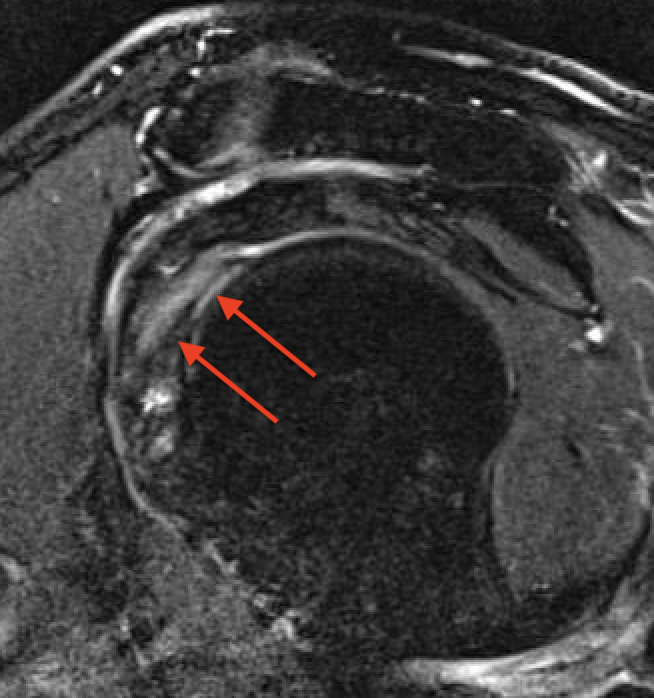
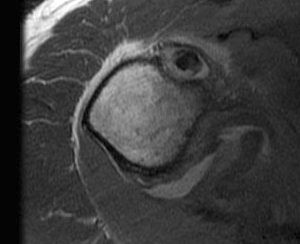
Sagittal MRI demonstrating severe LHB tendinopathy
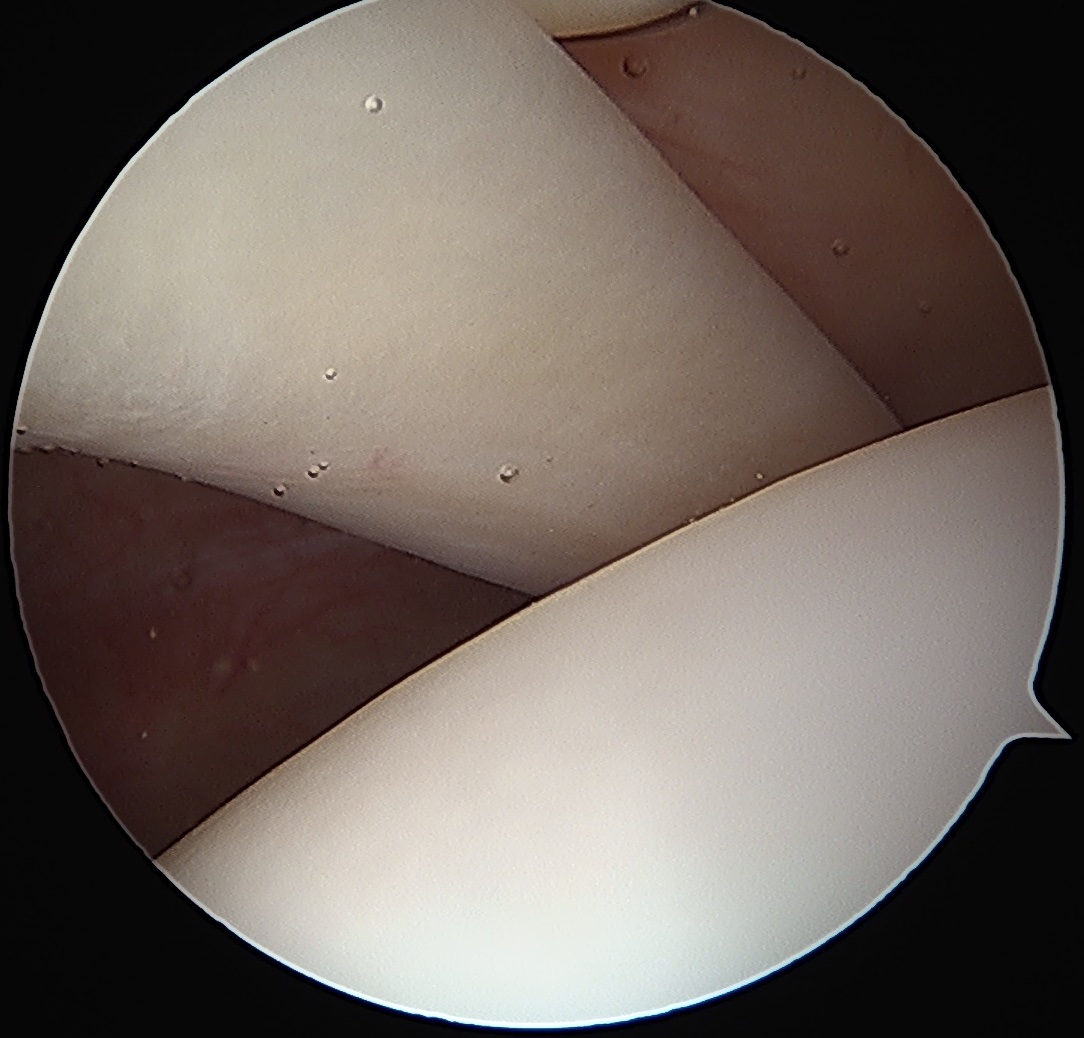
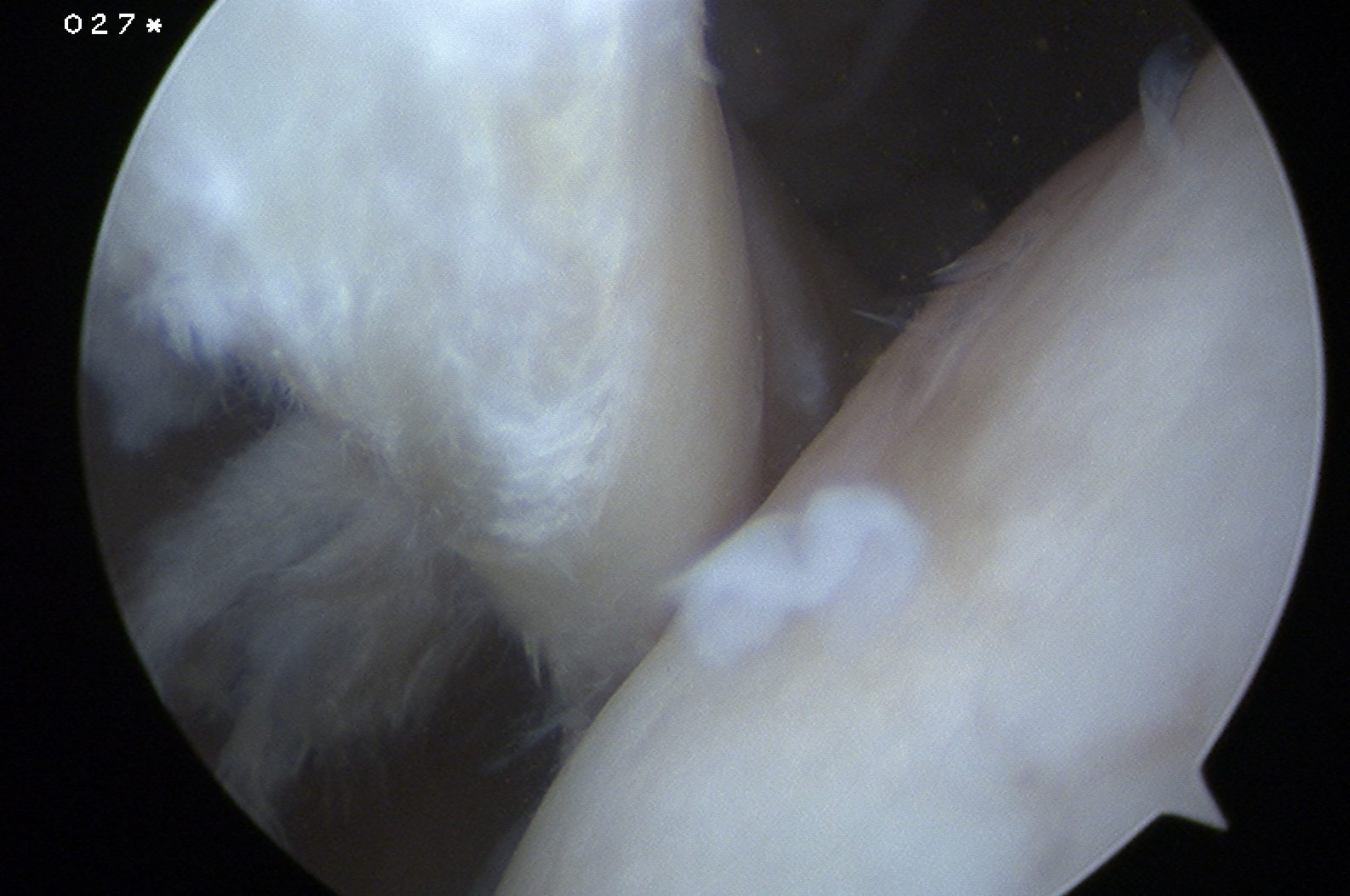
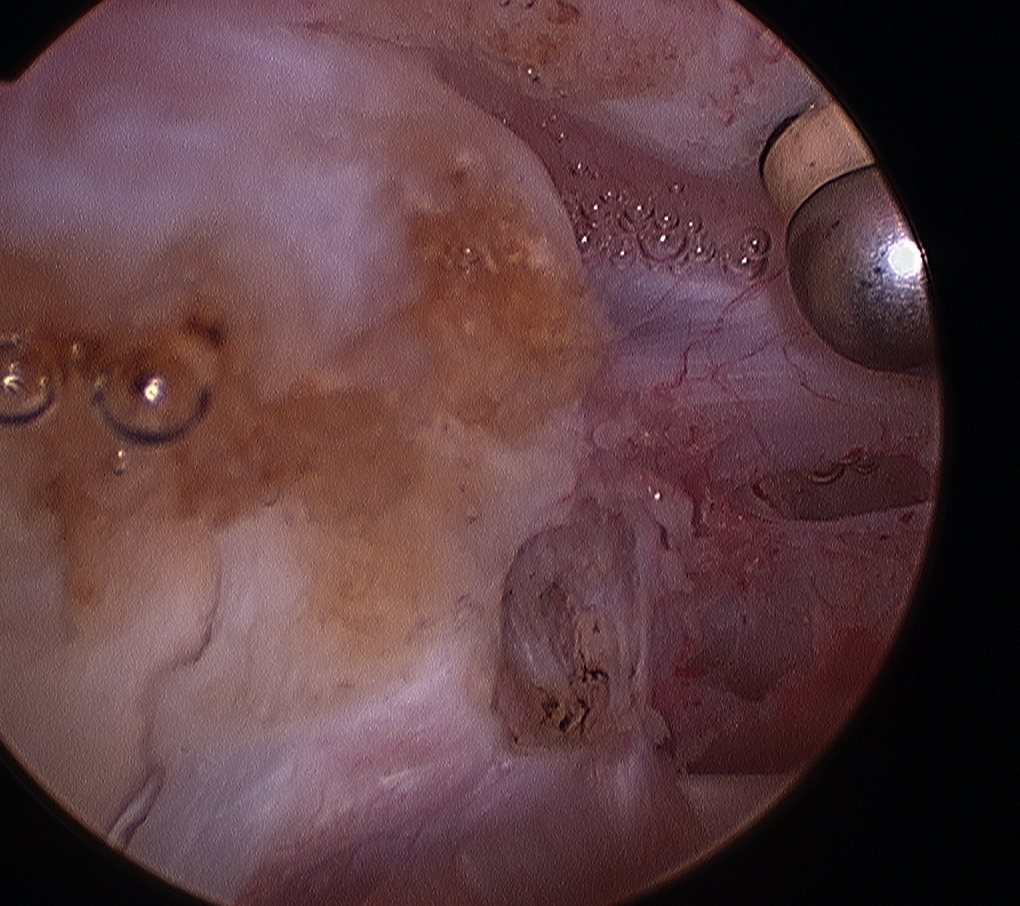
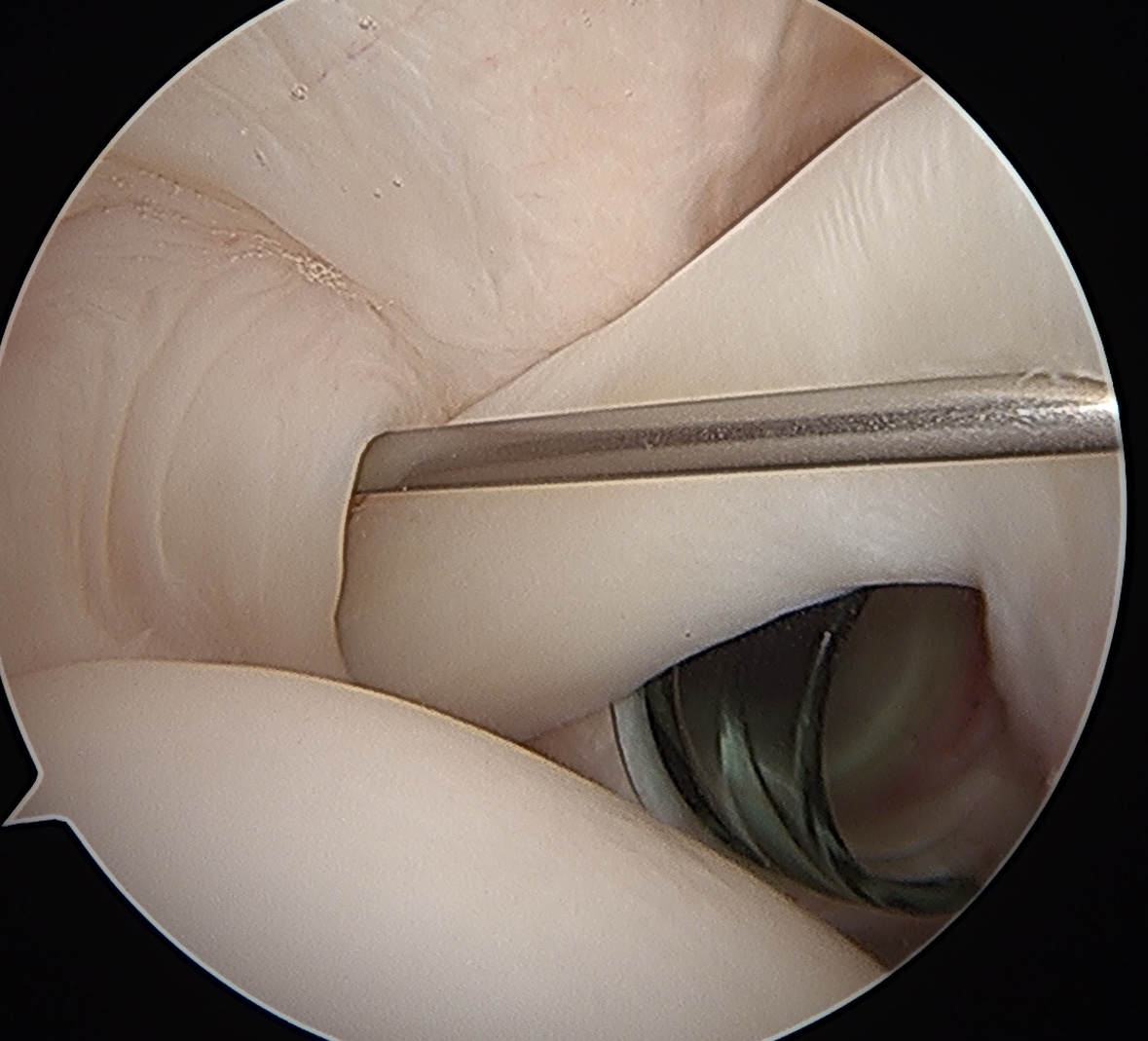
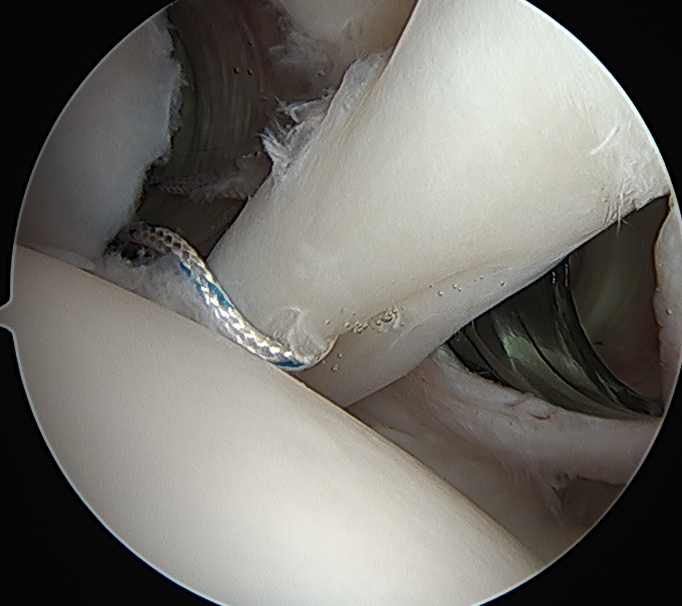
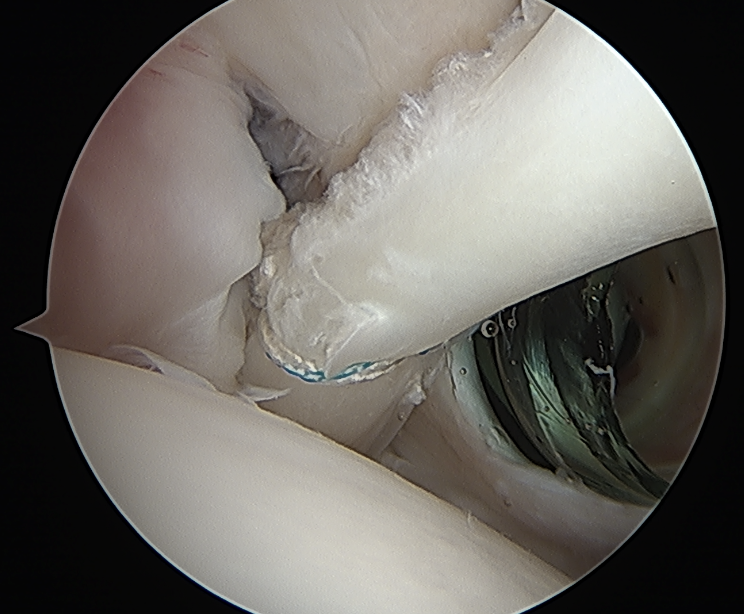
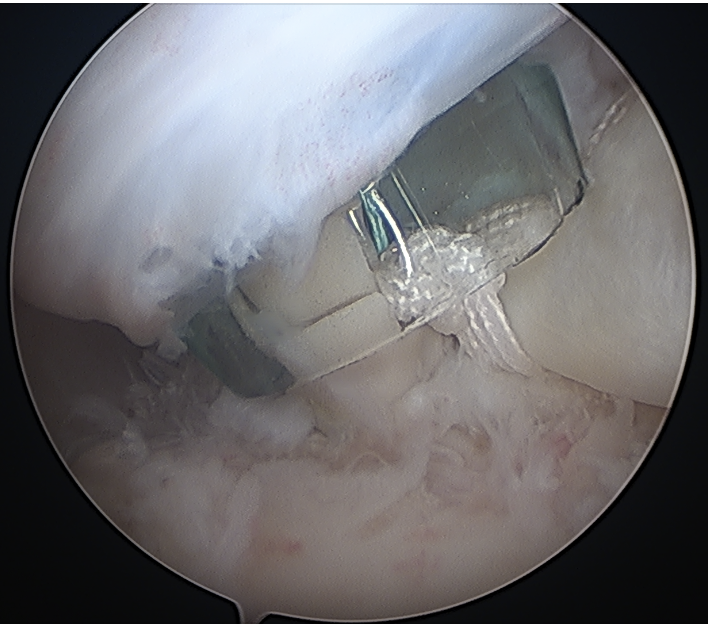
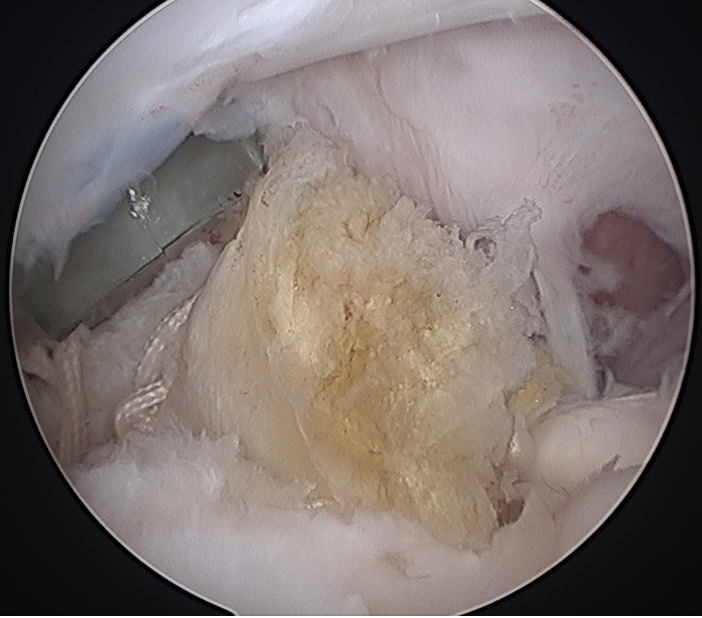
Arthroscopy
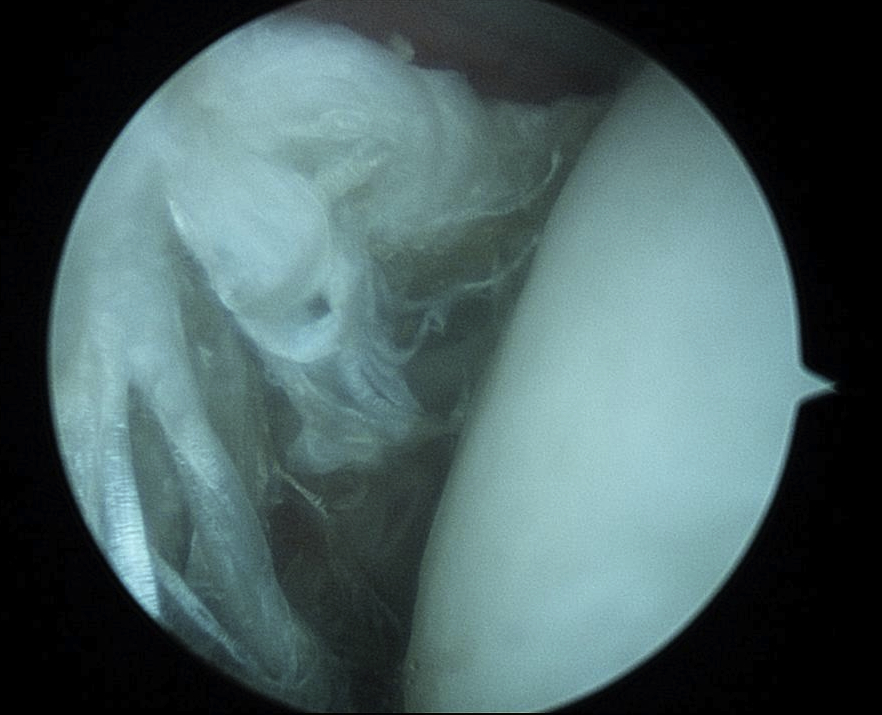
Normal
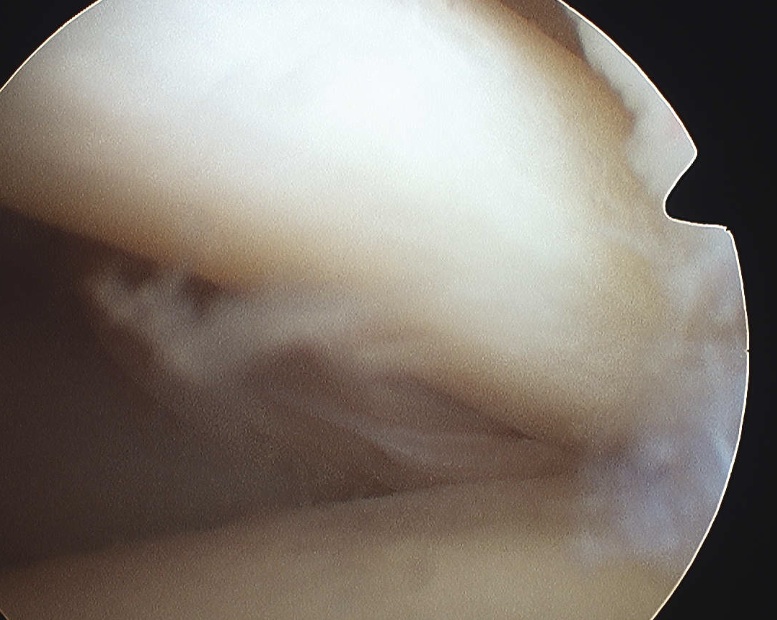

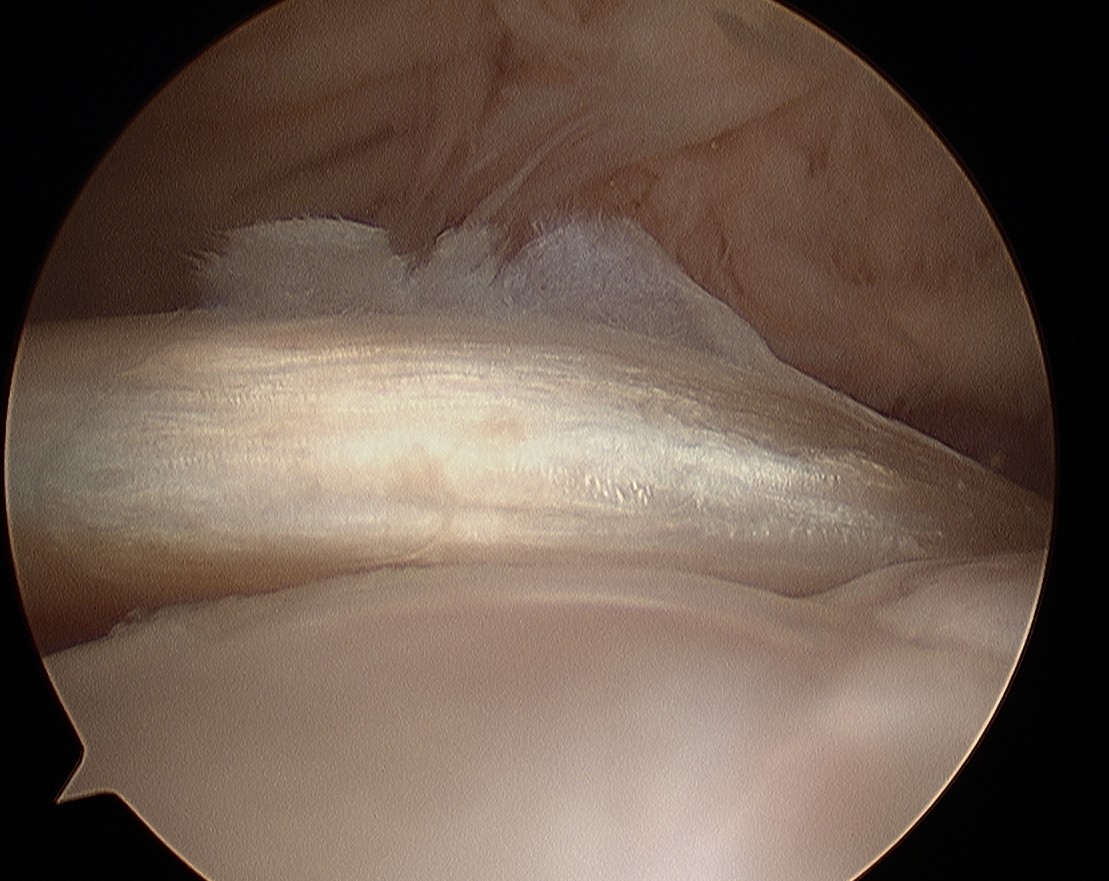
Tendonopathy
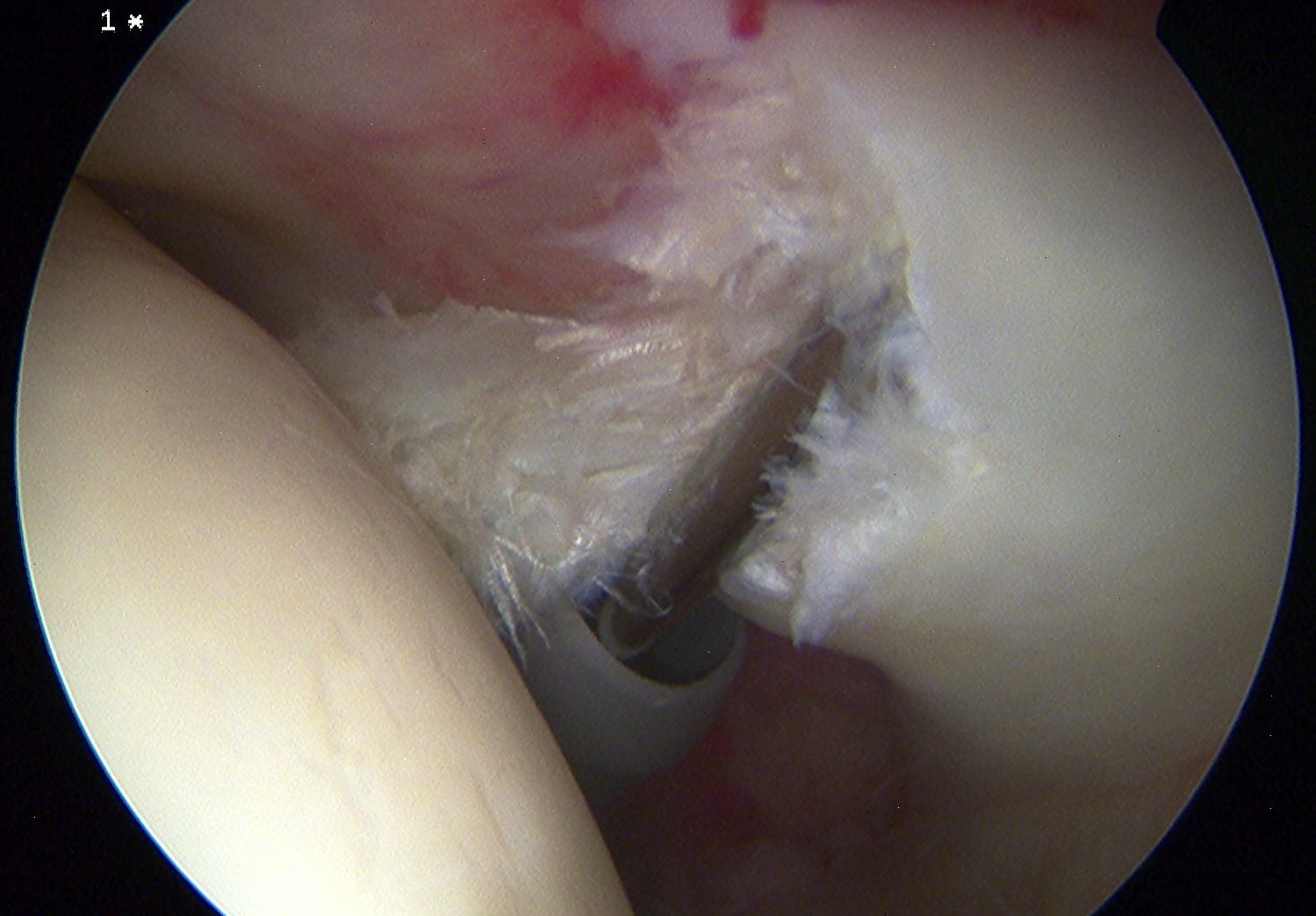
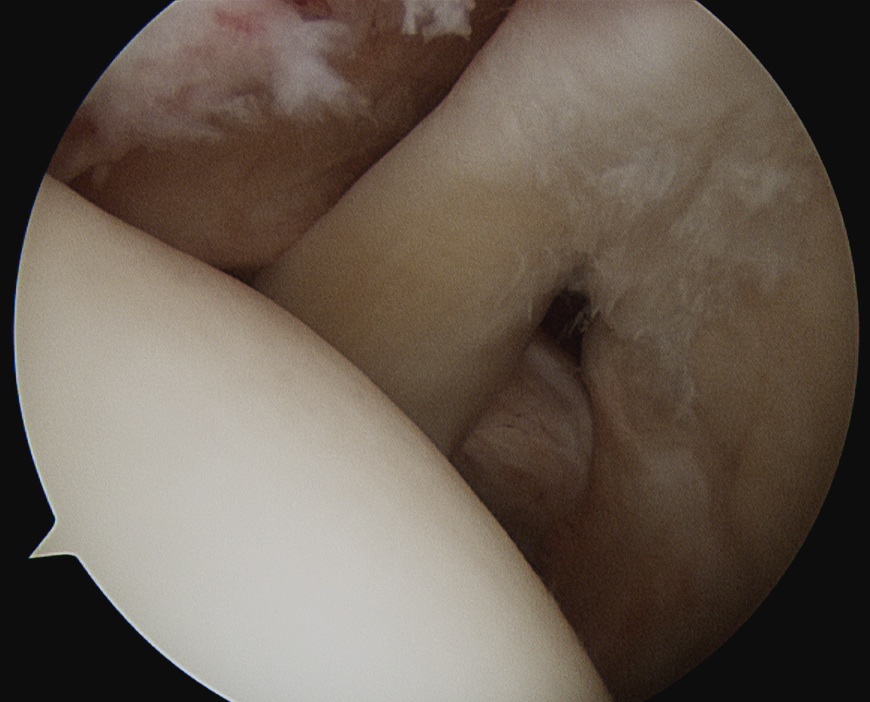
Medial subluxation of LHB
Management
Nonoperative
Physiotherapy
Cortisone injections
Operative management tendinopathy
Options
Tearing < 50%: Debridement
Tearing > 50% / thickening: Tenotomy / tenodesis
Tenotomy v Tenodesis
- RCT of tenotomy v tenodesis
- no difference in outcomes / cramping / supination strength
- increased cosmetic deformity / popeye in tenotomy (33%) versus tenodesis (10%)
Ahmed et al Shoulder Elbow 2021
- meta-analysis of RCTs of tenotomy v tenodesis
- no difference in functional outcomes or strength
- increase risk of popeye deformity with tenotomy
Tenotomy
Issues
Simple
30% risk of popeye deformity
Tenodesis Options
Arthroscopic versus open
Suprapectoral versus infrapectoral
Arthroscopic suprapectoral biceps tenodesis
Technique
Vumedi arthroscopic suprapectoral biceps tenodesis video
Beach chair
- portal just anterior to leading edge of supraspinatus
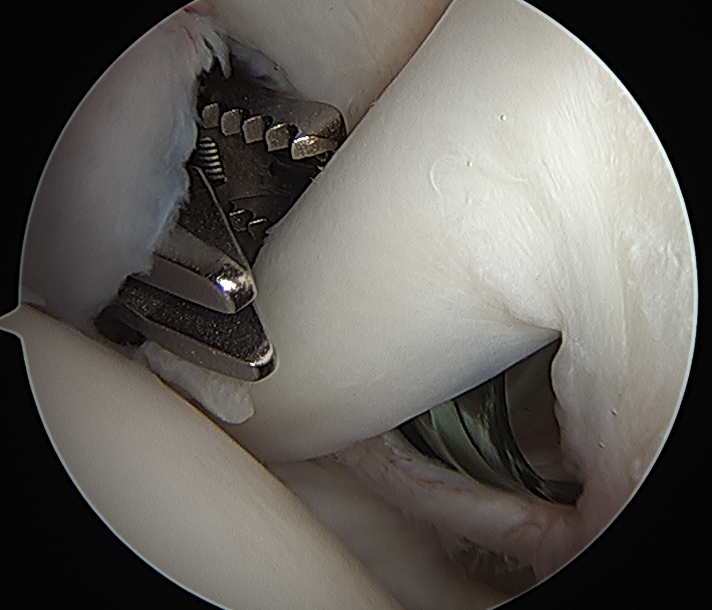
- tag biceps tendon with high strength suture and release
- repair superior labrum with one or two anchors
- anchor biceps tendon into bicipital groove
Portal just anterior to supraspinatus tendon
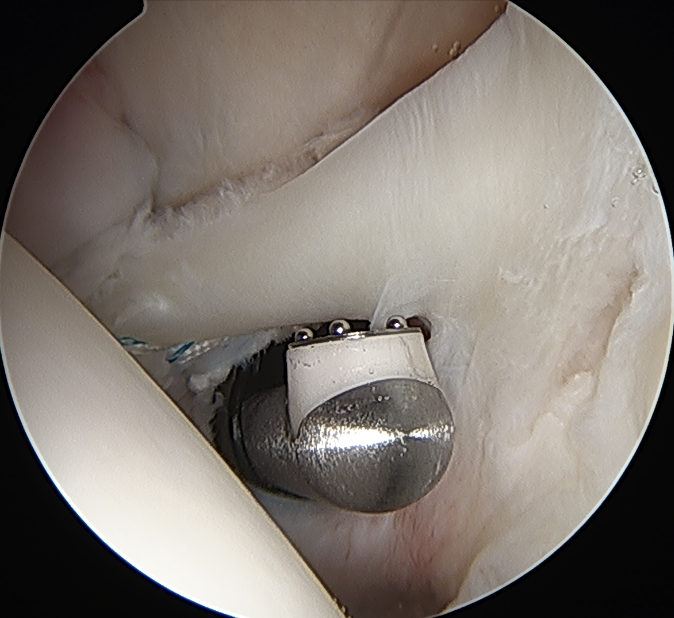
Tag biceps and release
Anchor biceps tendon into bicipital groove
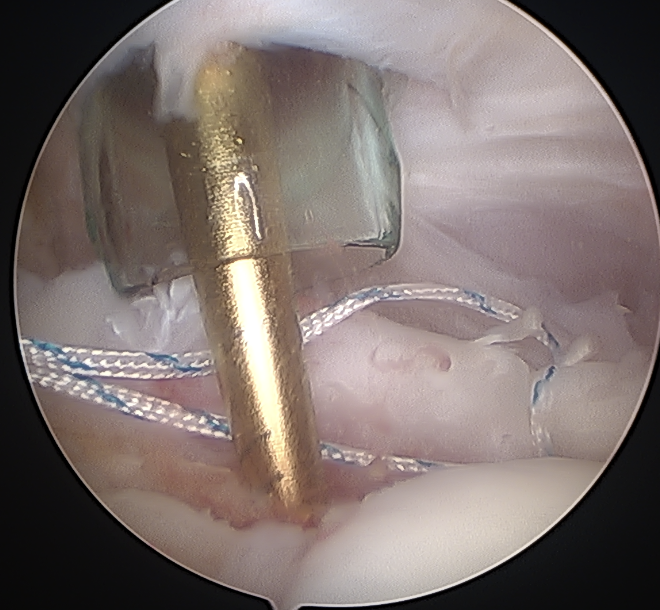
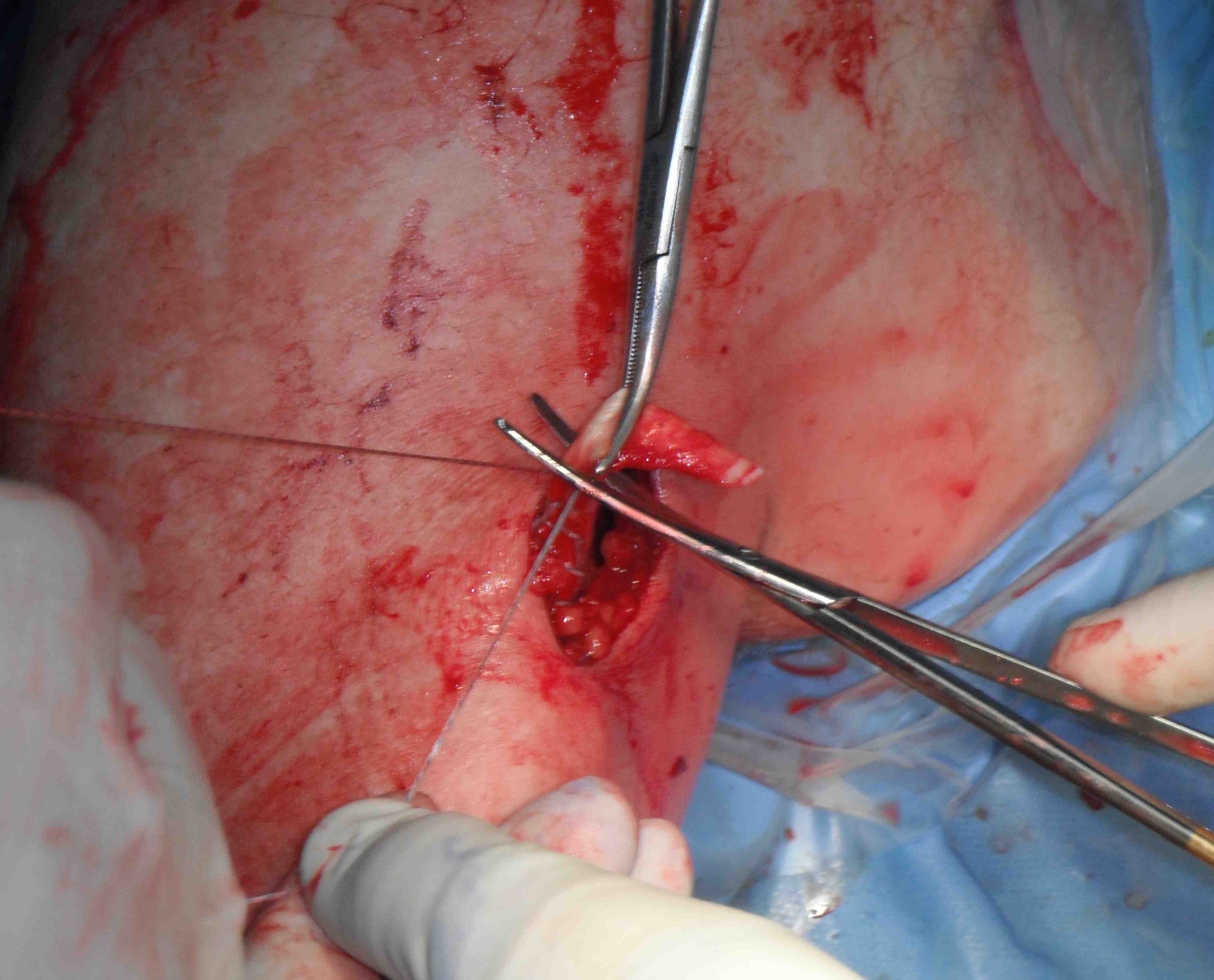
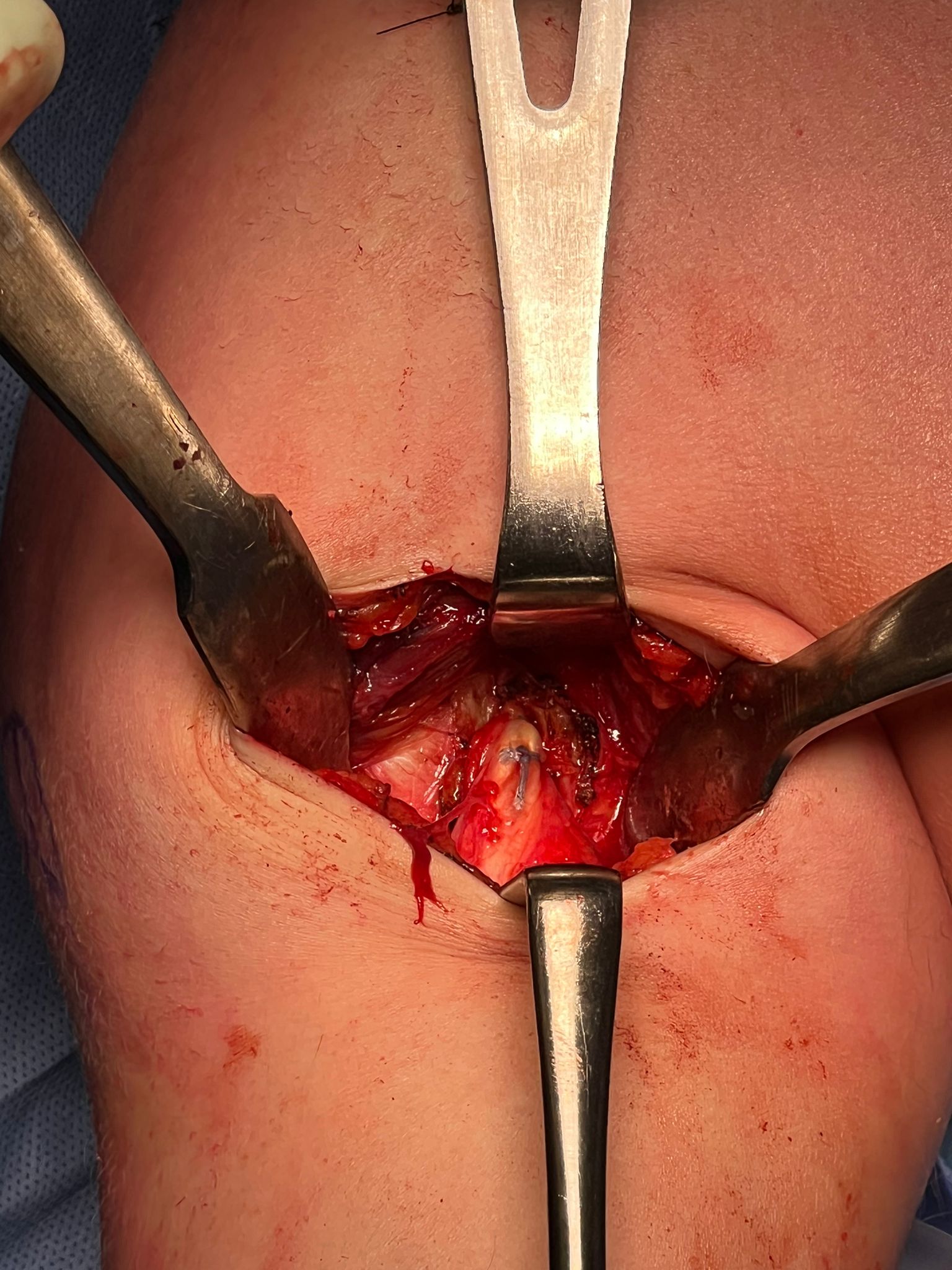
Open subpectoral biceps tenodesis
Technique
Vumedi open subpectoral tenodesis video
Arthrex subpectoral biceps tenodesis video using biceps button
Arthrex subpectoral biceps tenodesis surgical technique PDF
Beachchair
- arthroscopic biceps tendon release
- open approach to biceps
- incision centered on humerus below pectoralis tendon
- retract deltoid laterally / elevate pectoralis tendon / conjoint tendon medially
- find biceps tendon / shorten to 2cm of tendon / suture
- anchor biceps tendon


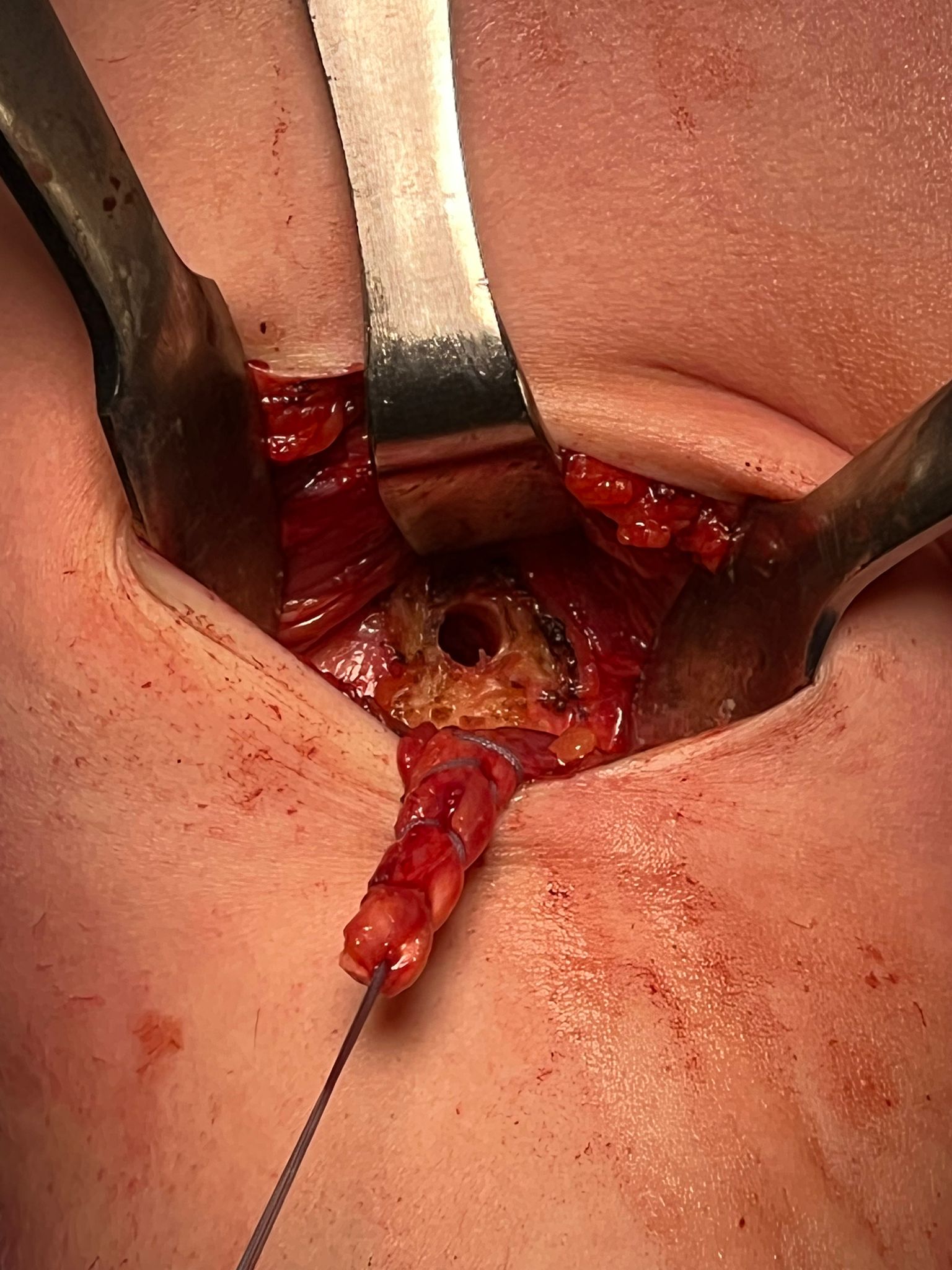
Bicortical open subpectoral biceps tenodesis using Arthrex Biceps Button