Etiology
FOOSH
Rare
Patho-anatomy
| Intrinsic | Extrinsic |
|---|---|
|
Lunate-triquetal ligament - C shaped - volar / dorsal / membranous - volar component strongest
|
Dorsal radiocarpal ligament
Palmar radio-triquetral ligament |
VISI
- lunate-triquetral ligament injury
- palmarflexion of lunate with dorsiflexion of triquetrum
Need injury to both intrinsic and extrinsic ligaments to get VISI deformity
Clinical
Ulna sided wrist pain
Swelling and tenderness over triquetro-lunate joint
Lunate-triquetral ballotment
- pisiform-triquetral with thumb and index finger
- lunate with other hand
- move them relative to each other looking for instability

Xray
Lateral xray
Palmar flexion of the lunate
Decreased scapholunate angle < 30o
MRI
Relatively low sensitivity versus arthroscopy
Likely better with 3T MRI
Arthroscopy
Often a dynamic instability
Need arthroscopy to diagnose
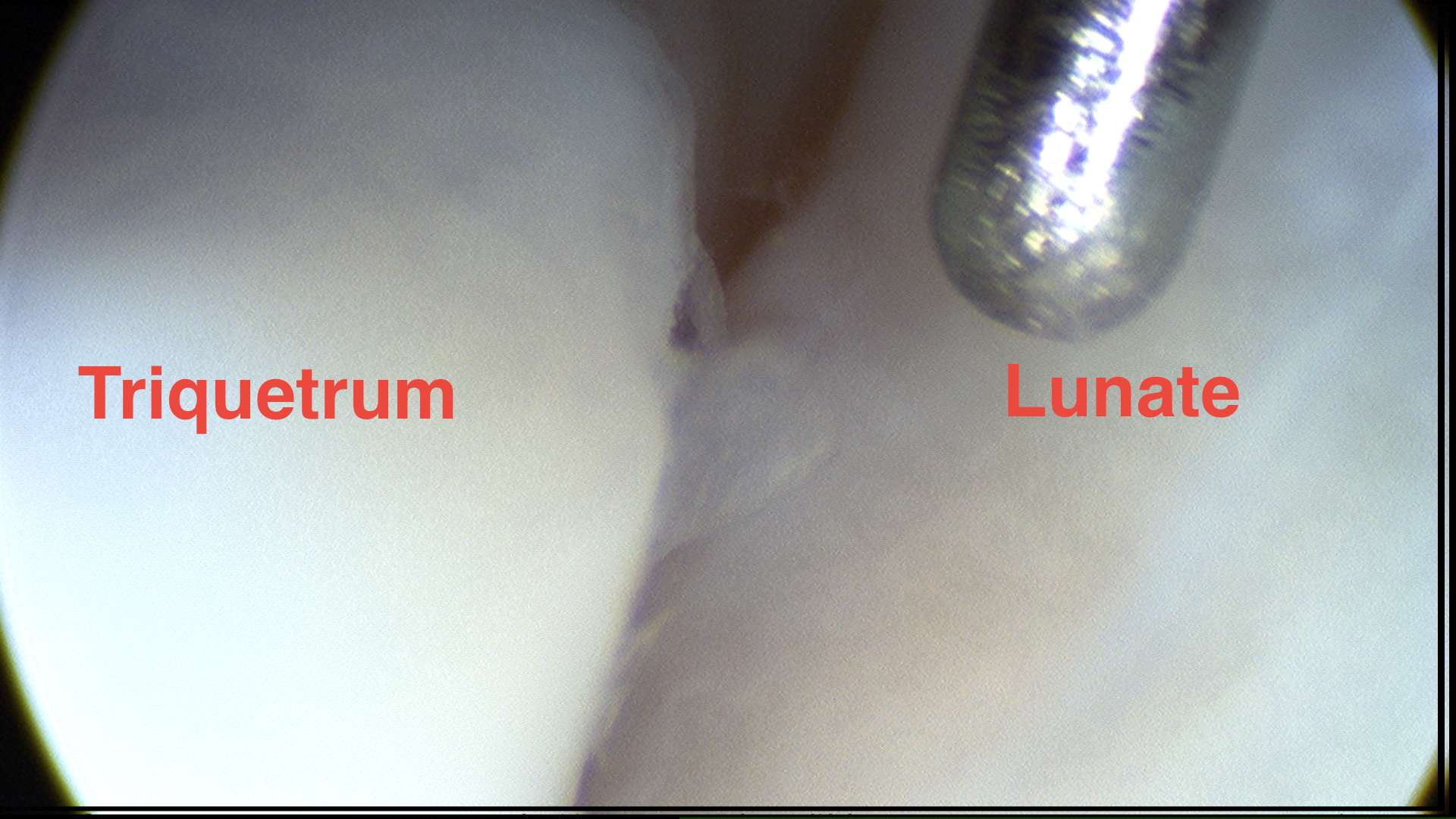
Normal lunate-triquetral ligament at midcarpal arthroscopy
Operative management
Options
Acute
- Repair +/- Reconstruction
- open v arthorscopic
Chronic
- reconstruction - ECU / palmaris longus / internal brace
- capsulodesis
- lunotriquetral arthrodesis
- ulna shortening osteotomy
Results
Lunotriquetral arthrodesis
Guidera et al J Hand Surg Am 2001
- 26 LT arthrodesis with K wires and bone graft
- 100% fusion
- ROM 80%
- good pain relief in 83%
Nickel et al J Wrist Surg 2022
- 28 LT arthrodesis with screw and bone graft
- 86% union rate
ECU reconstruction
- 46 patients with ECU reconstruction / tenodesis
- 87% satisfied
Reconstruction v arthrodesis
De Smet et al Acta Chir Belg 2005
- arthrodesis: 8/17 (47%) satisfied
- reconstruction with ECU: 8/13 (62%) satisfied
- 57 patients treated with repair v reconstruction v arthrodesis
- 5 year follow up
- best results with reconstruction
- lowest reoperation at 5 years with reconstruction: reconstruction 31%, repair 76%, , arthrodesis 78%
Technique


Dorsal approach
- 3/4 extensor compartment
- capsulotomy
- K wires into lunate and triquetrum to restore joint
- K wire LT joint
- repair ligament with intra-osseous sutures
+/- reconstruct with half of ECU
- additional incision over ECU
- radial half of ECU, 6cm, leave attached distally
- 4-5 mm drill holes in triquetrum and lunate
- pass through drill holes, reduce and K wire
- suture back to itself
+/- internal brace
AO surgery foundation LT ligament repair
LT repair + internal brace PDF
Arthroscopic repair LT ligament PDF
Arthroscopic assist ECU reconstruction PDF