


Epidemiology
Very rare
0.5% of all pediatic fractures
High energy trauma
Anatomy
Ossification
Appear: head 5-6 mths (1year), greater trochanter 2-5 years (5), lesser trochanter 9-13 years (9)
Fusion: females 14, males 16
Blood supply
Medial circumflex artery - major blood supply, posterior along femoral neck
Lateral circumflex artery - anterior, supplies little blood
Delbert Classification
| Type 1 | Type 2 | Type 3 | Type 4 |
|---|---|---|---|
|
Transepiphyseal separation
|
Transcervical fracture | Basicervical | Inter-trochanteric fracture |
|
Rare Associated with hip dislocation
|
Commonest 50% |
Second most common 30% |
|
|
AVN 100%
|
AVN 50% | AVN 30% | AVN 10% |
Management
Issues
Surgical timing
AlKhatib et al Int Orthop 2019
- systematic review of 231 cases
- < 24 hours fixation v > 24 hours fixation
- no difference in AVN rates
- still generally supports urgent treatment for displaced pediatric NOF fractures
Capsulotomy
Issue of hematoma decompression potentially reducing AVN risk
- naturally occurs with open reduction
- ? aspirate hip with closed reduction
- little evidence to support
Closed reduction
FATI CAR
- Flexion / Adduction / Traction / IR
- Circumduction / Abduction
- Reduction check in extension
- "Foot in Palm Test"
- if sufficiently reduced will sit without ER
Open reduction

Indication
Failure to obtain an adequate closed reduction
Hafez et al J Pediatr Orthop B 2025
- systematic review of 700 cases
- open versus closed reduction
- no difference in rates of AVN / nonunion / coxa vara
Watson Jones approach
Interval between TFL and gluteus medius
- harder approach to hip / more difficult reduction
- can use same approach to apply fixation
AO surgery foundation Watson Jones PDF
Vumedi surgical Watson Jones technique
www.boneschool.com/hip/displaced-hip-fractures-young
Smith Peterson
Interval between TFL and sartorius
- better approach to the hip / easier reduction
- separate approach for fixation
AO surgery foundation Smith Peterson PDF
Vumedi technique Smith Petersen
www.boneschool.com/hip/displaced-hip-fractures-young
Fixation
Type I / II - cannulated screws
Type III / IV - plate and screws


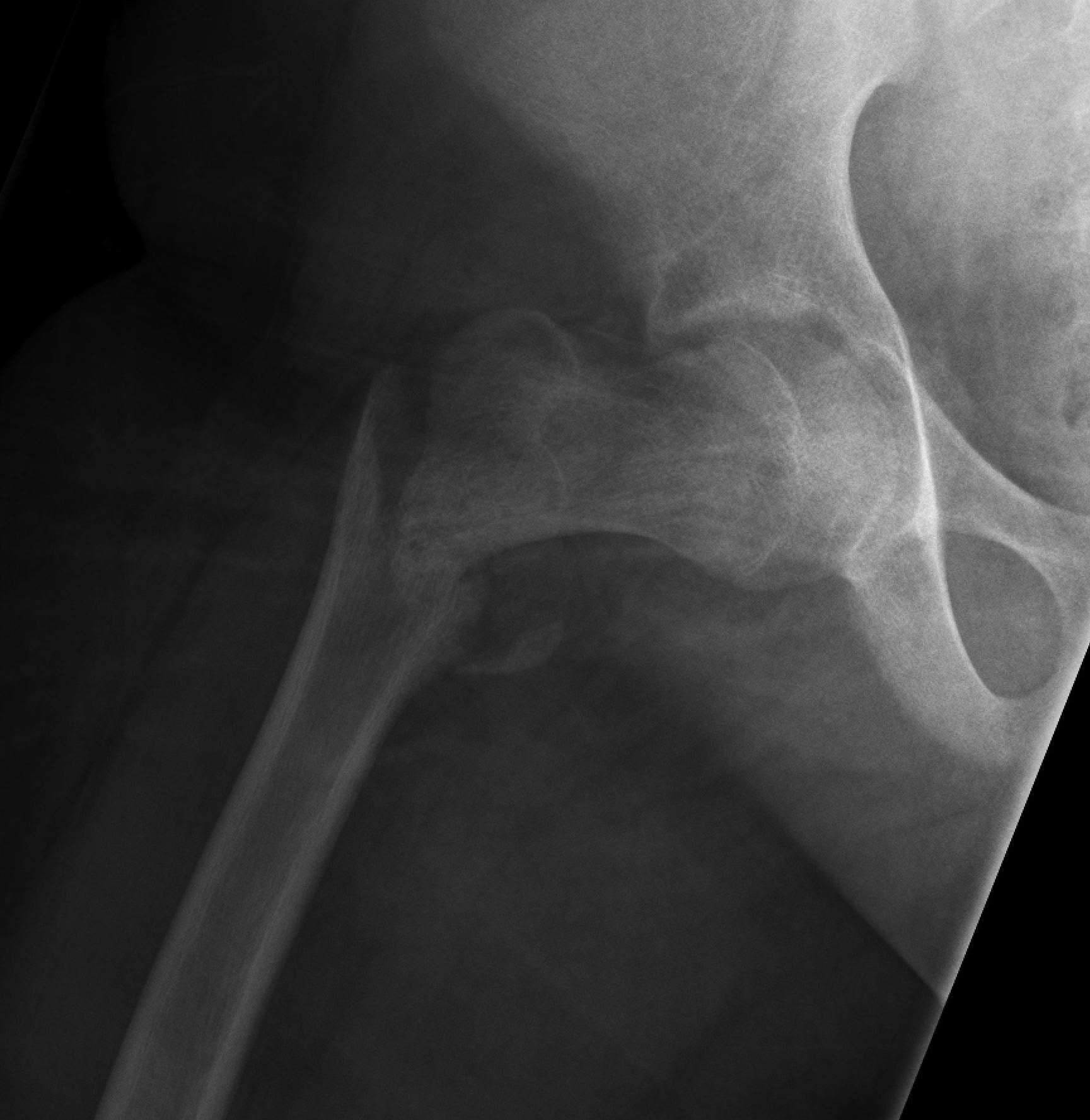
Type II fixation with cannulated screws

Type III fixation with plate and screws
Cannulated screws
Wang et al J Paediatr Orthop 2022
- 153 cases
- increased AVN with 3 rather than 2 cannulated screws
- increased AVN with larger screws
- increased AVN with screws closer to piriformis fossa / blood supply
Cannulated screws versus plate and screws
Chen et al J Pediatric Orthop 2026
- systematic review of 950 cases
- reduced AVN and growth plate closure with plate and screws in Type III /IV
Crossing physis with fixation
Indicated if needed for fracture stability
- risk is growth plate closure and leg length discrepancy
- avoid < 10 years old
- risks of loss of fixation > risks of leg length discrepancy
Complications
Types
Pandey et al J Clin Orthop Trauma 2020
- systematic review
- AVN 28%
- nonunion 6%
- coxa vara 14%
- premature growth plate closure 10% / leg length discrepancy > 1 cm 7%
AVN
Risk factors
Dong et al J Orthop Surg Res 2025
- systematic review of risk factors for AVN
- Type I / II
- older patients
- increased displacement
- poor reduction
Outcomes
Xin et al J Orthop Surg Res 2020
- systematic review of 200 cases pediatric AVN following fracture
- 65% collapsed
- 60% symptomatic
Management
www.boneschool.com/pediatrics/hip-AVN
Nonunion
Risk factors
Wang et al Orthop Traumatol Surg 2022
- 177 cases of pediatric NOF fractures
- nonunion associated with initial displacement, comminution, and poor reduction
- union usually occurred in first 6 months
Management
Inter-trochanteric or subtrochanteric valgising osteotomy +/- bone graft
- 9 cases of pediatric NOF nonunion
- all association with bone resorption and AVN
- treated with valgus inter-trochanteric osteotomy
- union achieved in all 9 cases
Growth arrest / leg length discrepancy
Management
Contra-lateral distal femoral epiphysiodesis
Coxa Vara
www.boneschool.com/pediatrics/coxa-vara