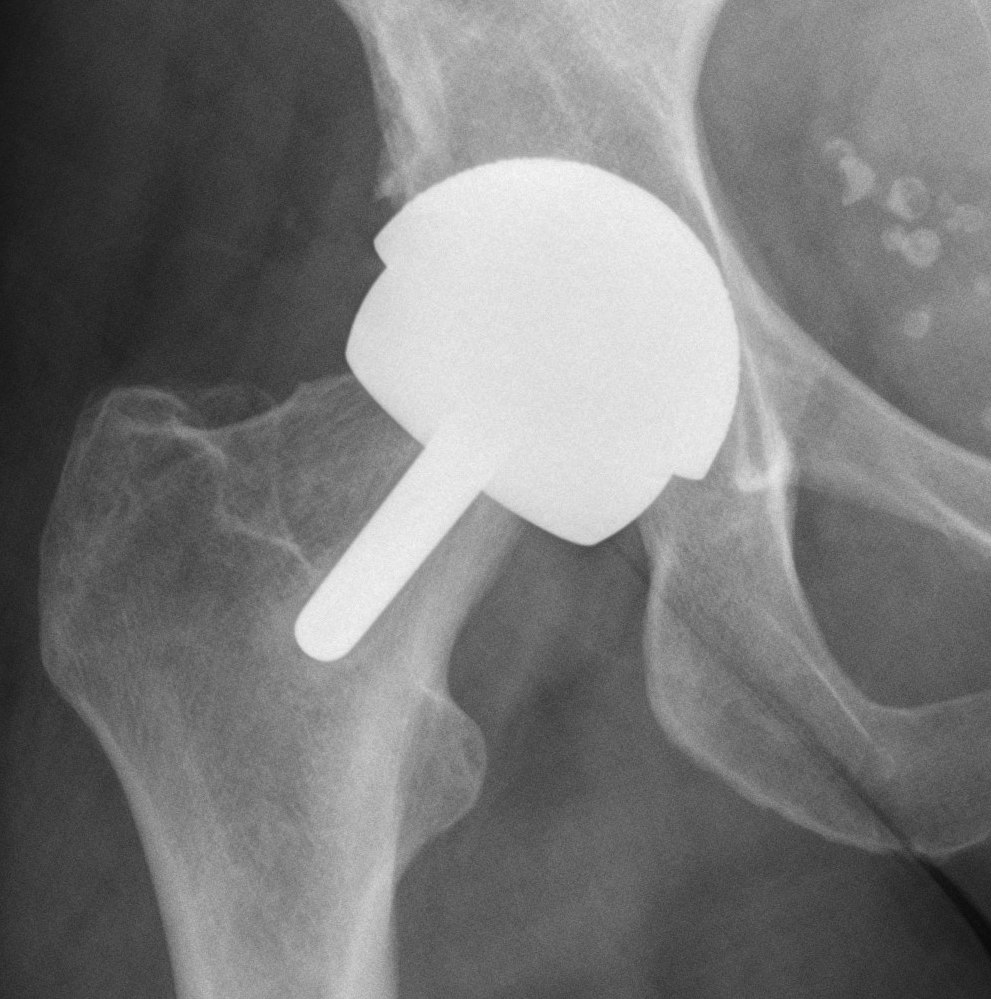

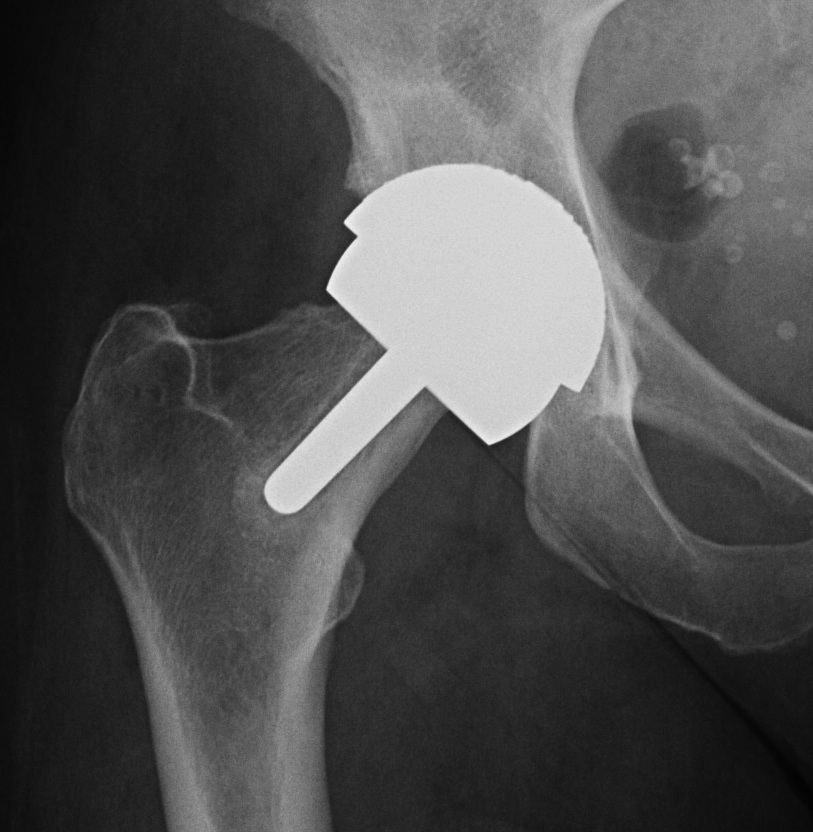
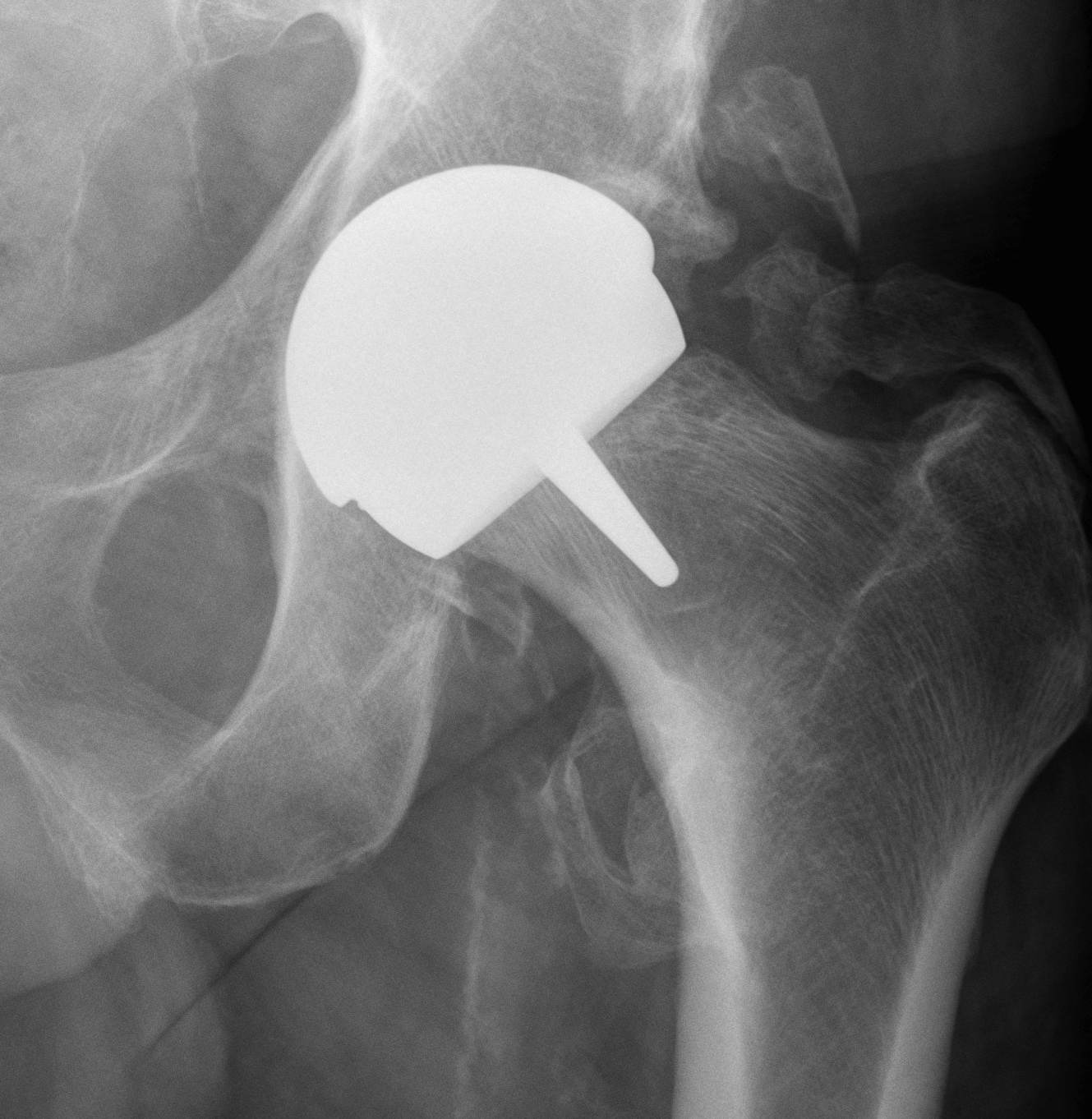
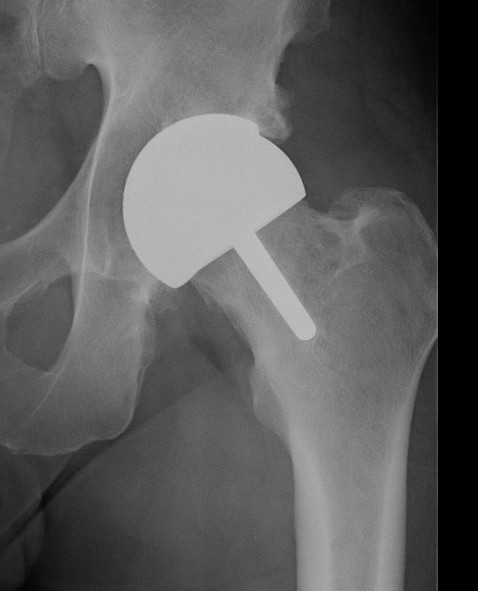
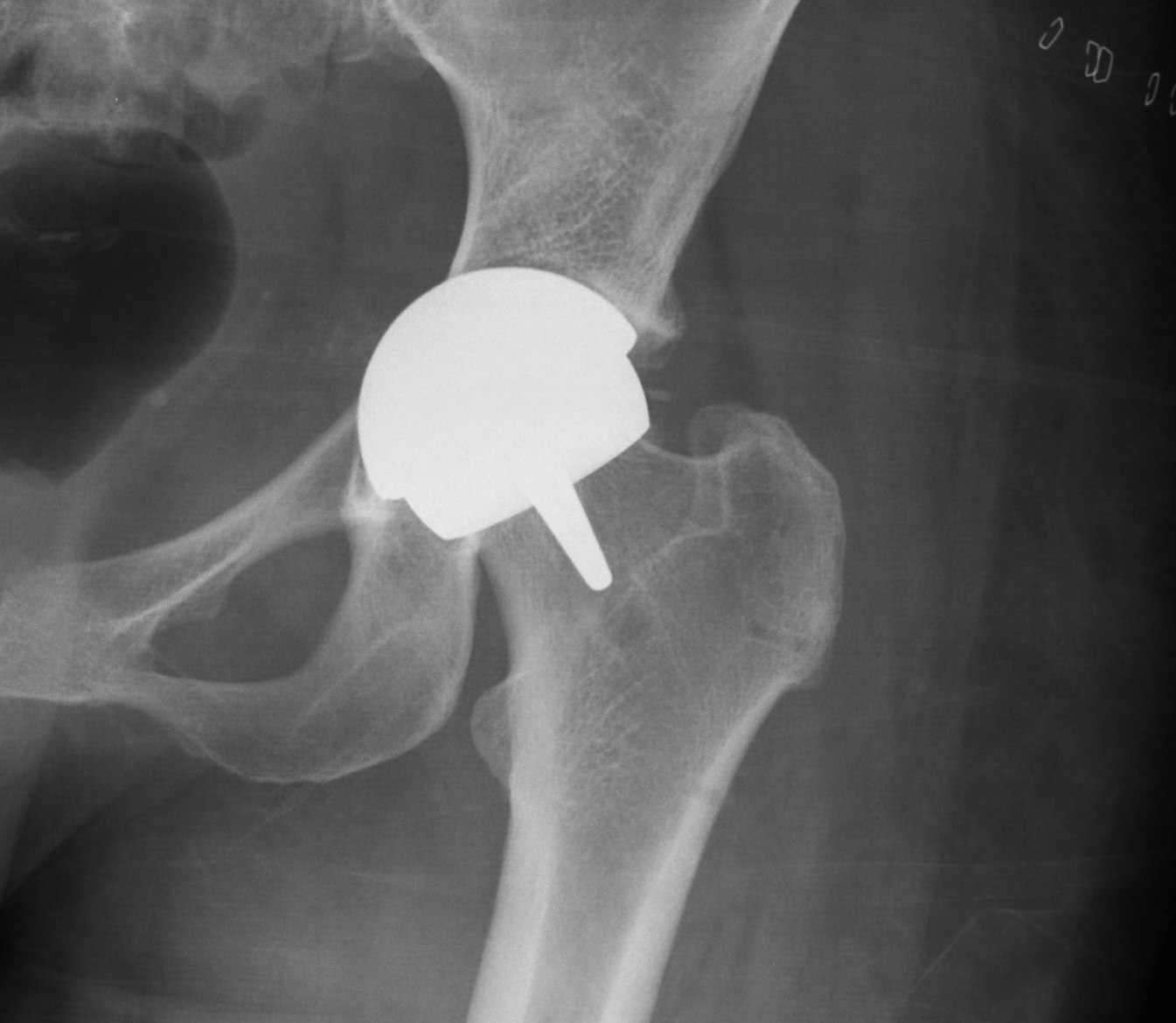
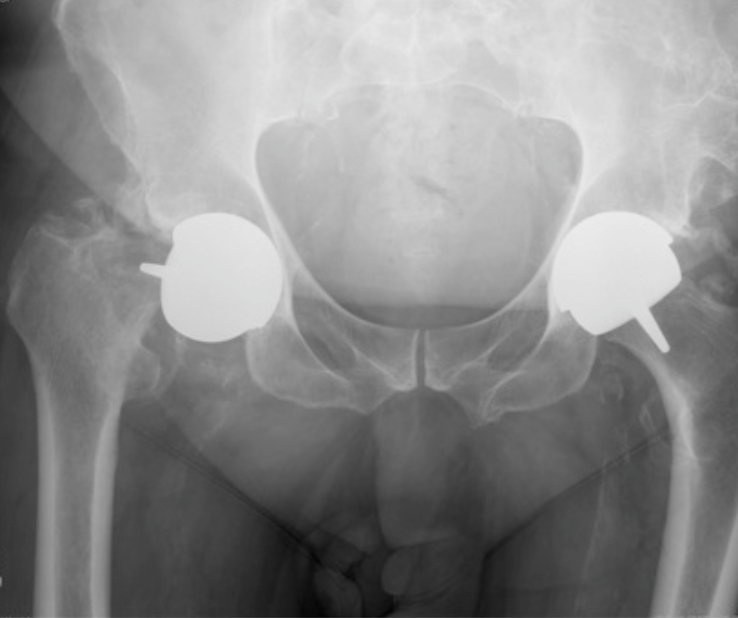
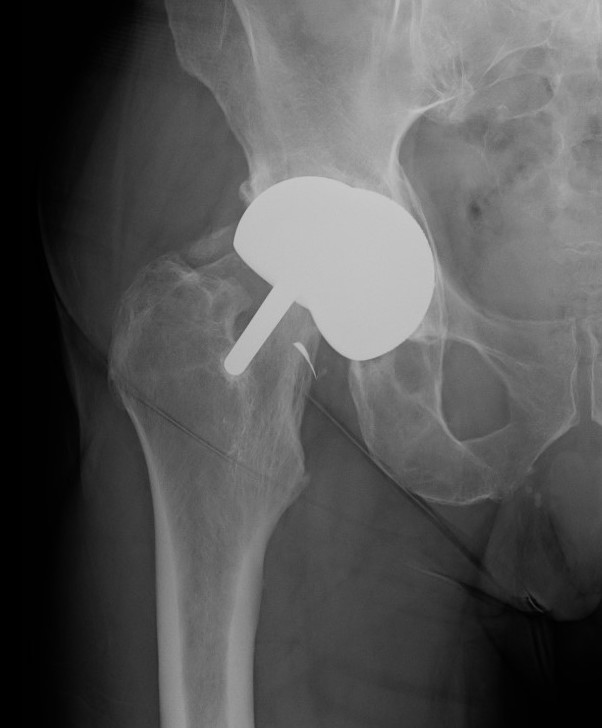
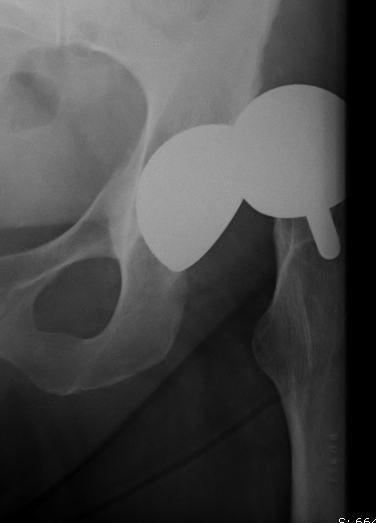
Birmingham hip resurfacing
Concept
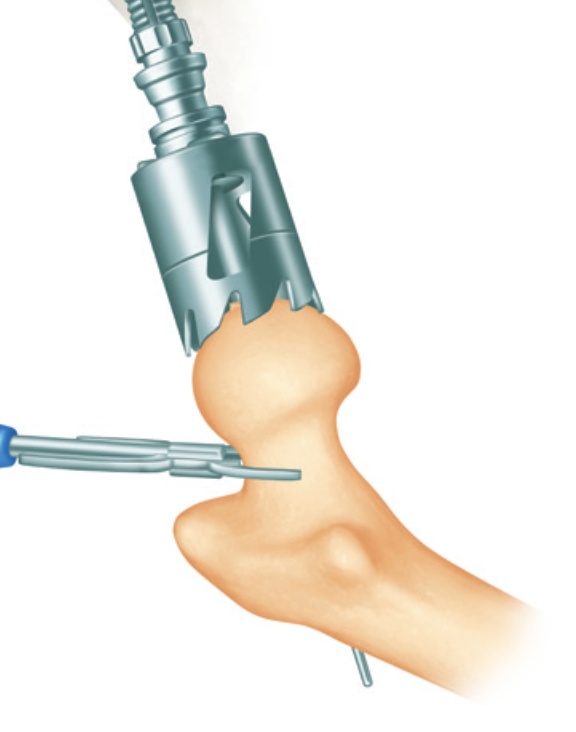
Femur - removal of femoral head cartilage and resurfacing with metal
Acetabulum - standard technique
Bearing surface - metal on metal
Potential advantages
1. Femoral bone stock preservation
2. Increased stability with large heads
3. ? Improved function
Domb et al J Arthroplasty 2021
- 50 BHR matched to 50 conventional THA
- no difference in outcome or forgotten joint score
- 50 BHR compared to 50 hybrid THA
- improved outcome scores and more active patients with BHR at 9 years
Disadvantages
1. Poor modularity - difficult to adjust LLD or offset
2. Access to acetabulum more difficult
3. Metal ions - adverse local tissue reactions / teratogenesis
Australian Joint Registry 2023
20 year revision rate 20,000 hip resurfacing
- resurfacing 11%
- conventional THA 8%
In 2022
- resurfacing was 80% less common than in 2005 / 0.7% of all THA
- 97.5% performed in males
| Diagnosis | 20 year revision % |
|---|---|
| OA | 11 |
| DDH | 19 |
| AVN | 16 |
| Prosthesis | 15 year revision % |
|---|---|
| Adept | 6.5 |
| Birmingham | 9.5 |
| Head size mm | 20 year revision % |
|---|---|
| < 45 | 31 |
| 45-49 | 15 |
| 50-54 | 8 |
| > 55 | 6 |
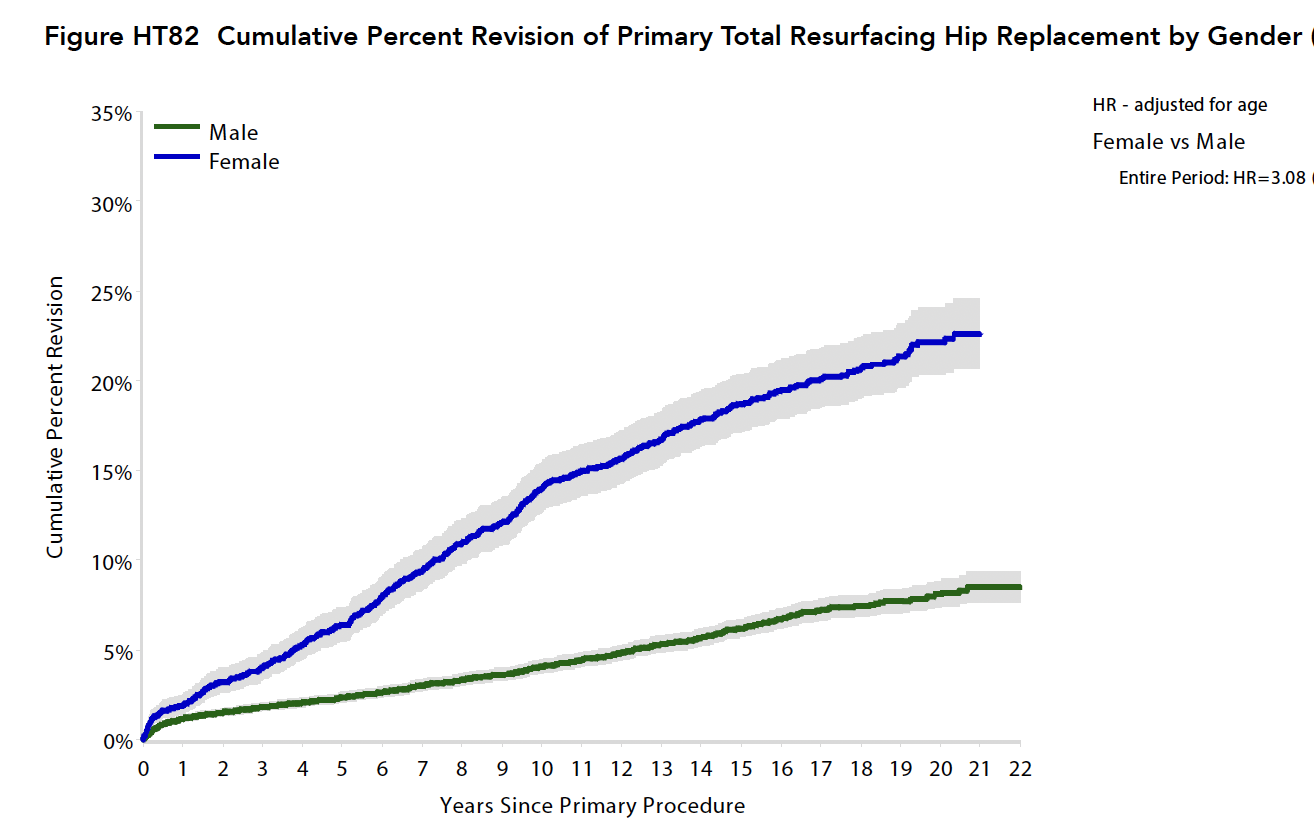
| Male | Female | |
|---|---|---|
| 5 year | 2.3 | 6.4 |
| 10 year | 4.1 | 14 |
| 15 year | 6.2 | 18.7 |
| 20 year | 8.1 | 22.1 |
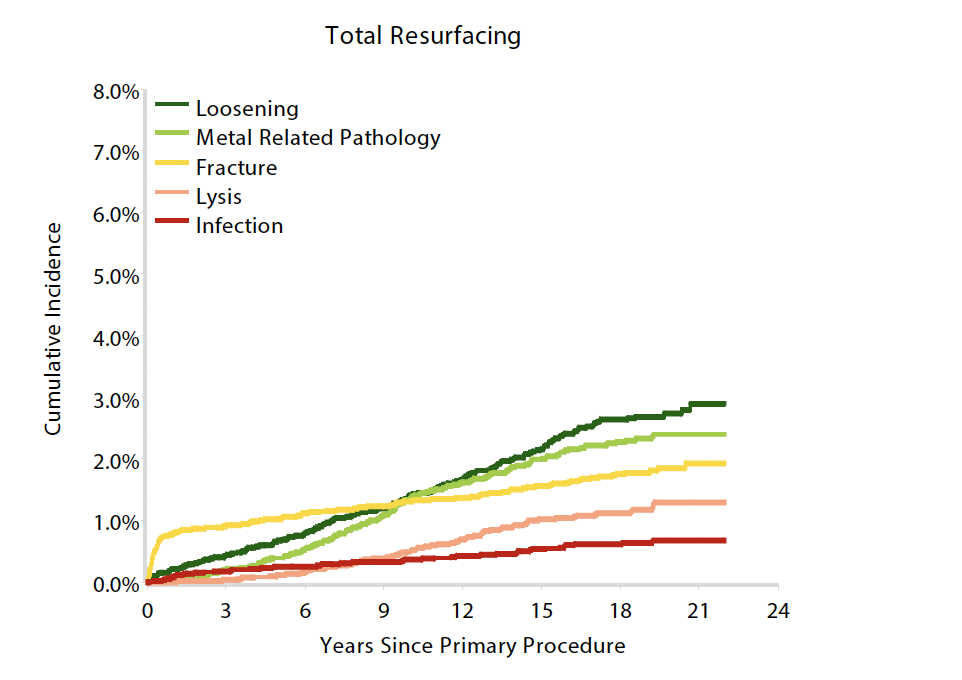
Indication for revision
Technique
Indications
Male / OA / good bone stock / large femoral head size
Contra-indications (from: Birmingham hip resurfacing technical guide)
| Absolute | Relative |
|---|---|
| Female | Osteoporosis |
| Cysts > 1 cm | Age > 65 |
| AVN > 50% | BMI > 35 |
| < 50 mm templated head | |
| Known metal sensitivity - jewelry | |
| Impaired kidney function - metal ions |
|
Techniques
Birmingham Resurfacing
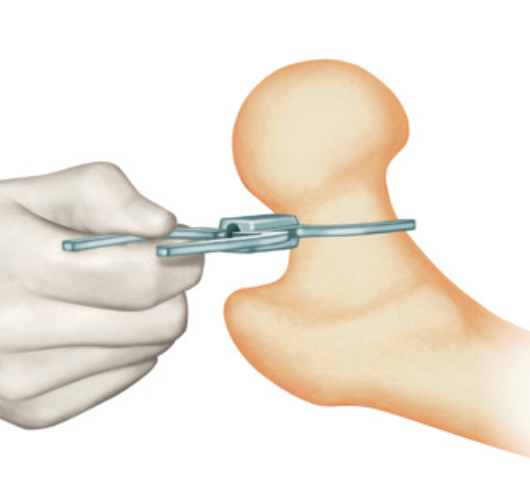
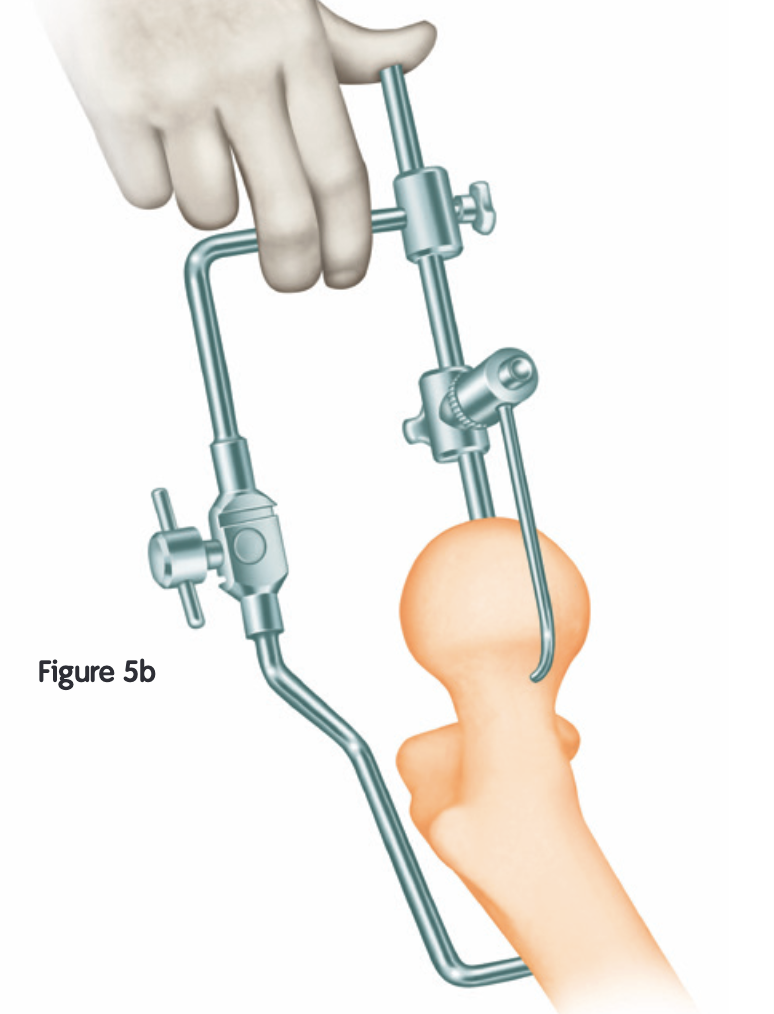
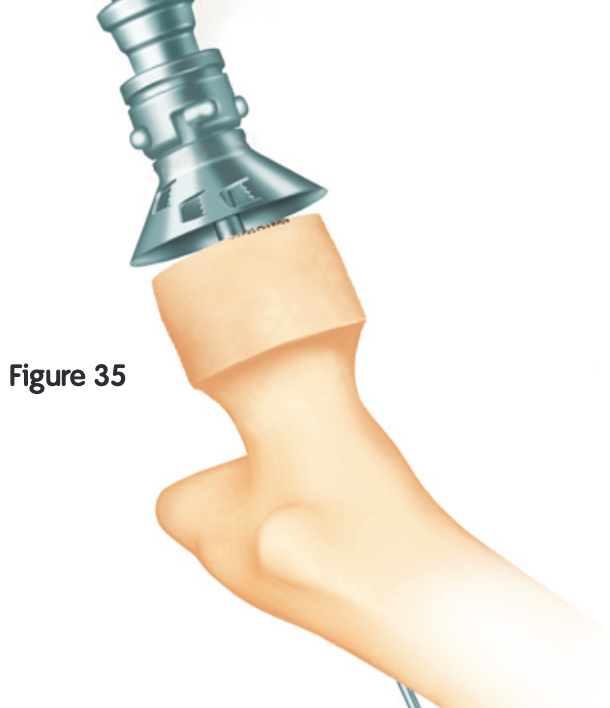
Smith&Nephew Birmingham Resurfacing PDF
Avoid
- notching
- varus
- open acetabulum
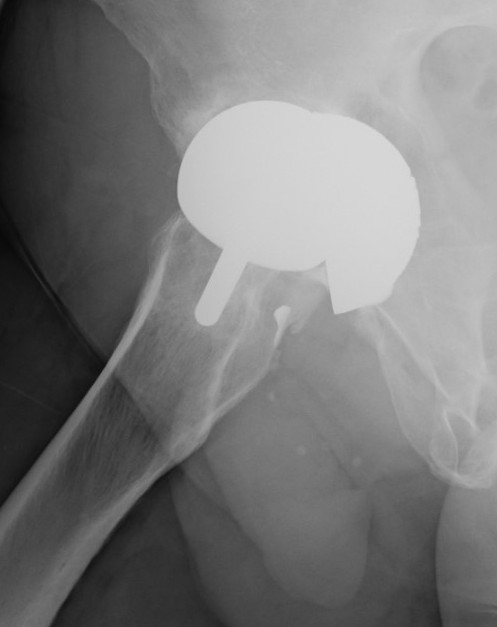
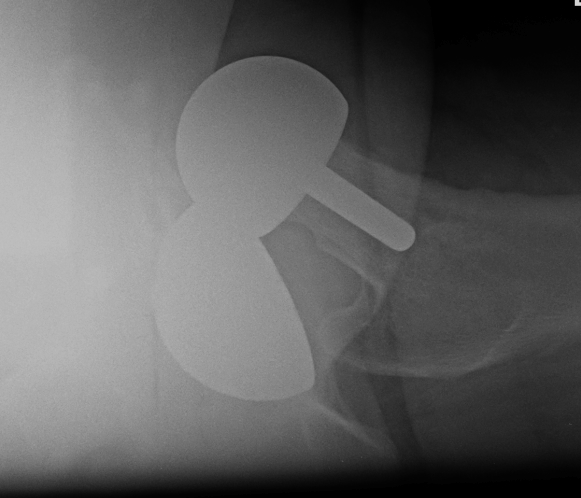
Technical issues

Oversized head

Varus Femoral Component

Femoral head notching

Open Acetabular Component - may cause point loading and increased metal wear
Navigation
Vumedi custom guides Birmingham resurfacing
Metal on Poly Hip Resurfacing
Vumedi video metal on poly hip resurfacing
Complications
Femoral Neck Fracture
Risk Factors
- decreased bone mass / osteoporosis / elderly / inflammatory arthritis / AVN
- females
- femoral head and neck cysts
- femoral neck notching
- varus femoral component
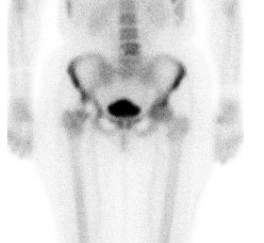
Metallosis
Malloy et al JBJS Open Access 2024
- systematic review of 2,100 BHR at minimum 10 years
- 95% survival
- 20% of revisions for loosening, 20% for metal reaction
Aseptic loosening
Issue
- cannot revise to metal on metal
- need to revision acetabular component as well
- revision of 53 hip resurfacing
- 10 year survival 63%
- worse outcomes with revision of metallosis
- worse outcomes with femoral revision only to MoM bearing
- Australian Joint Registry of 884 resurfacings undergoing revivision
- 10% re-revision rate of 26%
Instability
Femoral head AVN
Due to extensive releases required to expose / surgically dislocate femoral head