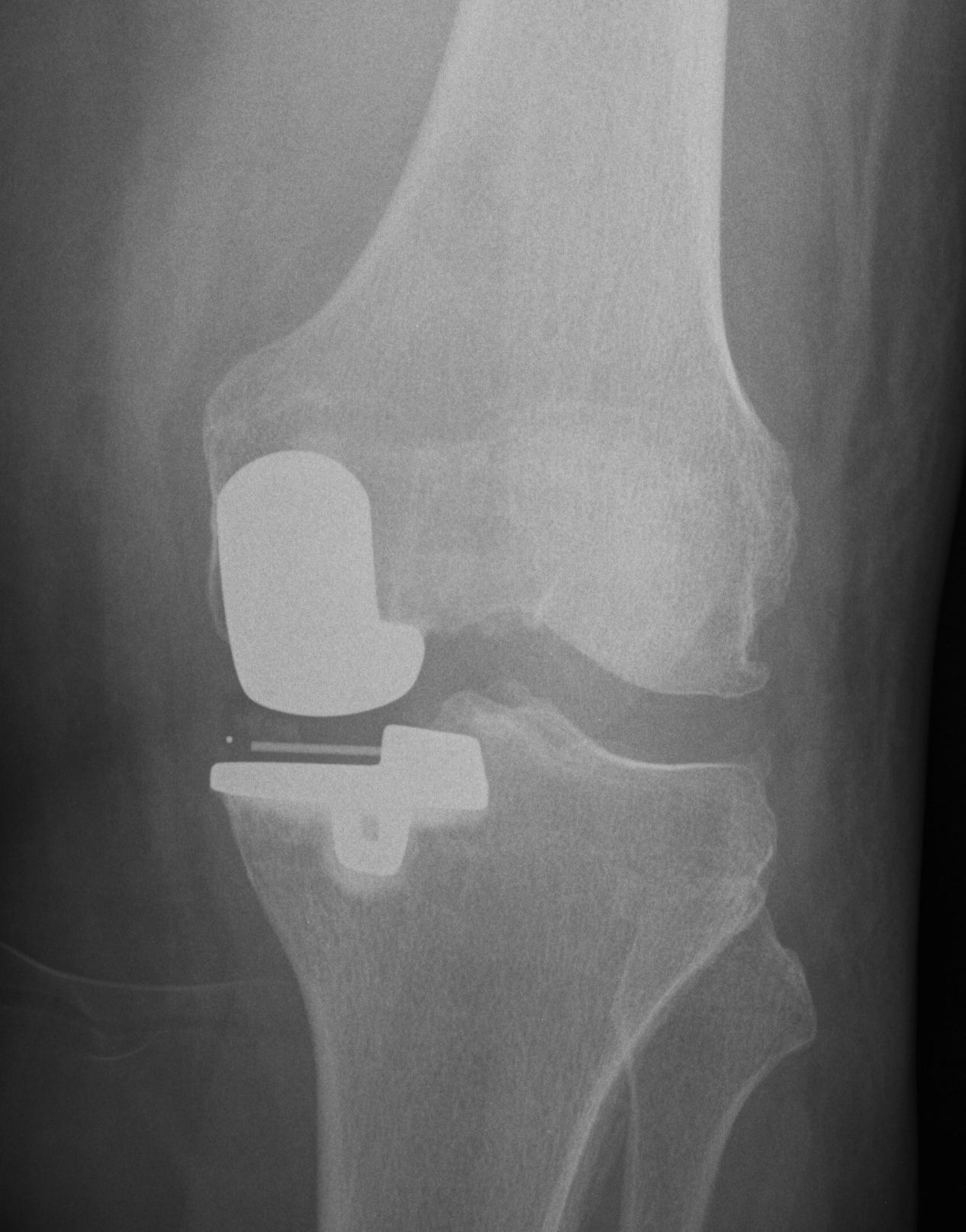
Patella Resurfacing
Options
1. Always resurface
2. Never resurface
3. Selectively resurface
Decision Making
Controversial
- literature divided on issue
Historically
- poor outcomes due to poor implant design
- now improved designs
- non resurfacing also improved due to better design and improved techniques in regard to tracking and rotation