Talar Neck Complications
AVN
Largely related to degree of displacement
Incidence
Hawkins Type I
- 0% to 13%

Hawkins Type II
- 20% to 50%
- usually only patchy and not a problem (rarely collapses)
Largely related to degree of displacement
Hawkins Type I
- 0% to 13%
Hawkins Type II
- 20% to 50%
- usually only patchy and not a problem (rarely collapses)
1. Flexor Tendon Rupture
2. Adhesions
3. PIPJ contractures
4. Triggering
5. Pulley failure
6. Quadrigia
5%
FDS only
< 20o sagittal
< 30o coronal
< 3 cm of shortening
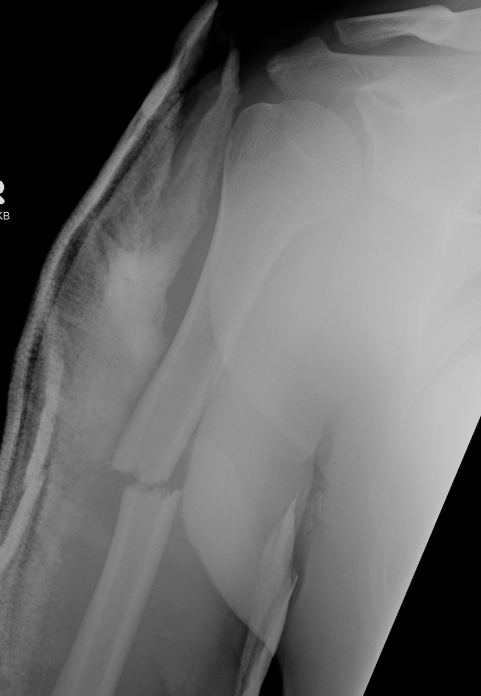


Usually a direct blow
- less commonly a fall on the outstretched hand
RTA / sporting accidents commonest causes
Can be pathological as a result of radionecrosis
- eg following radiotherapy for breast cancer.
Fractures of the clavicle are common
FOOSH
- axial load with a valgus force
1. Provides Valgus stability
- especially if MCL deficient
2. Longitudinal stability
- aided by interosseous membrane
3. Load Transfer
- 60% of load at elbow

2 groups
- young patient with high velocity injury
- older patient with comminuted, osteoporotic fracture
In the second group fixation can be very difficult
Hinged Joint
- trochlea axis is centre of rotation
- 40o anterior angulation in sagittal plane
1. Removal Loose body
2. Excison of osteophytes
- coronoid
- olecranon
- aiming to improve ROM / prevent impingement
RA
- very good results
- 97% 10 year survival Coonrad-Morrey prosthesis
Other Dx
- OA / post-traumatic arthritis / nonunion
- tend to have worse survival than RA
Haemophilia
- elbow joint commonly involved
- 90% of haemophiliacs
Acute unreconstructable fracture > 60


Parosteal OS
- bone is not continuous with cortex in MO
3% incidence in elbow joint trauma to some degree
Lateral : Medial 9:1
4th & 5th decades
- M = F
- 75% dominant arm
50% of regular tennis players
- especially > 2 hrs / week
Insertion pathology / Enthesopathy
Over-extension of the elbow with supination / pronation
Lateral epicondyle
- anconeus from posterior face
- ECRB and EDC from anterior face (CEO)