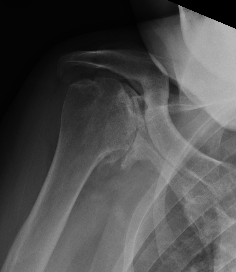

Templating
Xray
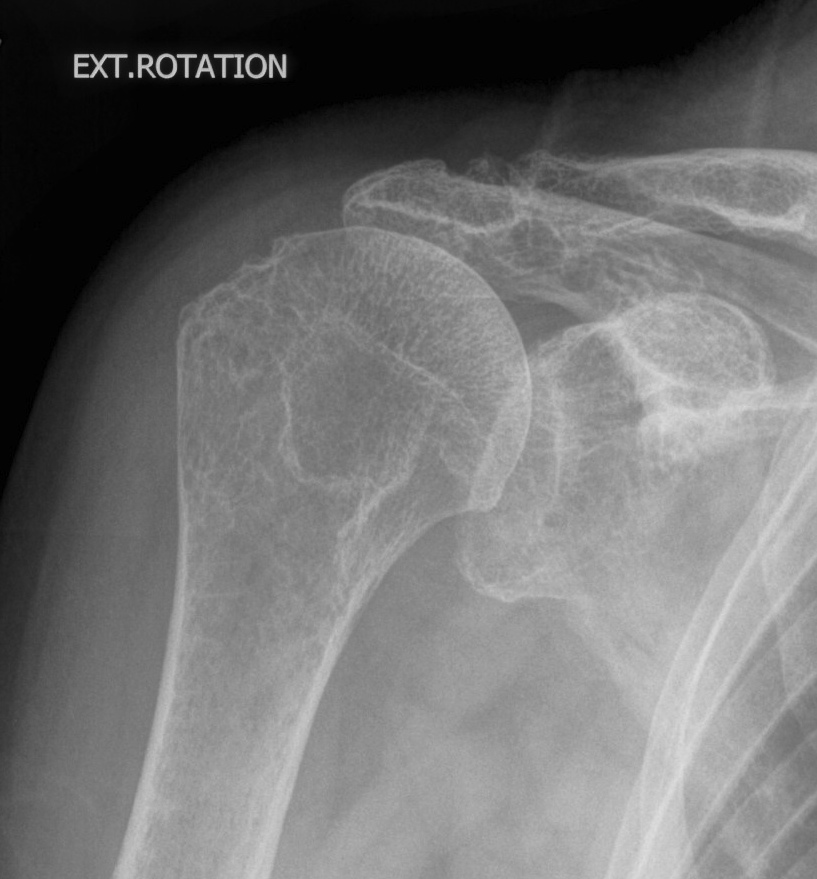
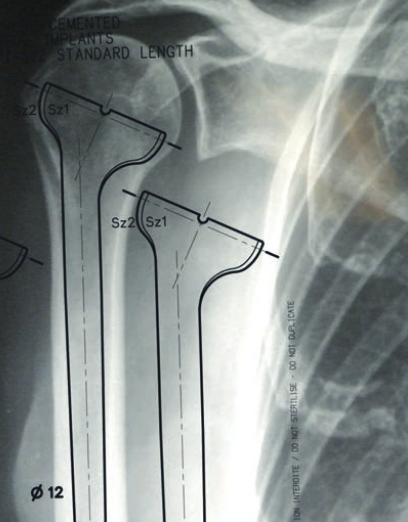
Template size and fit of glenoid & humeral components
CT scan
Axial - assess glenoid bone stock / version
Coronal - look for superior wear


CT templating
Zimmer Trabecular metal rTSA CT templating
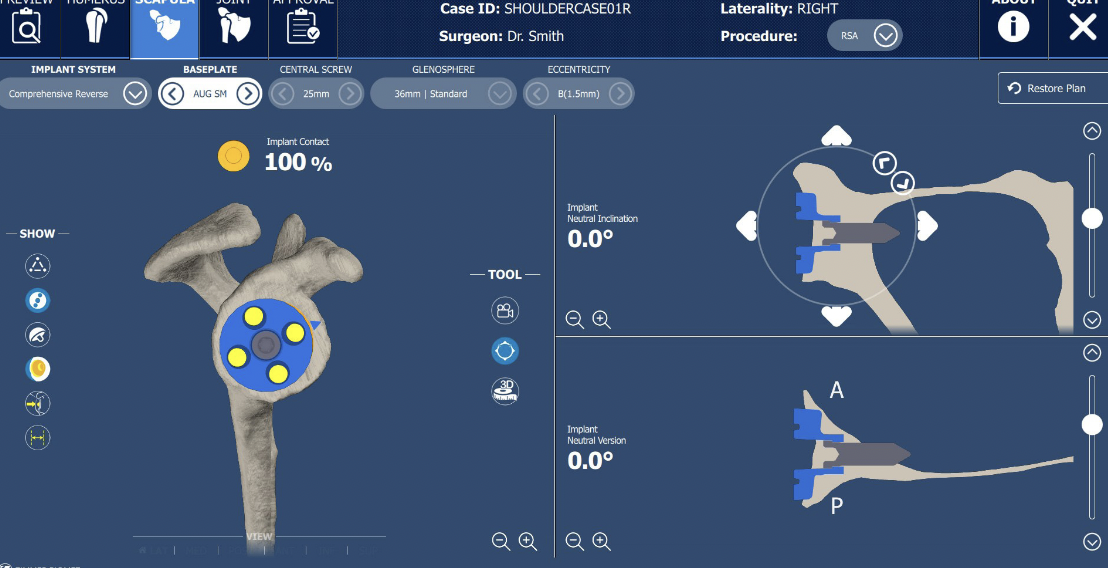

Zimmer Signature One CT templating pdf
- systematic review of use of computer assisted navigation in rTSA
- increases accuracy baseplate screw placement
- allows longer screws and better purchase
- systematic review of computer assisted navigation in rTSA
- improves inclination of the baseplate
- increases use of augmented implants
- increases surgical time
Surgical approach
Options
Deltopectoral approach
Anterosuperior approach
Deltopectoral approach
AO surgical foundation deltopectoral approach
Likely better glenoid visualization but have to divide subscapularis
Incision based upon coracoid
- identify and protect cephalic vein
- biceps tenotomy
- subscapularis tenotomy / peel / lesser tuberosity osteotomy
? Subscapularis repair
Collin et al J Should Elbow Surg 2022
- 86 patients with rTSA and repaired subscapularis tenotomy
- 2 year ultrasound - subscapularis healed in 53%
- no difference in outcome scores between healed and not healed
- improved internal rotation when healed, with no difference in external rotation
- systematic review of subscapularis repair in rTSA
- increased instability without subscapularis repair with medialized implants
- no difference with lateralized implants
- increased ROM with subscapularis repair
Superior lateral approach
AO surgical foundation deltoid split technique
Vumedi superolateral approach for rTSA in fracture
Possible poorer glenoid visualization, but can leave subscapularis intact
Incision over lateral acromion
- split anterior and middle deltoid muscle bundles
- limit 4 cm from acromion to preserve axillary nerve
- can release deltoid from anterior acromion +/- with piece of bone
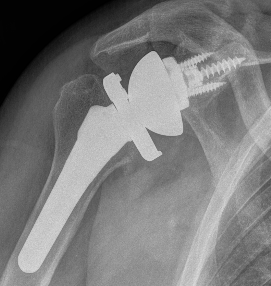
Surgical technique
Depuy Synthes Delta Xtend Reverse Surgical technique
Vumedi surgical technique rTSA with PSI / glenoid augment / offset humeral liner
Humerus preparation

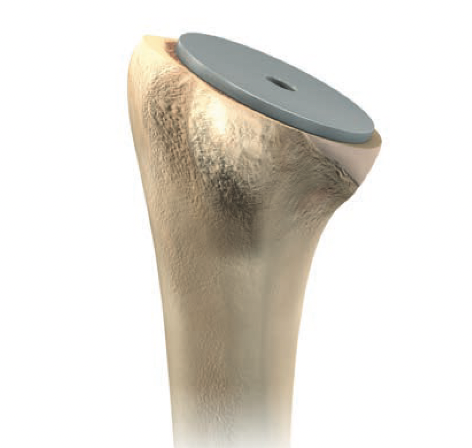
Depuy Synthes Delta Xtend
Use cutting guide for neck cut angle
Set retroversion 20°
Inlay verus onlay
Leave trial stem in to prevent fracture
Glenoid baseplate
Remove all labrum and release capsule from glenoid
- identify inferior border of scapula
- ? release triceps from inferior border
- insert retractors to expose glenoid
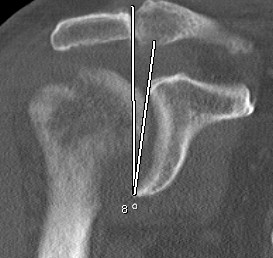
Centering guide wire passed

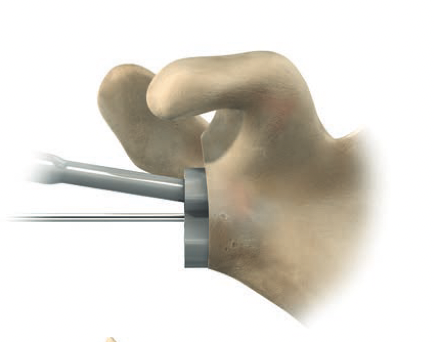
Depuy Synthes Delta Xtend
Center of inferior circle of glenoid
- metaglene needs to be positioned low to prevent inferior impingement and dislocation
- wire needs to angle perpendicular or slightly inferior / avoid superior tilt
- should exit scapula anteriorly about 3cm medial to glenoid
- ensure inferior screw will be in inferior good bone
- ream cartilage to subchondral bone
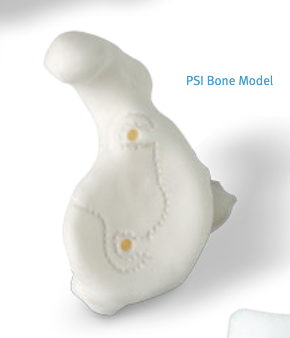
Patient specific instrumentation
Zimmer PSI Trabecular metal rTSA
Zimmer Signature One Surgical technique PDF

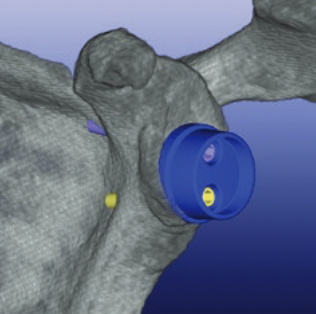
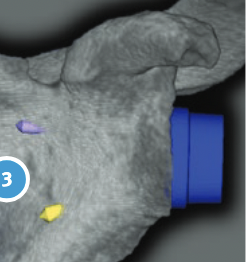
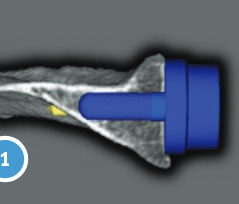
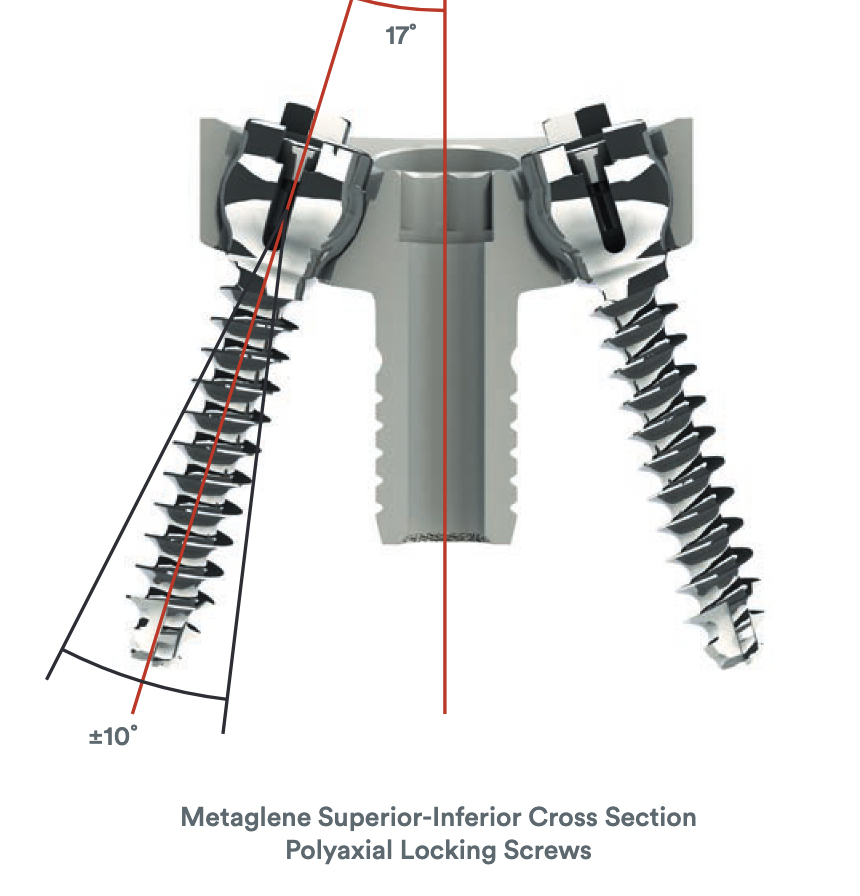
Metaglene / baseplate fixation
Screws as long as possible
- inferior screw - long into scapular pillar
- superior screw - aim for coracoid
- anterior / posterior screws - convergent / divergent

Depuy Synthes Delta Xtend

Glenosphere
Typically lateralized / slight inferior overhang
Trial components
Insert humeral stem
Trial humeral liner options
- varying offset to cover humeral head
- can medialize center of rotation
- adjust thickness for stability
Stability
- shuck test
- stable through range of motion
- no inferior impingement
Tendon transfers
Indication
Limited external rotation
Options
Latissimus dorsi
T major
Results
- RCT of rTSA +/- LD/Tmajor transfer
- no difference outcome scores
- improved external rotation rTSA 58% v rTSA+tendon transfers 73%
Hones et al Clin Shoulder Elbow 2024
- systematic review of external rotation in rTSA
- lateralized rTSA versus rTSA + LD tendon transfer
- better external rotation with lateralized rTSA
Technique
Detach latissmus dorsi
- pass anterior to posterior
- suture via drill holes to the posterior aspect of the humerus

Rehabilitation
- RCT of early v delayed ROM in 80 rTSA
- no difference in outcomes