Epidemiology
4% of cervical spine fractures
Anatomy
Bony
- Occipitoatlantal joint (C0/C1)
- poor bony congruency, relies on ligamentous stability
Ligaments
- Alar ligaments: Strong ligaments connecting odontoid to occipital condyles
- Apical ligament: Weak ligament, connecting apex of odontoid to foramen magnum
- Tectorial membrane: Continuation of PLL connecting posterior body of axis to forament magnem
Mechanism
Compression / lateral compression
High association with blunt force trauma
- seen in association with other cervical and orthopedic injuries
- high association with significant head injuries
West et al World Neursurg 2018
- 46 patients with occipital condyle fractures
- 30% had intra-cranial injuries
- 43% had significant other cervical spine injuries
Symptoms
Skull base pain
Cranial nerve injury / hypoglossal nerve injury
- hypoglossal canal in close proximity
- slurred speech, difficulty swallowing
- can be delayed presentation
Classification Anderson & Montesano
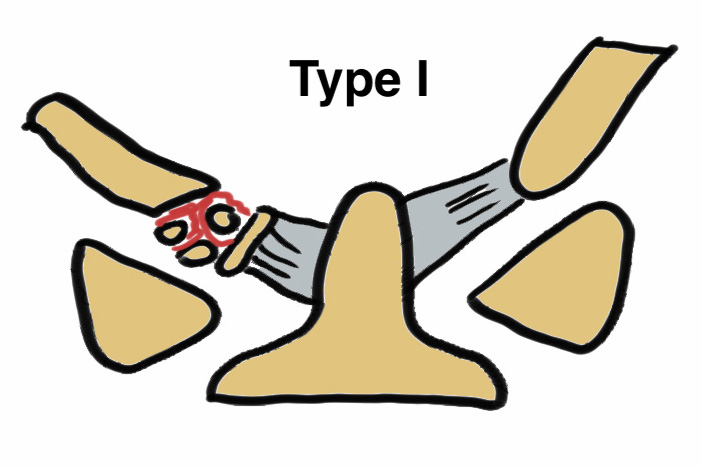
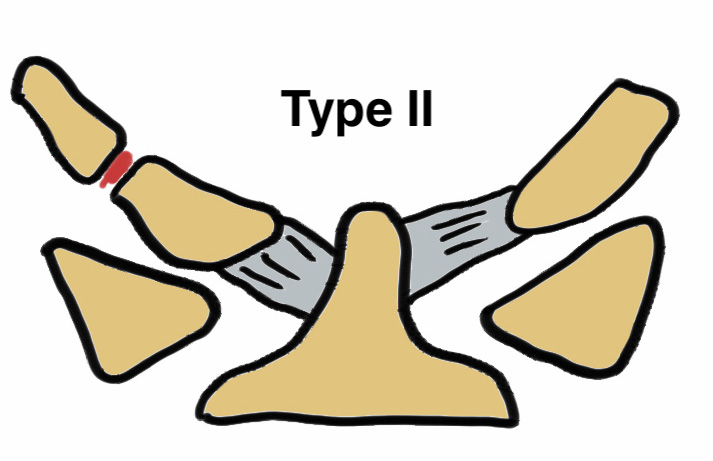
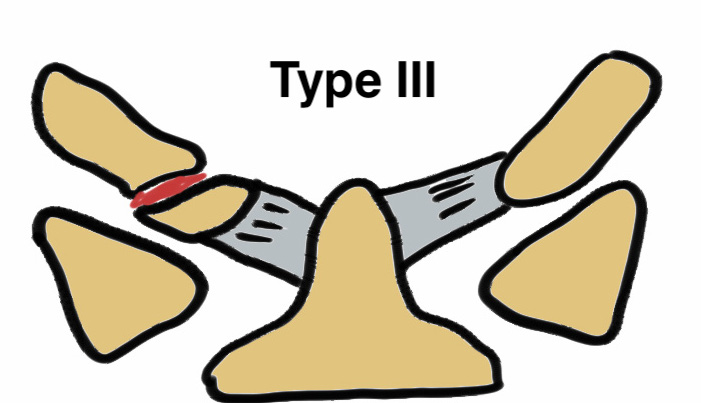
| Type | Description | Management |
|---|---|---|
| Type I | Condyle impaction without displacement | Collar |
| Type II | Condyle fracture associated with basal skull fracture / involvement of the foramen magnum | Collar |
| Type III | Infero-medial condyle avulsion fracture secondary to alar ligaments | Halo-thoracic brace |
- 95 patients with 107 occipital condyle fractures
- 77% unilateral occipital condyle fractures
- 75% type III
- associated cervical spine injuries seen in 31%
- 10/95 died
Xray
Frequently misses this injury
CT


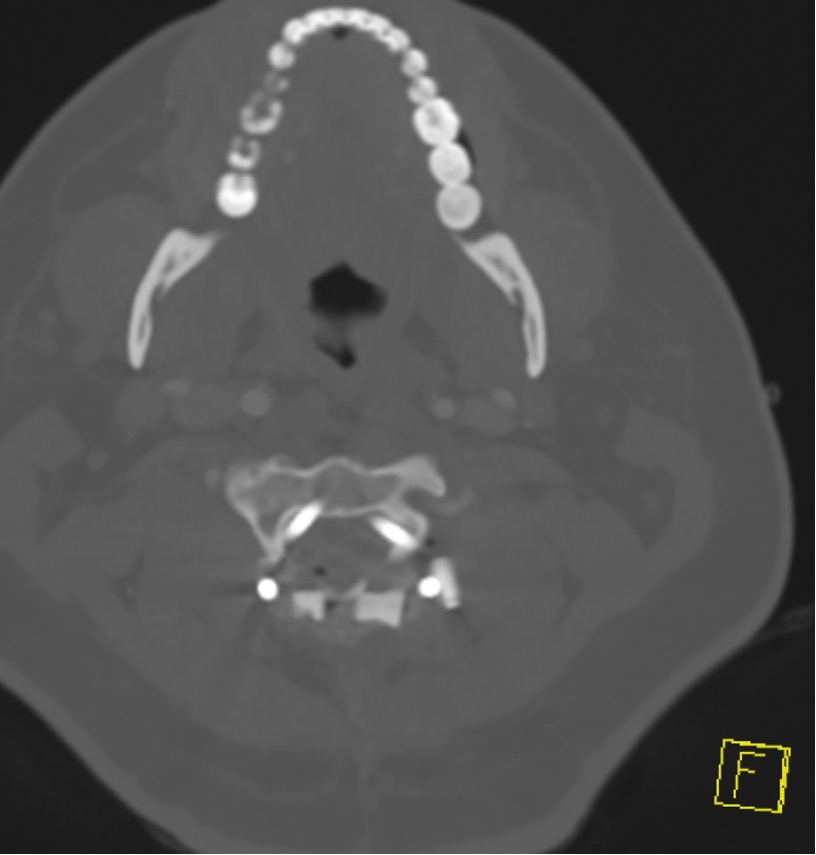
Type II: Occipital condyle fracture involving base of skull
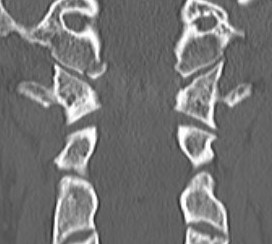
Type III: Inferomedial alar ligament avulsion

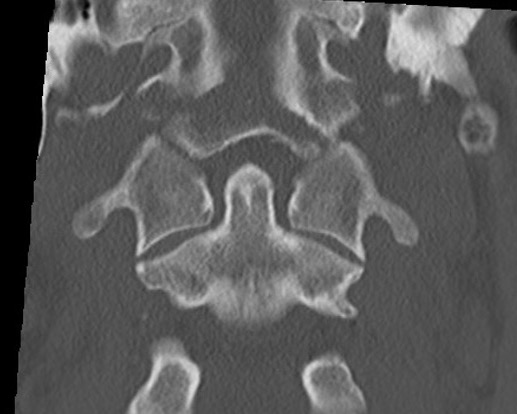
Type II: Basal skull involvement
Management
External immobilization
Musbahi et al Clin Neurol Neurosurg
- systematic review of 25 studies and 239 patients
- all treated in halo or collar for 3 months
- mortality rate 40% from other injuries
Maserati et al J Neurosurg Spine 2009
- follow up of 104 occipital condyle fractures
- occipital-cervical (C0-C3) fusion in 2 who had evidence of craniocervical malalignment
- remainder all treated with collar
- no late instability / malalignment / nerve compression
Type I / II
Stable
Collar
Type III
Issue
Potentially unstable
Fiester et al Eur Spine J 2021
- 34 patients with infero-medial Type III occipital condyle fracture
- MRI stable in all but one patient
Management
? Halo-thoracic brace
Outcomes
- 28 patients with occipital condyle fractures treated nonoperative
- mean Neck Disabilty Index was 14 (mild disability)
- headache most common symptom