

Definition
Malignant cartilage producing tumour
Epidemiology
Second most common primary malignant bone tumor after osteosarcoma
- 20 - 27%
Mean age 50 - 70% of patients > 40 at age of presentation
Male = Females
Location
Extremities 45%
- medullary canal metaphysis long bones
- proximal femur
Axial skeleton 31%
- 20% pelvis
Two Distinct Types
1. Primary Chondrosarcoma
Arises de novo
2. Secondary Chondrosarcoma (1/4)
Arises in existing cartilage lesion
- most common in osteochondromas / enchondromas
- also fibrous dysplasia / unicameral bone cyst / Paget's / post radiotherapy
Osteochondroma
< 1% solitary lesions
5% multiple lesions
Malignant features
- growth after skeletal maturity
- pain
- calcification in cartilage cap
- disappearance of previous calcification
- cartilage cap > 1-3 cm
- hot on bone scan
- erasure of smooth outline



Enchondroma
Malignant features
- endosteal scalloping
- size > 5 cm rarely benign (80% of enchondromas are < 2cm)
Grading
Conventional Chondrosarcoma
Grade 1 Low
Grade 2 Intermediate
Grade 3 High grade
Non conventional subtypes (10 - 15%)
Periosteal / clear cell / myxoid / mesenchymal / dedifferentiated
Clinical
Pain
- progressive
- at night
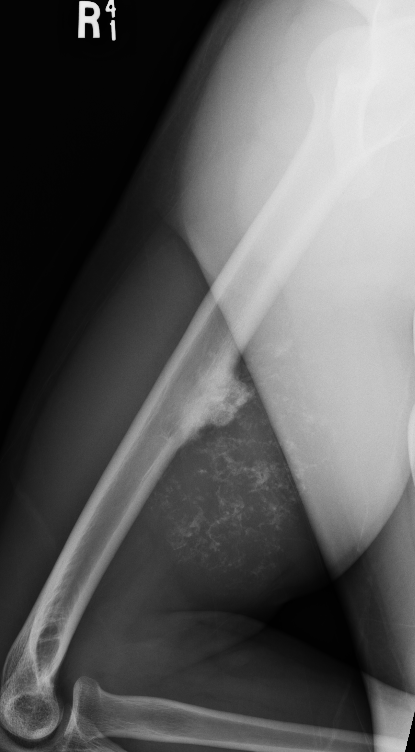
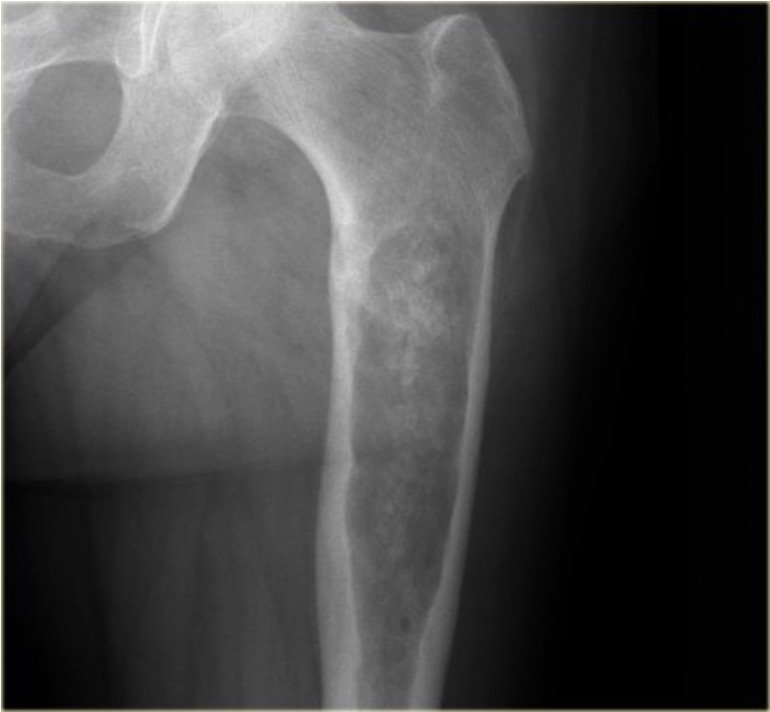
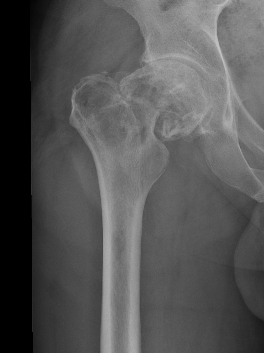
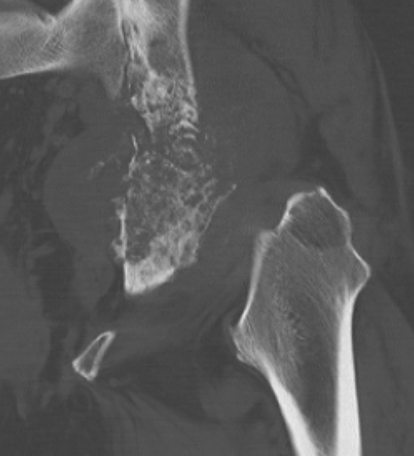
X-ray
Lytic lesion with punctate or spotty calcification
Worrisome features
- growth over time
- large > 5cm
- endosteal scalloping is hallmark of chondrosarcoma


Enchondroma enlarging over time


Large calcification with endosteal scalloping humerus
Large calcified lesion with endosteal scalloping

Pathological fracture
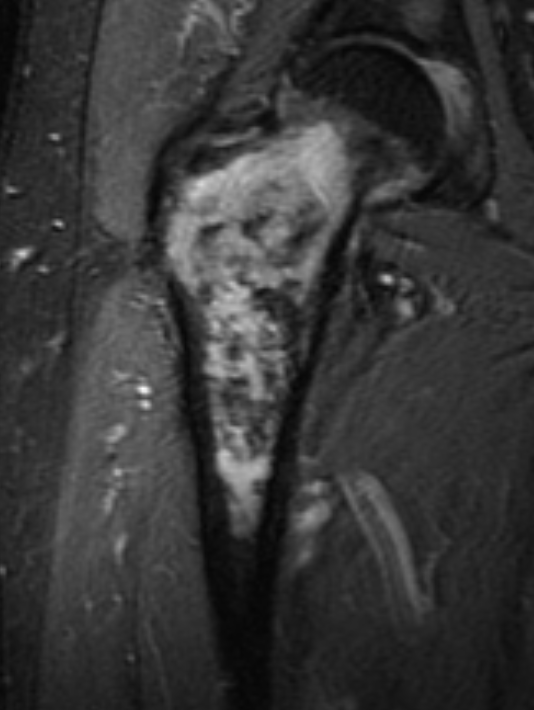
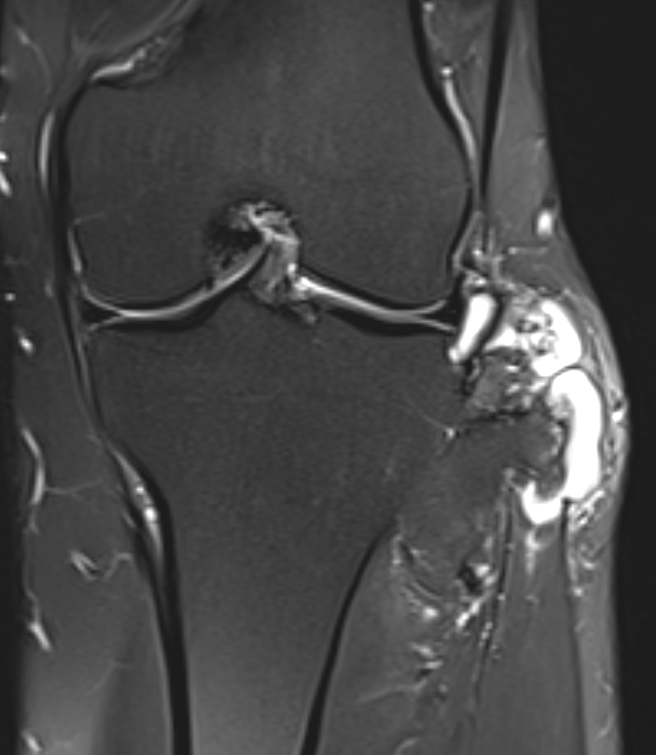
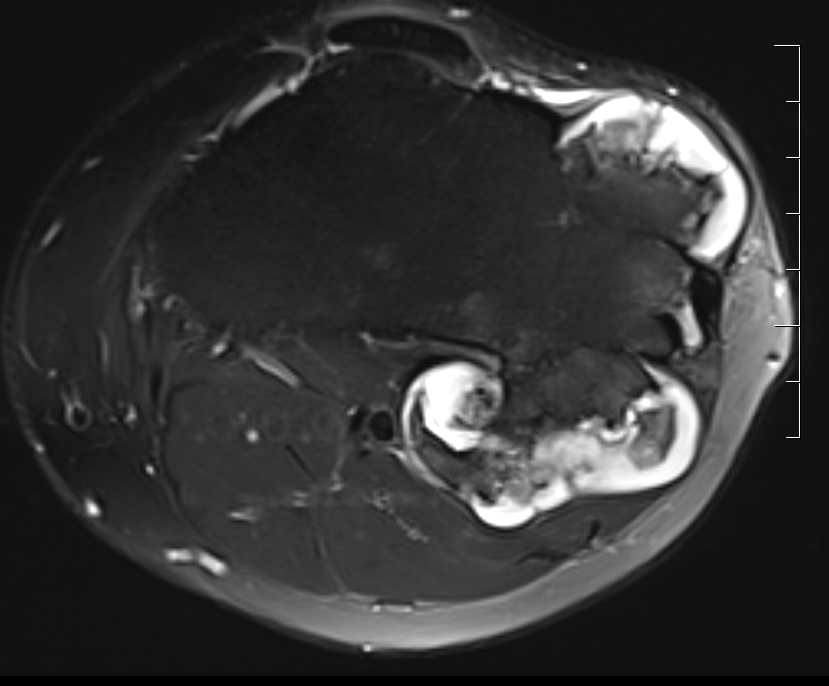
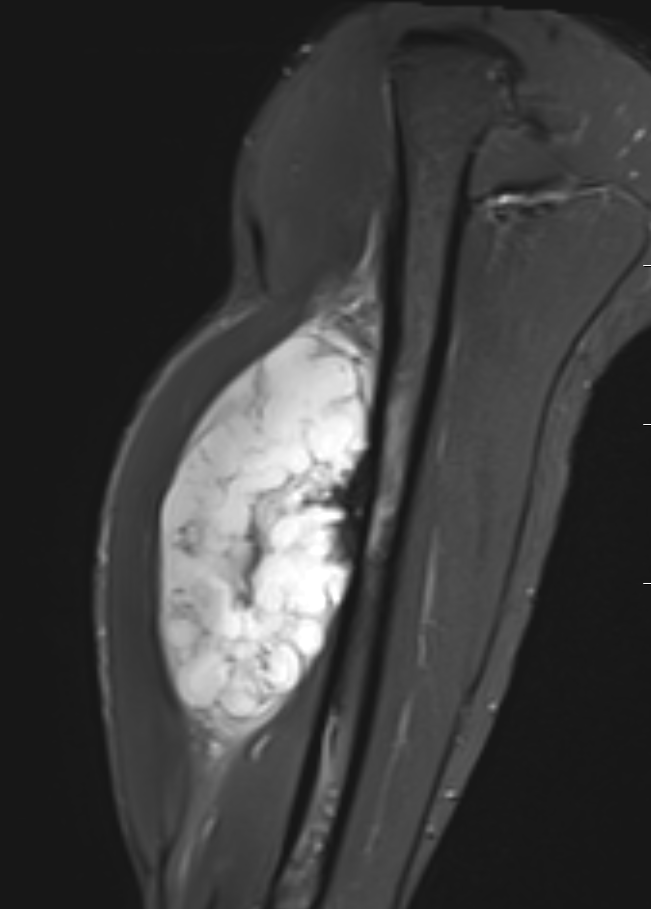
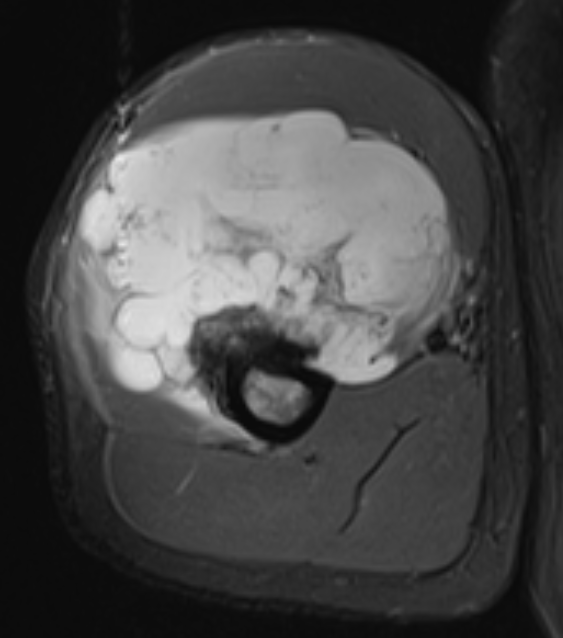
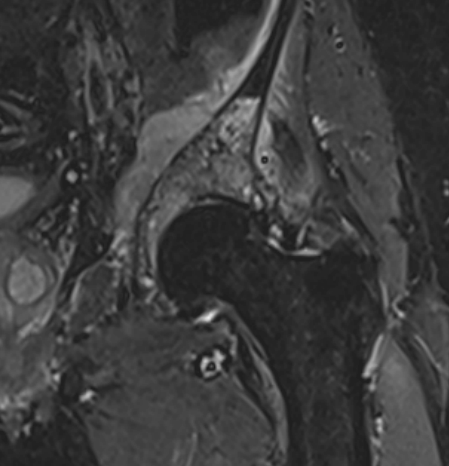
MRI
- MRI of 179 chondrosaroma
- features of high grade chondrosarcoma
- bone expansion, active periostitis, soft tissue mass and increased tumour length

CT

Histology
Lobules of hyaline cartilage
Features that suggest malignancy
- pleomorphism / hypercellularity / mitotic figures / double nuclei
Pathology outlines / chondrosarcoma
Biopsy
Accuracy
- accuracy of histological grading of biopsy versus samples from surgery
- 126 chondrosarcoma
- grouped into high versus low grade
- accuracy 90% in long bones
- accuracy 67% in pelvis
- accuracy of histological grading of biopsy versus samples from surgery
- 262 pelvic chondrosarcoma
- accuracy of biopsy in defining grade 37%
Reliability of histological grading
SLICED study group, JBJS Am 2007
- 9 pathologists viewing 46 biopsies / samples
- benign / low grade / high grade
- inter-rater reliability 0.4
Management
Principles
Resistant to chemotherapy / radiotherapy
- slow growing
- low vascularity
High grade
- wide resection
Low grade
- slow growing / low risk of of metastasis
- ? suitable for intra-lesional treatment
Dedifferentiated
- consider chemotherapy
Low grade / intralesional treatment
Technique
Cortical window
- burr / currette
- phenol / cryotherapy / liquid nitrogen
Results
Dierselhuis et al Cochrane Database Sys Review 2019
- intralesional treatment versus wide resection for low grade / Grade 1 chondrosarcoma long bones
- 14 studies and 511 participants
- 419 treated with intralesional treatment, 91 with wide resection
- no difference in recurrence free survival
- lower complication rates and better functional outcomes with intralesional treatment
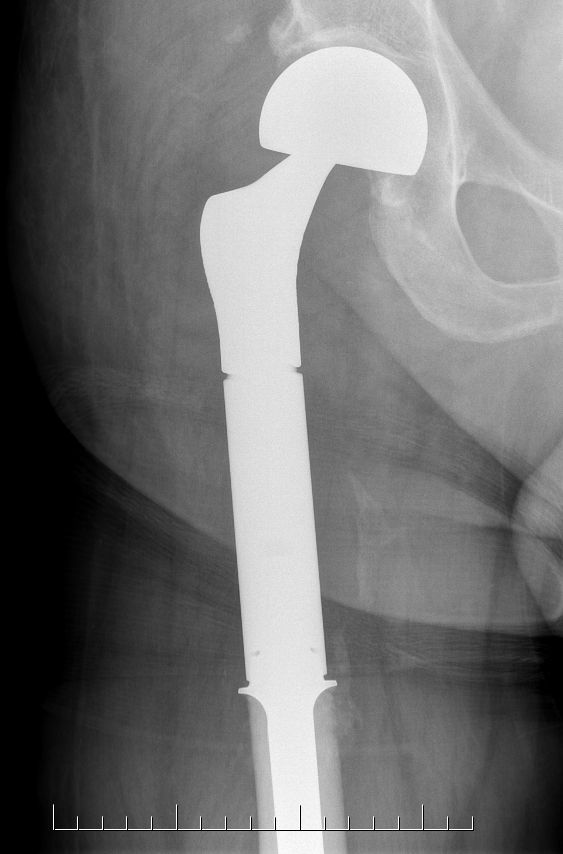
High grade / Wide resection





Pelvis
Issues
- low grade uncommon
- wide resection difficult

Wide resection
- hemipelvectomy
- hind quarter amputation (1% mortality)

Prognosis
Grade 1: >90% 5 year survival
Secondary chondrosarcoma: 90% 5 year survival
Grade 2: 75% 5 year survival
Grade 3: 30% 5 year survival
Factors
Histological grading
Surgical margins
- important as there is no adjuvant treatment
- more difficult in the pelvis
Histological grading
Fromm et al World J Surg Oncol 2019
- 37 patients with grade 1 chondrosarcoma
- 5 year survival 97%
- 10 year survival 92%
Dierselhuis et al Cochrane Database Sys Review 2019
- intermediate grade 10 year survival 53 to 64%
- high grade 10 year survival 29 to 38%
Amer et al J Orthop Research 2020
- Juxtacortical: 68% 5 year survival
- Clear-cell: 62% 5 year survival
- Myxoid: 50% 5 year survival
- Mesenchymal: 38% 5 year survival
- Dedifferentiated: 11% 5 year survival
- Chondrosarcoma secondary to osteochondroma
- 51 cases treated with wide resection
- 10 year survival 89%
- increased recurrence in pelvic tumours
Surgical margins
- 262 pelvic chondrosarcoma
- patients with > 1 mm resection 100% 10 year disease free survival
- patients with < 1 mm resection 52% 10 year disease free survival
Stevenson et al Eur J Surg Oncol 2018
- 341 cases chondrosarcoma
- surgical margin > 0.4 mm important at reducing local recurrence
- local recurrence associated with reduced survival in grade 2 and 3