

Epidemiology
Wrist and hand commonly affected in rheumatoid wrist (70%)
Overall, incidence of surgery in patients with RA reduced in the era of biological treatment
However, incidence of finger and wrist arthroplasty in RA increasing
- clinically silent synovitis
- patients want improved function
Pathology
Ulna sided synovitis
- volar subluxation of carpus and prominent ulna
- contributes to ulna sided extensor tendon rupture
ECU subluxaton - leads to radial deviation of wrist
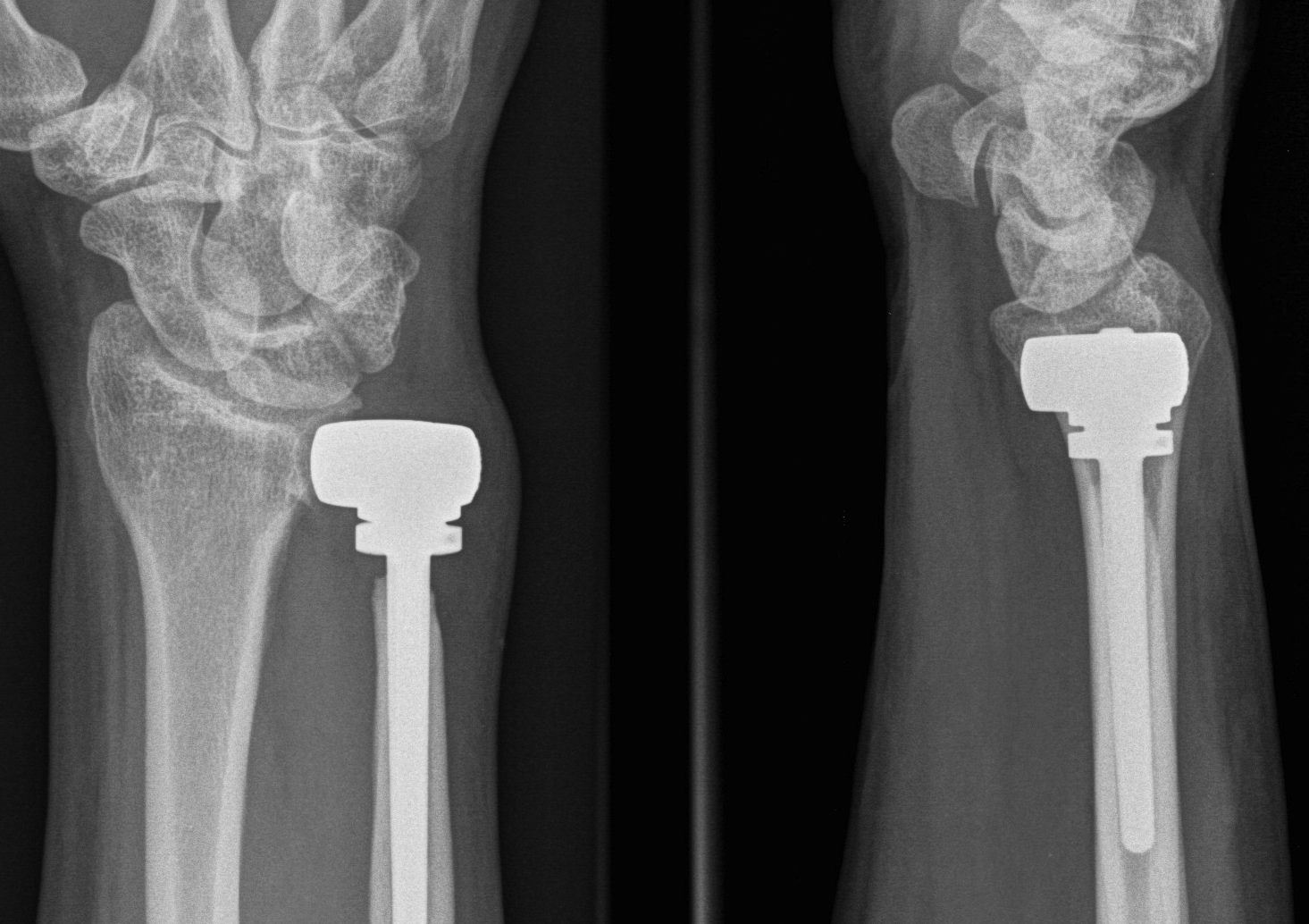
Xray


End stage rheumatoid arthritis of the wrist


End stage rheumatoid arthritis of the wrist
Operative Management
Clinical issues
DRUJ pathology - instability / arthritis
Extensor tendon rupture - repair / reconstruct
Flexor tendon rupture - repair / reconstruct
Wrist collapse / deformity - arthrodesis / arthroplasty
Synovectomy
Indications
Persistent painful wrist synovitis not settling with medical management
Minimal xray changes
Arthroscopic synovectomy
- arthroscopic synovectomy in 56 RA wrists with mean 8 year follow up
- 75% controlled synovitis
Vumedi arthroscopic wrist synovectomy video
Open technique
Dorsal approach
- 3/4 extensor compartment
- perform partial wrist denervation (PIN in floor of 4th extensor compartment)
- Berger ligament sparing arthrotomy (between DRC and DIC ligaments) / T shaped capsulotomy
- radiocarpal and midcarpal synovectomy
- DRUJ synovectomy +/- excision through longitudinal capsular incision
- ECRL to ECU transfer to prevent radial deviation
- repair extensor retinaculum underneath tendons to protect bed
Volar approach
- carpal tunnel decompression
- debride flexor tendons
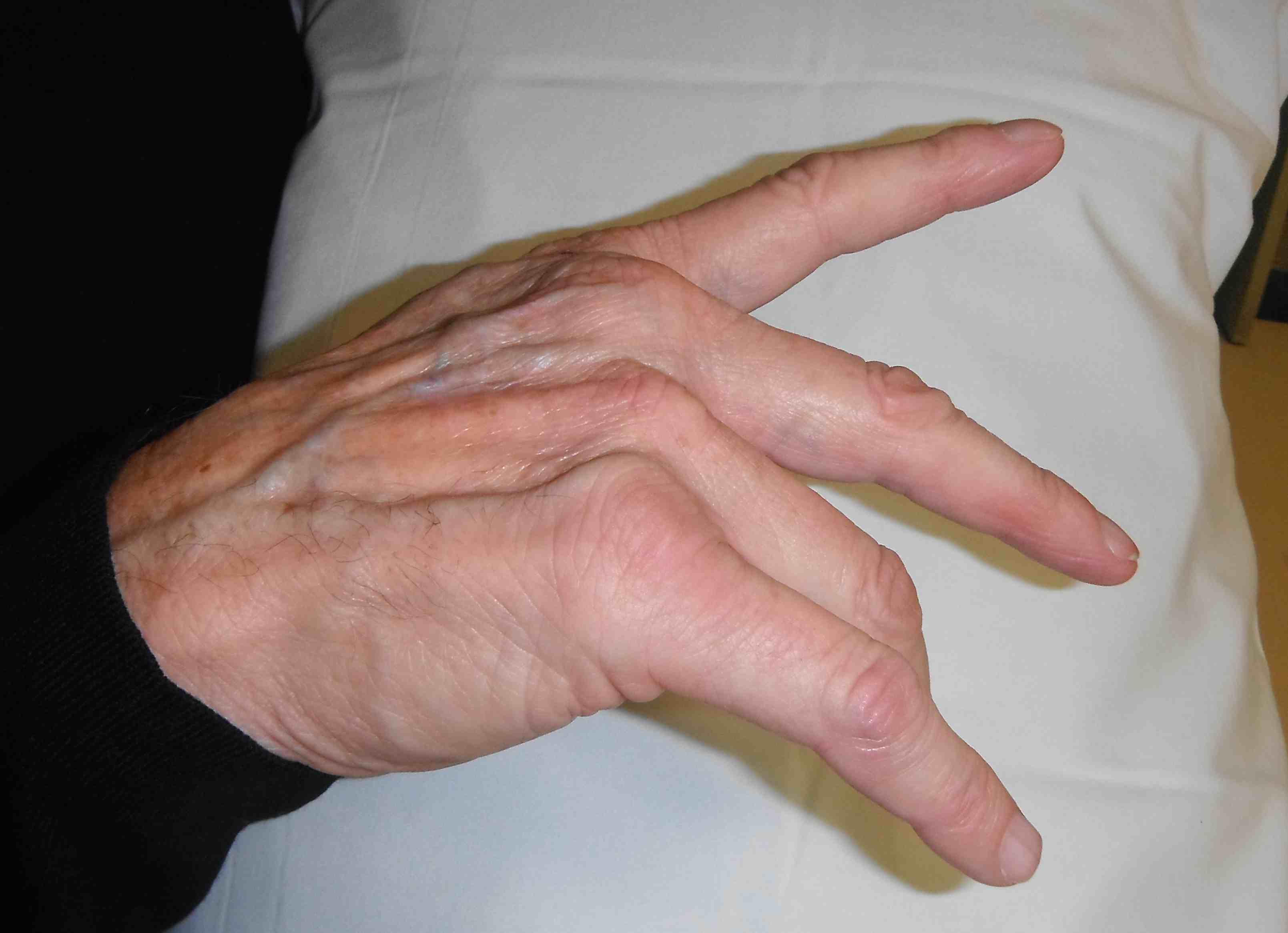
Extensor tendon rupture
Pathology
Dorsal synovitis / prominence of DRUJ
Extensor tendons rupture ulna to radial starting with little finger
- EDM > LF > RF > MF > IF > EIP
- opposite to flexor tendons
- extensor digiti minimi first (Vaughan-Jackson syndrome) - can be clinically silent due to action of EDC
EPL to thumb rupture also common
Differential diagnosis of dropped fingers
MCPJ and extensor tendon subluxation
PIN palsy at elbow
Tenodesis effect
- if extensor tendons intact
- passive wrist flexion causes finger extension


Tenodesis effect - passive flexion and extension of wrist does not cause finger extension / extensor tendons ruptured
Operative management
Options
Finger extensor tendons
- direct end to end repair - ? not indicated
- end to side suturing of adjacent extensor tendons
- interposition graft - palmaris longus
- tendon transfer - ECRL / FDS
Thumb
- EIP to EPL transfer
+/- synovectomy and address DRUJ
+/- wrist fusion
| Little finger rupture | Little and ring finger | Little / ring / middle finger | Little / Ring / Middle / Index finger |
|---|---|---|---|
|
Little finger - EDM to 4th EDC - end to side suture
|
Little finger - EIP to EDM - end to end
Ring finger - 4th EDC to 3rd EDC - end to side
|
Little / ring finger - EIP - end to end
Middle finger - middle to index - ERCL end to end |
Boyes procedure - Little / ring finger to ring FDS - Middle / index finger to middle finger FDS |
Technique
Vumedi EIP to EPL transfer video
Results
Suzuki et al Mod Rheumatol 2016
- 46 cases triple finger extensor tendon rupture
- free graft v end to end v EIP v combined end to side and EIP
- best results with combined end to side and EIP
Shin et al J Hand Surg Rehab 2020
- 51 rupture extensor tendons in RA
- direct repair v interposition graft
- reduced extensor lag with direct repair
Flexor tendon rupture
Epidemiology
Much less common than extensor tendon ruptures
Commonly affects FPL to thumb and FDP to index finger
Pathology


STT joint synovitis, subluxation and spurs
- causes attrition and rupture of adjacent flexor tendons
- FPL and FDP / FDS to index finger
Management
Technique
Carpal tunnel incision
- debride bone prominence
- flexor synovectomy
FPL rupture - fuse IPJ and transfer FDS index or ring finger
Index finger FDP - fuse DIPJ
Index finger FDP + FDS - fuse DIPJ and middle finger FDS transfer
Distal radio-ulna joint


Clinical
DRUJ subluxes dorsally
- pain with wrist rotation
- instability
Options

Darrach's procedure - resection distal ulna
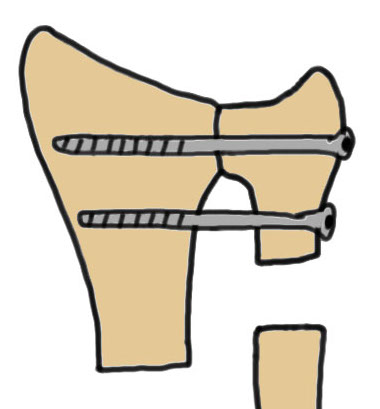
Suave - Kapandji - distal radio-ulna arthrodesis with screws + proximal ulna pseudoarthrosis
DRUJ replacement - hemiarthroplasty / total joint arthroplasty
Wrist arthrodesis / arthroplasty
Results
Darrach's versus Suave - Kapandji
Nakagawa et al Mod Rheumatol 2003
- 31 Darrach's versus 32 Suave - Kapandji in RA patients
- no difference in pain
- improved grip strength and reduced ulna wrist translocation SK procedure
DRUJ replacement
Galvis et al J Hand Surg Am 2014
- 17 patients with RA undergoing total DRUJ arthroplasty
- at 3 years follow up, 15/17 substantial pain relief
Techniques
www.boneschool.com/DRUJ-arthritis
Wrist arthritis
Options
Wrist arthrodesis - poor bone stock / significant defomrity
Wrist arthroplasty - adequate bone stock / minimal deformity
Results
Zhu et al J Hand Surg Eur 2021
- systematic review of arthrodesis v arthroplasty for end stage RA wrist
- 23 studies - 343 arthrodesis and 618 arthroplasty
- complication rate: arthrodesis 17%, arthroplasty 19%
Wrist arthrodesis


Technique
www.boneschool.com/wrist-arthrodesis
Results
Kluge et al J Hand Surg Am 2013
- 93 wrist fusion in RA with intramedullary rod
- 3rd metacarpal to distal radius
- good outcomes
Arboucalot et al Hand Surg Rehab 2020
- 101 radiolunate v 26 radioscapholunate arthrodesis in RA
- similar clinical outcomes
- nonunion: radiolunate 30% v radioscapholunate 62%
Total wrist arthroplasty
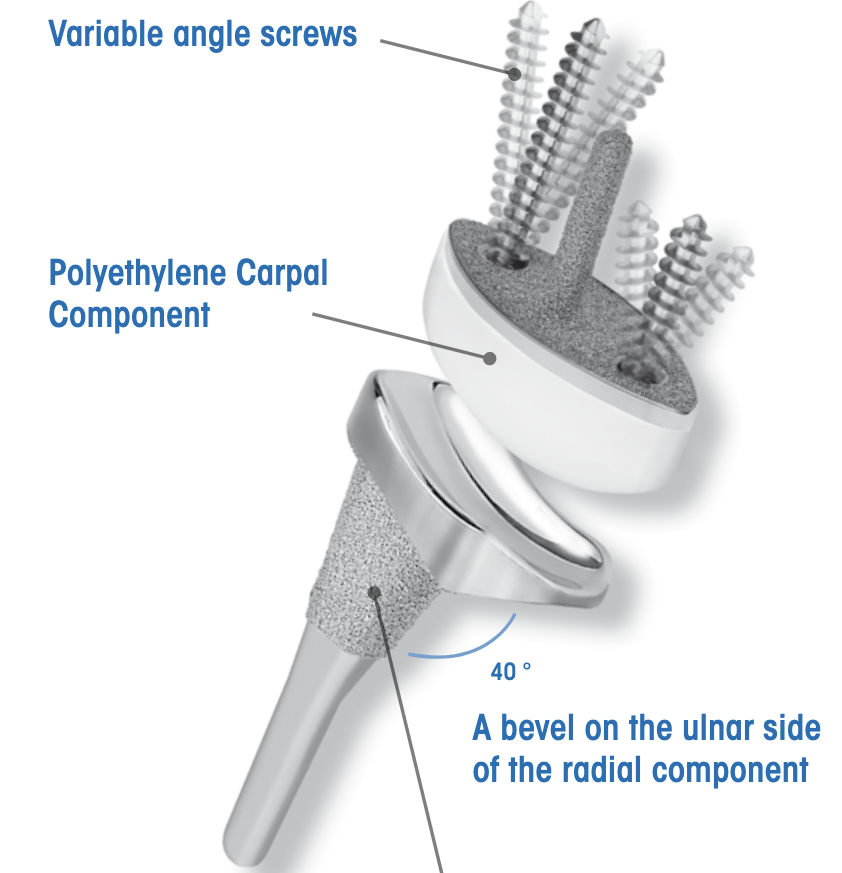
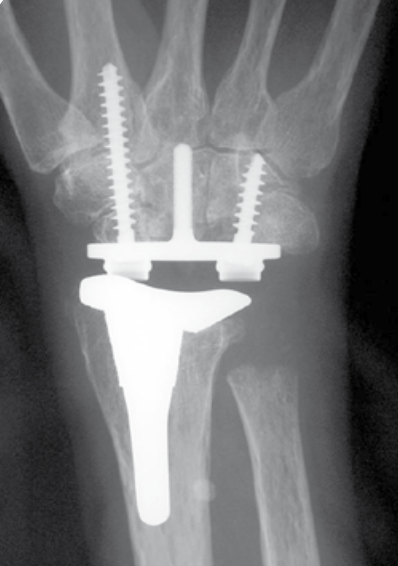
Universal 2 Total Wrist Implant system surgical technique PDF
Technique
www.boneschool.com/wrist-arthroplasty
Results
- 425 primary total wrist arthroplasty followed for mean 2 years
- 90% inflammatory arthritis
- intra-operative fractures 2%
- postoperative fractures 2%
- 88% 10 year survival