

Operative management
Indications
Difficulty with footwear
Pain
Lateral instability
Contra-Indications
Progressive deformity
Treatable spinal pathology i.e. syringomyelia
Algorithm
Stage 1 - flexible 1st metatarsal plantaflexion / shoe modification
|
Stage 2 Fixed first metatarsal / cavus Flexible hindfoot varus |
Stage 3 Fixed first metatarsal / cavus Fixed hindfoot varus |
Stage 4 OA / bony deformity |
|
|---|---|---|---|
| Forefoot cavus |
Steindler plantar fascia release 1st metatarsal osteotomy Claw toe surgery
|
Steindler plantar fascia release 1st metatarsal osteotomy Claw toe surgery
|
Triple arthrodesis Tarsal osteotomy |
| HIndfoot varus |
T posterior transfer - weak dorsiflexion P longus to P brevis transfer - weak eversion
|
Calcaneal osteotomy
|
|
Concept
Best to perform joint preserving surgery in young patients if possible
- 52 feet with CMT and cavovarus deformity
- compared joint preserving and joint sacrificing surgery
- joint preserving better functional outcomes and fewer complications
Stage 2: Fixed cavus with flexible hindfoot varus
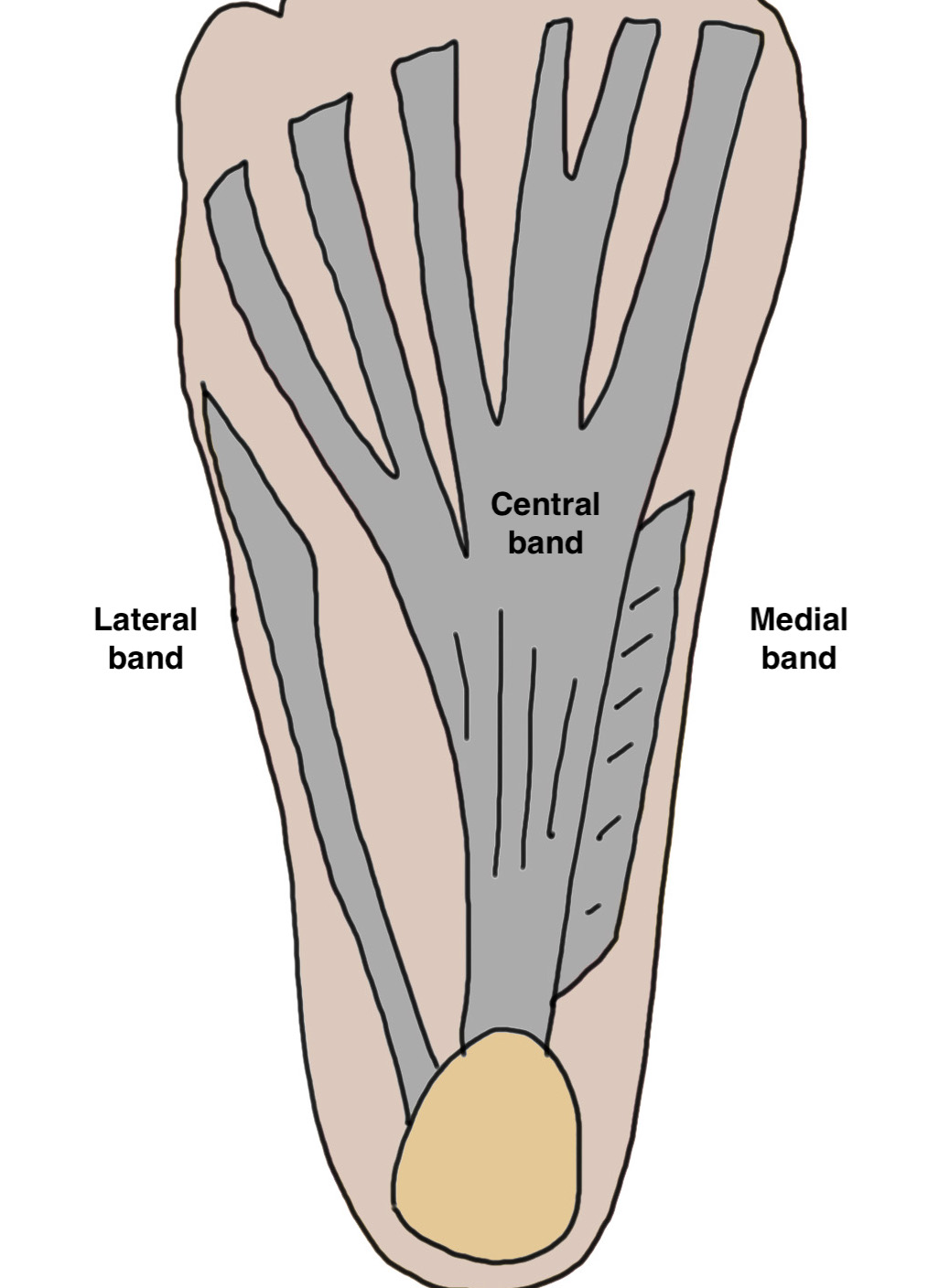
Steindler Plantar Fascia Release
Open Technique
Vumedi open plantar release video
Longitudinal medial incision
- 2-3 cm at plantar aspect of calcaneal insertion
- open medial fascia
- reflect abductor hallucis dorsally
- separate above and below fascia
- release plantar fascia at insertion of calcaneum
- lateral plantar nerve is at lateral edge of fascia
Arthroscopic technique
Arthrex endoscopic plantar fascia release
First metatarsal extension osteotomy


Indication
- incomplete correction of first ray
- mature patient with closed physis
Technique
Dorsal closing wedge osteotomy
- base of metatarsal
- leave plantar surface intact
- 3-4 mm wedge
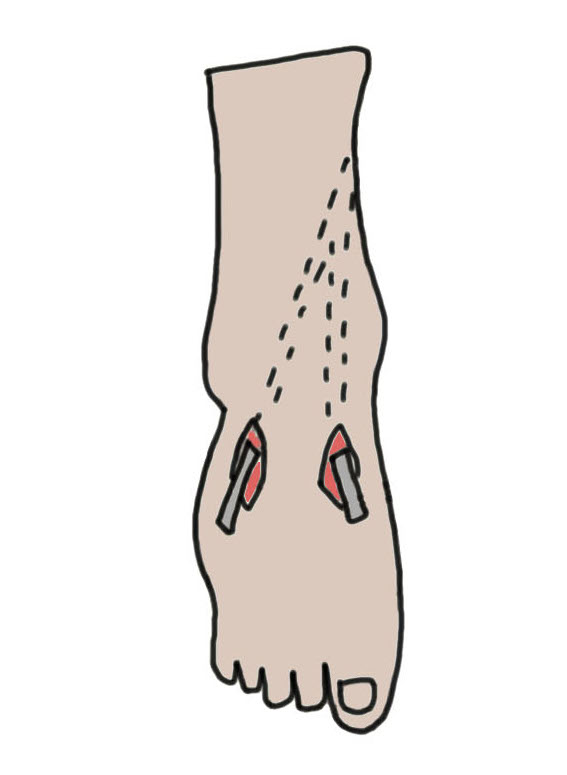
Tibialis Posterior transfer and medial soft tissue release
Indication
Weak dorsiflexion / dropfoot
Technique
Vumedi tibialis poterior tendon transfer
Dorsomedial incision
- release T posterior from insertion on navicular
Medial soft tissue release
- release talonavicular joint and spring ligament
Proximal medial calf incision
- retrieve T posterior tendon
- pass anteriorly through interosseous membrane
Dorsolateral / Dorsomedial incision
- tunnel T posterior tendon under skin
- pulvetaft to T anterior +/- P brevis (split T posterior transfer)
Results
- tibialis posterior transfer for dropfoot in 23 feet with CMT
- results in active dorsiflexion
P longus to P brevis transfer
Indications
Weak eversion
Technique
Vumedi P long to brevis transfer technique
Lateral incision over peroneal sheath
- protect sural nerve
- P longus plantar, P brevis dorsal
- suture P longus to P brevis distally
- release P longus proximally and pulvetaft through P brevis
Great Toe Clawing
Hyperextension MTPJ / Flexion IPJ
Jones procedure
- IPJ fusion
- EHL tendon transfer
Lesser Claw Toes
Flexible Girdlestone FETT
Fixed Extensor Tenotomy / PIPJ fusion / MTPJ dorsal capsulotomy / Weil's osteotomy
+/- Tendo achilles lengthening +/- Lateral Ligament reconstruction
Results
Leeuwesteijn et al Foot Ankle Surg 2010
- 33 patients with CMT, pes cavus, and flexible hindfoot varus
- treated with 1st metatarsal osteotomy / soft tissue release / tendon transfers
- recurrence of cavus in 2 patients - treated with triple arthrodesis
Ward et al JBJS Am 2008
- 41 feet with cavovarus feet and CMT
- metatarsal osteotomy, plantar fascia release, P longus transfer, Jones procedure, +/- T anterior transfer
- correction cavus well maintained
- most patients some recurrence hindfoot varus
Stage 3: Fixed cavus + fixed hindfoot varus
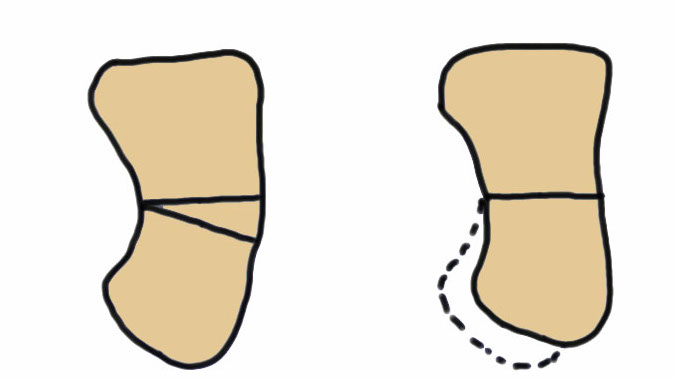
Dwyer lateral closing wedge calcaneal osteotomy
Indication
Fixed hindfoot varus
Technique
Video Dwyer calcaneal osteotomy
Lateral approach
- posterior and inferior to peroneal tendons
- resect lateral wedge of bone
- reduce calcaneal ostoeotmy and fix with screws
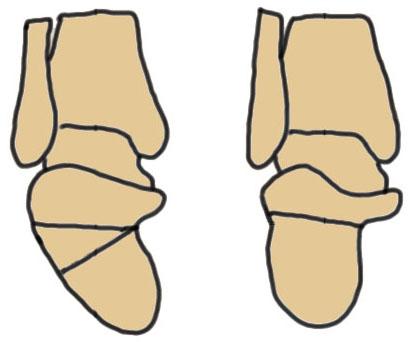
Lateral displacement calcaneal osteotomy


Technique
Lateral approach
- curve just behind peroneals
- homann in front of tendoachilles
- homann under calcaneum
Oblique osteotomy behind posterior facet
- 45o
- open with lamina spreader
- split periosteum medially with osteotome
- avoid damage to medial structures
- transfer laterally 1 cm
- screw fixation
Stage 4: Bony deformity / salvage
Triple Arthrodesis
Meary closing wedge tarsectomy
Indication
Fixed deformity, difficult cases
Results
Simon et al Foot Ankle Surg 2019
- tarsectomy / calcaneal osteotomy / metatarsal osteotomy in 26 feet
- good results 58%
- fair results 23%
- poor results 19%